
Abstract
Background:
Patients often sustain prolonged neuromuscular dysfunction after anterior cruciate ligament reconstruction (ACLR). This dysfunction can present as interlimb loading rate asymmetries linked to reinjury and knee osteoarthritis progression.
Purpose/Hypothesis:
To evaluate how asymmetric walking protocols can reduce interlimb loading rate asymmetry in patients after ACLR. It was hypothesized that asymmetric walking perturbations would (1) produce a short-term adaptation of interlimb gait symmetry and (2) induce the temporary storage of these new gait patterns after the perturbations were removed.
Study Design:
Descriptive laboratory study.
Methods:
Fifteen patients who had undergone ACLR were asked to perform an asymmetric walking protocol during the study period (2022-2023). First, to classify each limb as overloaded or underloaded based on the vertical ground-reaction force loading rate for each limb, participants were asked to perform baseline symmetric walking trials. Participants then performed an asymmetric walking trial for 10 minutes, where one limb was moving 0.5 m/s faster than the other limb (1 vs 1.5 m/s), followed by a 2-minute 1 m/s symmetric deadaptation walking trial. This process was repeated with the limb speeds switched for a second asymmetric trial.
Results:
Participants adopted a new, symmetric interlimb loading rate gait pattern over time in response to the asymmetric trial, where the overloaded limb was set at 1 m/s. A linear mixed-effects model detected a significant change in gait dynamics (P < .001). The participants exhibited negative aftereffects after this asymmetric perturbation, indicating the temporary storage of the new gait pattern. No positive short-term gait adaptation or storage was observed when the overloaded limb was set to a faster speed.
Conclusion:
Asymmetric walking successfully produced the short-term adaptation of interlimb loading rate symmetry in patients after ACLR and induced the temporary storage of these gait patterns in the initial period when the perturbation was removed.
Clinical Relevance:
These findings are promising, as they suggest that asymmetric walking could serve as an effective gait retraining protocol that has the potential to improve long-term outcomes in patients after ACLR.
Anterior cruciate ligament (ACL) ruptures—occurring in 250,000 Americans each year—are common among young athletes. 13 These ruptures are often treated by undergoing ACL reconstruction (ACLR) and rehabilitation to restore healthy, symmetric limb loading to limit reinjury upon return to sports.10,13,19,24,27 Yet, even with current rehabilitation practices, patients can continue to have prolonged neuromuscular dysfunction and impaired proprioception after ACLR.10,27 These impairments in muscle activation and the ability to sense where their limb is in space hinder the adaption and storage of healthy limb loading dynamics.10,24,27 A measurable consequence of these deficits is interlimb loading rate asymmetry that contributes to the development of knee osteoarthritis (OA).1,3,7,14-16,18,21 While rehabilitation programs have been successful in overriding these deficits to restore symmetric muscle strength, lingering dynamic interlimb gait asymmetries often remain.2,5,6,10 Thus, this suggests that alternate rehabilitation strategies are needed to produce the adoption and storage of healthy symmetric loading rate dynamics to help improve long-term outcomes in patients after ACLR.
Reducing gait asymmetry in patients experiencing neuromuscular dysfunction is a challenge. However, great strides have been achieved in stroke rehabilitation. Stroke research has highlighted the potential of purposely induced asymmetric gait perturbations, where one limb is set at a different speed from the other to stimulate positive gait adaptation and restore interlimb gait symmetry.4,11,20,23,26 Reisman et al 22 showed that a 0.5 m/s asymmetric gait perturbation was effective in reducing interlimb step length and double support time asymmetry in the short term in patients after stroke, while Roper et al 24 utilized asymmetric walking to modify interlimb spatiotemporal gait dynamics in patients after ACLR. This work was significant because it indicated how asymmetric walking could override patients’ diminished neuromuscular drive to adopt new gait dynamics after ACLR.
Interlimb loading rate asymmetry is detrimental to knee health and contributes to the initiation and progression of posttraumatic osteoarthritis (PTOA) after ACLR.1,3,12,14-16,18,19,21 Thus, implementing the asymmetric walking protocol provides a unique opportunity to combat a serious issue in this population. To maximize the effectiveness of the asymmetric walking protocol, it is important to set each limb at the correct speed. Reisman et al 22 found that limb speed selection depends on patients’ initial gait asymmetry, as it represents their gait impairment. Given that higher loads and loading rates have been measured in both the reconstructed and nonreconstructed limbs in patients who had ACLR, it supports the idea that limbs should be grouped by neuromuscular function and not surgical status (ie, reconstructed vs nonreconstructed).2,5,6,8,9,17 Therefore, when considering the gait adaptations associated with an asymmetric walking protocol for patients who had undergone ACLR, it is critical to determine the proper limb speed selection to promote positive adaptation. However, that decision may not depend solely on the surgical status of the patient’s limbs.
In the present study, we sought to expand on previous work to examine how asymmetric walking could promote the adoption and storage of interlimb loading rate symmetry in patients who had ACLR. It was hypothesized that (1) purposely induced asymmetric gait perturbations would cause short-term adaptations in limb loading rate in patients after ACLR and that (2) the reduced limb loading asymmetry in these patients would remain temporarily after the perturbation is removed. The findings from this study could support the use of asymmetric walking as a potential gait retraining method to correct gait asymmetry and limit knee OA progression to help improve long-term outcomes after ACLR.
Methods
Study Participants
The study protocol received institutional review board approval, and all participants provided written informed consent. In this study, 9 women and 6 men (N = 15) who had undergone ACLR—mean (± SD) age, 21.5 ± 3 years; height, 1.7 ± 0.1 m; mass, 73.3 ± 16.4 kg; time since reconstruction, 42 ± 28 months; and graft type, 7 hamstrings, 7 patellar tendons, 1 quadriceps—were included in the data collection between 2022 and 2023.
Prescreening
All study participants underwent a prescreening process to identify those with interlimb loading rate differences. During the prescreening test, participants performed 2 symmetric walking tasks, at 1 and 1.5 m/s, respectively, for 3 minutes each. Interlimb differences were classified as either overloaded or underloaded. The limb that produced the higher loading rates at both 1 and 1.5 m/s was defined as the overloaded limb, while the limb that had the lower loading rates was defined as the underloaded limb. The limb loading rate and interlimb loading rate differences were measured for each participant during symmetric walking trials. All participants in this study exhibited significant interlimb differences of at least 5% in the 1 m/s trial and 10% in the 1.5 m/s trial.
Instrumented Asymmetric Walking Protocol
Participants were asked to perform the asymmetric protocol during a single session (Figure 1). Participants performed the protocol on a split-belt instrumented treadmill (Bertec). Ground-reaction forces recorded by the instrumented treadmill were collected at 1200 Hz. An initial 5-minute warm-up walking trial was conducted to allow participants to become acclimated to the equipment (Figure 1). For the first recorded trial, the participants performed a symmetric walking trial at a set speed of 1 m/s, followed by a symmetric walking trial set at 1.5 m/s (Figure 1). Data were collected for 3 minutes for each of the symmetric trials. Next, participants completed the first of 2 asymmetric trials. Each asymmetric trial had a between-limb difference in speed of 0.5 m/s, with one limb set at 1 m/s and the other limb set at 1.5 m/s. There were 2 conditions for the asymmetric walking protocol—condition 1, in which the overloaded limb was set at 1 m/s, and the underloaded limb was set at 1.5 m/s; condition 2, in which the overloaded limb was set at 1.5 m/s, and the underloaded limb was set at 1 m/s. The order in which the limb was set at the faster speed during the asymmetric walking trials was randomized. To evaluate changes in loading rate between the overloaded and underloaded limbs over time, participants were asked to perform the asymmetric walking trials for 10 minutes. Each asymmetric walking trial was followed by a 2-minute symmetric walking deadaptation trial to normalize the participant’s gait before completing the subsequent asymmetric trial (Figure 1). Once participants finished the second deadaptation trial, they had completed the protocol.

Schematic of the asymmetric walking protocol performed by patients who had ACLR. The adaptation trials represent the 10-minute asymmetric walking trials with an interlimb gait speed difference of 0.5 m/s between the overloaded and underloaded limbs. Each asymmetric adaptation trial is followed by a symmetric deadaptation trial. ACLR, anterior cruciate ligament reconstruction.
Data Processing and Feature Extraction
The ground-reaction force data were collected from the instrumented treadmill and filtered using a zero lag, fourth-order, lowpass Butterworth filter with a 35 Hz cutoff frequency in Vicon Nexus (Vicon Motion Systems). The mean loading rate was extracted from the stance phase of the vertical ground-reaction force gait data using a custom MATLAB code (MATLAB R2019a; The MathWorks). The loading rate is a measure of force production over time and was determined by dividing the first peak ground-reaction force by the time to reach the first peak from the initial impact. The loading rate was extracted for each limb to allow for interlimb comparisons.
Statistical Analysis
The 2 asymmetric trials and their corresponding symmetric deadaptation trials served as the trials of interest, as they captured the adaptive behavior of the patients after ACLR during the protocol. The mean loading rates for each minute of the asymmetric and deadaptation trials were plotted over time for each participant to demonstrate loading rate progression. A mixed-effects model was fit to the mean minute-to-minute loading rate data to determine whether patients who had ACLR adopted new loading rate behavior during the asymmetric walking protocol. The interlimb difference (overloaded limb–underloaded limb) served as the model response variable, while the fixed factor was time, and the random factor was the participant number. A test of fixed effects was performed on the model to determine whether the fixed factor (time) produced a significant change in the response variable (difference in loading rate). A significant change in this response variable over time would indicate the presence of adaptive behavior. The threshold for significance was set at P < .05.
A Tukey pairwise comparison was conducted to evaluate the mean minute-to-minute loading rate data to identify when a new loading rate behavior was adapted during the asymmetric walking protocol. The statistical analyses were performed using RStudio (RStudio; Integrated Development Environment for R. RStudio).
A power analysis was performed to determine the sample size based on early results from pilot data. For a linear mixed-effects model that uses time as the fixed factor to predict loading rate difference, a power analysis determined that 13 participants would provide a power of 80% to detect a significant change in loading rate difference over time using a small effect size of 0.1.
Results
Prescreening: A Loading Rate-Based Approach for Characterizing Gait Asymmetry
A comparison of interlimb differences in loading rate indicated that the differences were the largest when comparing the overloaded and underloaded limbs loading rates in patients who had ACLR (Table 1). The loading rates were significantly greater in the overloaded limb in both the symmetric 1 m/s (P = .005) and 1.5 m/s (P < .001) walking trials (Table 1). A minimal nonsignificant difference of only 0.1 body weight per second (BW/s) was measured between the reconstructed and nonreconstructed limbs during both the symmetric 1 m/s (P = .24) and 1.5 m/s (P = .48) walking trials (Table 1). Thus, all subsequent study analyses were performed by examining the loading rate dynamics in the overloaded and underloaded limbs.
Limb and Interlimb Loading Rate Differences for the Overloaded and Underloaded Limbs and Reconstructed and Nonreconstructed Limbs During the Baseline Symmetric Walking Trials a

Data are reported as mean ± SD. BW, body weight.
Adoption of Interlimb Loading Rate Symmetry Over Time in Response to Asymmetric Walking Perturbation
The interlimb difference in loading rate was significantly reduced in response to the asymmetric walking perturbation during condition 1—when the overloaded limb was set to the slower 1 m/s speed, and the underloaded limb was set to the 1.5 m/s (Table 2). The graphical representation of the mean minute-by-minute loading rate demonstrates how the overloaded and underloaded limbs converged to the same loading rate over 10 minutes during condition 1 (Figure 2A). An assessment of the interlimb loading rate differences indicated that patients who had ACLR had adopted symmetrical limb loading rate dynamics by the end of the 10-minute trial when the overloaded limb was set as the slower speed (Figure 2C; Table 2). The convergence of the overloaded and underloaded limbs was supported by the results of the linear mixed-effects model (R2 = 0.81), as it indicated that the interlimb difference decreased significantly over time (P < .001) (Table 3). Furthermore, it was revealed that patients who had ACLR reduced the loading rate in the overloaded limb when it was set at a slower speed. Thus, eliminating the interlimb difference suggests that patients who had ACLR adopted a symmetric interlimb loading rate pattern over time.
Comparison of Interlimb Differences in Loading Rate for Each 10-minute Asymmetric Walking Trial a

Data are reported as means. The interlimb difference was calculated as an overloaded limb—underloaded limb. Values with different superscripts denote significantly different mean interlimb difference based on Tukey pairwise comparisons for the mixed effects model of each trial.
Overloaded, 1 m/s and underloaded, 1.5 m/s.
Overloaded, 1.5 m/s and underloaded, 1 m/s.
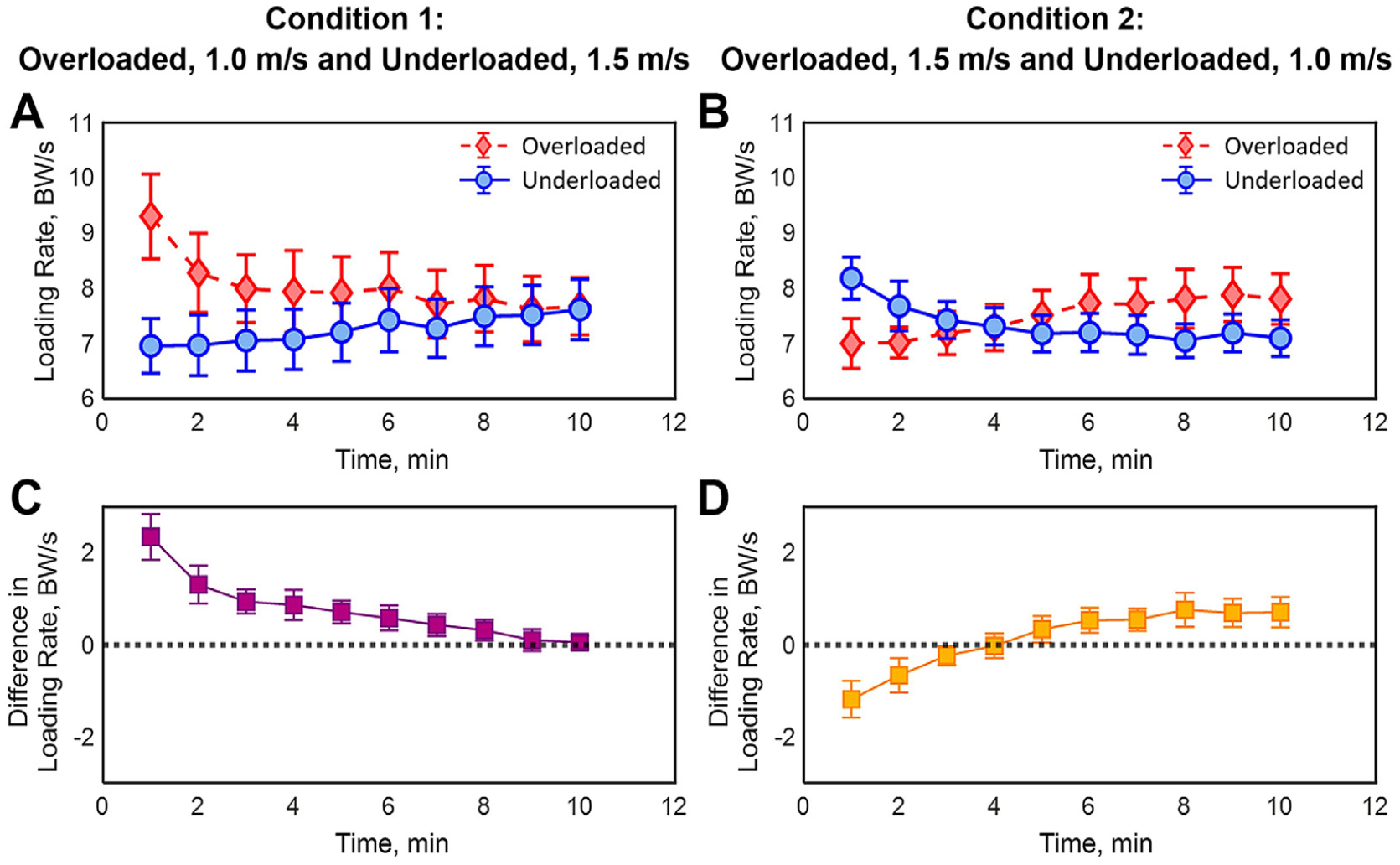
Comparison of the mean minute-by-minute loading rates for the overloaded and underloaded limbs during the two 10-minute asymmetric walking trials. (A) The loading rate over time during asymmetric condition 1—overloaded limb set as the slower 1 m/s speed. (B) The loading rate over time during asymmetric condition 2—overloaded limb set as the faster 1.5 m/s speed. (C) The difference in loading rate between the overloaded and underloaded limbs during condition 1. (D) The difference in loading rate between the overloaded and underloaded limbs during condition 2. Error bars represent standard deviations. BW, body weight.
Linear Mixed-Effects Models of the Interlimb Difference in Loading Rate for Both Asymmetric Trials

Overloaded, 1 m/s and underloaded, 1.5 m/s (R2 = 0.81).
Overloaded, 1.5 m/s and underloaded, 1 m/s (R2 = 0.85).
When the overloaded limb was set at the faster 1.5 m/s speed (condition 2), the mean minute-by-minute loading rate data showed that the 2 limbs initially converged to the same value around 4 minutes before diverging and resulting in a final interlimb difference of 0.6 BW/s after 10 minutes (Figure 2B; Table 2). The linear mixed-effects model (R2 = 0.85) fit to this data confirmed that the interlimb difference in patients who had ACLR significantly changed over time in response to condition 2 (P < .001) (Table 3). During this asymmetric condition, the overloaded limb increased its loading rate over time, while the underloaded limb decreased its loading rate over time. Patients who had ACLR produced a new interlimb loading rate pattern in response to the asymmetric walking condition 2.
Aftereffects of Asymmetric Walking Protocols
Patients who had ACLR showed no significant difference in interlimb loading rate at the end of the deadaptation period after the asymmetric walking condition where the overloaded limb was set to the slower speed (P = .21) (Table 4; Figure 3, A and C). The magnitude of the difference in loading rate at the end of the 2-minute deadaptation period was the same as the baseline but led to a decrease in loading in the overloaded limb (Table 4 and Figure 3, A and C). The change in the pattern of the difference in loading rate indicates that patients who had ACLR modified their limb loading dynamics even after the asymmetric walking perturbation was removed. Moreover, the overloaded limb did not revert to the elevated loading rate values exhibited during the baseline assessment. The analysis of the aftereffects suggests that patients who had undergone ACLR adopted and stored positive adaptive limb-loading behavior in response to this asymmetric walking condition.
The Difference in Loading Rate for the Symmetric Baseline Trials and the First 2 Minutes of Symmetric Deadaptation Trials that Occurred Immediately After Asymmetric Walking a

Data are reported as mean ± SD. Bold P values indicate significance. BW/s, body weight/second.
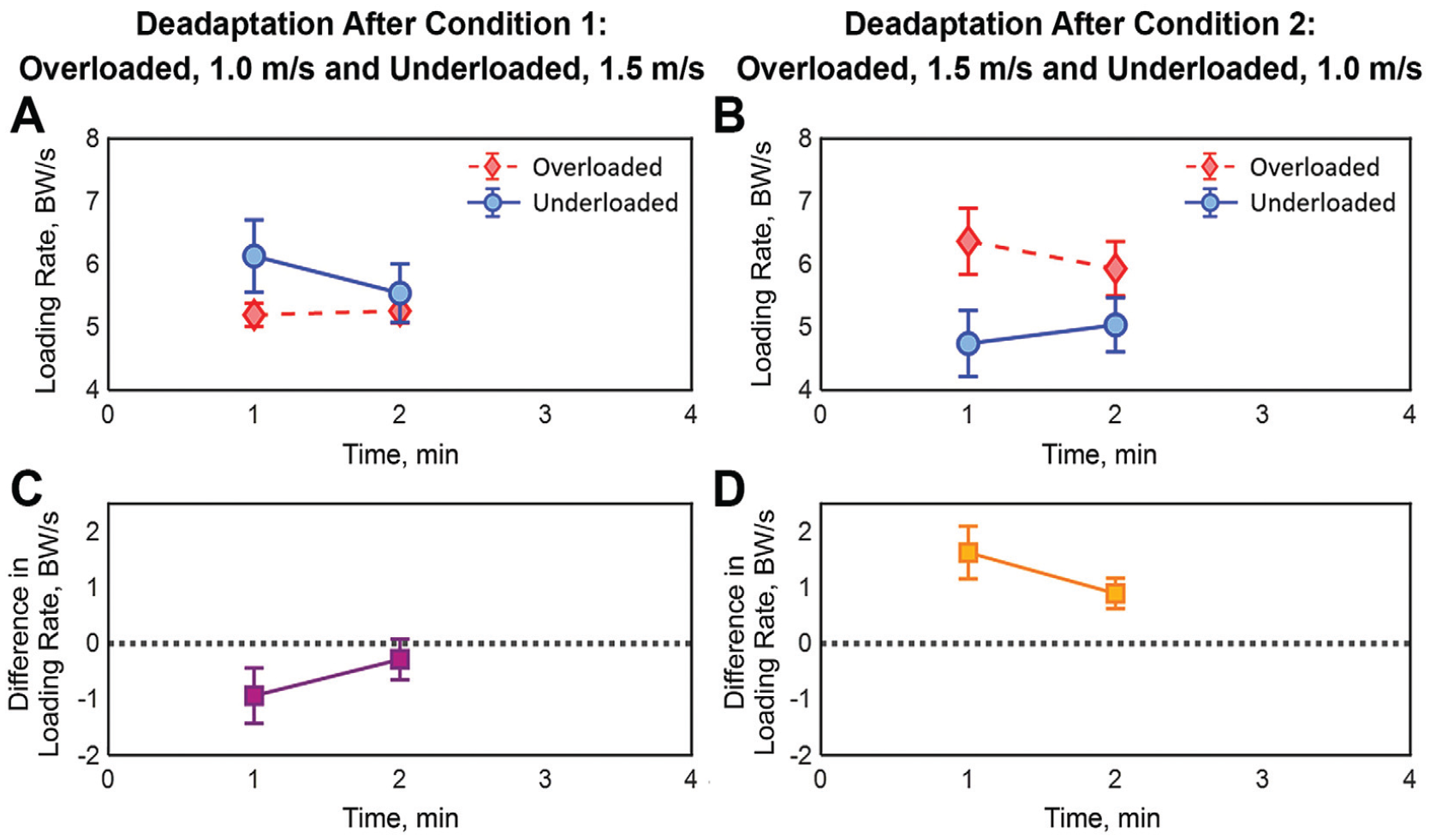
Comparison of the mean minute-by-minute loading rates for the overloaded and underloaded limbs during the two 2-minute symmetric deadaptation walking trials. (A) Loading rates over time during the symmetric deadaptation trial after asymmetric condition 1—overloaded limb set as the slower 1 m/s speed. (B) Loading rates over time during the symmetric deadaptation trial after asymmetric condition 2—overloaded limb set as the faster 1.5 m/s speed. (C) The difference in loading rate between the overloaded and underloaded limbs during the deadaptation after condition 1. (D) The difference in loading rates between the overloaded and underloaded limbs during the deadaptation after condition 2. Error bars represent standard deviations. BW, body weight.
The interlimb difference did increase at the end of the symmetric deadaptation period after the asymmetric walking condition in which the overloaded limb was set to the faster 1.5 m/s speed (0.7 BW/s) when compared to the baseline assessment (0.3 BW/s). A significant interlimb difference was present at the end of the trial (P < .001) (Table 4; Figure 3, B and D). The analysis of the aftereffects indicated that patients who had undergone ACLR did not eliminate their interlimb loading rate asymmetry in response to the asymmetric walking trial where the overloaded limb was set at the faster speed.
Discussion
The study successfully utilized a purposely applied asymmetric walking perturbation to adopt and store interlimb loading rate symmetry in the short-term in patients who had ACLR. These patients adapted new interlimb loading dynamics in response to both asymmetric walking protocols. However, interlimb loading rate asymmetries significantly decreased over time in response to a prolonged 10-minute exposure to the asymmetric walking perturbation, where the overloaded limb was set to the slower 1 m/s speed. Furthermore, the analysis of the aftereffects determined that patients who had ACLR temporarily stored the healthy limb loading behavior, as their interlimb loading rate difference during the symmetric deadaptation trial fell below their interlimb difference measured during the initial baseline assessment. The ability of these patients to even temporarily adopt and store healthy limb loading dynamics highlights the potential of the targeted asymmetric walking approach to serve as a gait retraining tool to help restore healthy gait dynamics and possibly limit the progression of knee PTOA in patients who had ACLR.
This study adopted an alternate approach to characterize and analyze interlimb gait asymmetry in patients after ACLR. Instead of the traditional comparison of reconstructed to nonreconstructed limbs, the study compared the overloaded and underloaded limbs previously introduced by Blackburn et al.2,14,17,18,24 This classification strategy proved useful, as it uncovered underlying loading asymmetries in this population of patients who had undergone ACLR that would not have been revealed using the traditional reconstructed and nonreconstructed limb designations. Furthermore, the overloaded designation was critical, as it helped inform which limb should be set at the faster speed during the asymmetric walking perturbation.
The 2 asymmetric walking protocols elicited different adaptive responses in patients who had ACLR. Their adaptive responses were found to be highly dependent on the perturbation direction—that is, which limb was set at the faster or slower speed. In the case in which the overloaded limb was set at the slower speed, both limbs converged to the same loading rate after 8 minutes and maintained their interlimb symmetry for the duration of the trial. This positive adaptive behavior suggests that patients who had ACLR utilized a predictive, feedforward motor control strategy to correct their gait asymmetry and reduce the loading rate in the overloaded limb.6,26 Alternatively, when the overloaded limb was set at the faster speed, the patients failed to develop interlimb symmetry and reverted to their initial baseline asymmetry orientation. It is believed that this asymmetric protocol reinforced the altered gait biomechanics the participants initially presented with. In contrast, the other protocol challenged the participants to adopt new gait dynamics in response to the perturbation demands. These findings demonstrate that when the overloaded limb is set at a slower speed, an asymmetric walking perturbation can effectively restore interlimb loading rate symmetry in patients who had ACLR.
The deadaptation loading rate dynamics of patients who had ACLR provided valuable insight into the short-term storage of the new gait patterns. Following the asymmetric walking protocol in which the overloaded limb was set at the slower speed, patients experienced sustained interlimb symmetry, and the overloaded limbs produced lower loading rates than the underloaded limbs. This was the opposite of the patients’ initial baseline asymmetry, demonstrating a negative aftereffect in response to that protocol. The negative aftereffect indicates that the central nervous system did store the new gait pattern.21,25,28 This temporary storage of the new gait pattern after a single 10-minute session is promising, as it further demonstrates the effectiveness of using asymmetric walking as a gait retraining and/or rehabilitation tool in patients who had ACLR.
The study is not without its limitations. Here, the deadaptation period was only 2 minutes, which may not have fully captured the patients’ deadaptation behavior. However, 2 minutes was long enough to establish 2 points: (1) participants demonstrated the negative aftereffects following the asymmetric protocol that indicated the storage of a new gait pattern, and (2) they demonstrated their progression to normal, symmetric walking. The deadaptation period should be increased in future studies to provide a more comprehensive assessment of deadaptation dynamics. The participants in this study varied in their time since ACLR surgery. Despite this variability, all the participants exhibited the same adaptive response to the asymmetric perturbations, supporting the use of this perturbation in patients who had ACLR regardless of their time since surgery. Yet, future studies should evaluate gait adaptation in response to asymmetric walking in patients who had undergone ACLR at the same time. Moreover, current methods may be difficult to replicate for clinical applications. However, future research should focus on developing a lower-cost training methodology that can simulate the same type of asymmetry as the split-belt treadmill. One possible option explored in the laboratory is using ankle weights to simulate the same type of asymmetry as the treadmill.
Conclusion
This study determined that the short-term adoption and storage of interlimb loading rate symmetry can be achieved through purposely applied asymmetric gait perturbations. The asymmetric protocol was most effective when the overloaded limb was set to a slower speed. Furthermore, this work demonstrated that patients who had ACLR maintained the capacity to adopt new gait patterns despite their impaired neuromuscular function. These findings are promising, as they suggest that asymmetric walking could serve as an effective gait retraining protocol for patients who had ACLR and could help improve long-term outcomes after ACLR.
Footnotes
Final revision submitted May 4, 2023; accepted June 20, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Connecticut (ref No. H17-246).