
Abstract
Background:
Sumo wrestling is a traditional sport in Japan and becoming popular worldwide. Risk factors for lower back injuries in sumo wrestlers are heavier weight and larger body mass index (BMI). The mawashi (loincloth belt) worn by sumo wrestlers has been shown to restrict motion of the lumbar spine.
Purpose:
To study the effects of sumo wrestling on the lumbar spine of high school and freshmen collegiate wrestlers, investigating the relationship between radiological findings, wearing of the mawashi during training, and lower back symptoms.
Study Design:
Case series; Level of evidence, 4.
Methods:
From 2001 to 2017, a total of 197 members of the Japanese Sumo Federation (55 high school and 142 college freshman students) underwent routine radiographic examination of their lumbar spines and answered a questionnaire regarding lumbar symptoms. Wrestlers were classified as symptomatic and asymptomatic based on responses to a custom questionnaire. We used the unpaired t test to evaluate patient demographics and the chi square test to analyze radiographic lumbar spine abnormalities between symptomatic and asymptomatic wrestlers.
Results:
The wrestlers’ mean height, weight, BMI, and duration in the sport were 174.0 ± 6.7 cm, 107.1 ± 22.4 kg, 35.2 ± 6.4, and 8.0 ± 3.2 years, respectively. There were 91 participants in the symptomatic group (46.2%) and 106 (53.8%) in the asymptomatic group. Ten wrestlers (5.1%) had osteophyte formations in the lumbar body; 8 of the 11 osteophytes (72.7%) appeared in the upper lumbar spine. Of the total, 48 wrestlers (24.4%) had deformities (Schmorl nodules) in the lumbar body, and 23 of 50 (46.0%) and 10 of 16 (62.5%) deformities were found in the upper lumbar spine of collegiate and high school wrestlers, respectively. Five wrestlers of the total 197 athletes (2.5%) had disc space narrowing in the lumbar body, with 3 of the 5 cases of disc space narrowing (60.0%) found in the upper lumbar spine. Spondylolysis in the lumbar body was found in 25 wrestlers (12.7%); 19 of the 91 symptomatic wrestlers (20.9%) had spondylolysis, compared with 6 of the 106 (5.7%) asymptomatic wrestlers (P = .0028).
Conclusion:
Almost one-third of sumo wrestlers had ≥1 abnormal radiological finding in the lumbar spine. There was a significant relationship between symptomatic wrestlers and spondylolysis.
The origins of sumo can be traced back to a bout in 23 BC between Nomi-no-Sukune and Taima-no-Kehaya in front of Emperor Suinin in Japan. Sumo has since been a traditional sport in Japan. The first World Sumo Championship was held in 1992, when the International Sumo Federation was established. The World Sumo Championships have been held in various countries, including Japan, Germany, and Brazil. The 23rd World Sumo Championship was held in Japan in October 2019, and the 14th World Women's Sumo Championship was held in Japan in 2019.
The high prevalence of injuries among sumo wrestlers has been thought to be due to the frequency of bouts between wrestlers of different sizes. 13 Nakagawa et al 13 investigated the characteristics and statistics of injuries among sumo wrestlers in 101 collegiate and 203 high school sumo wrestlers. They found that injury-associated pain was most frequently reported in the lower back, neck, knees, and shoulders. 13 The risk factors for lower back injuries are heavier weight and larger body mass index (BMI). The longer a sumo wrestler's career is, the higher the risk of neck, wrist, finger, and shoulder injuries is. 13 However, no increase in the risk of lower back and knee injuries was observed by Nakagawa et al. Therefore, beginner sumo wrestlers, especially heavyweights, are taught how to prevent lower back and knee injuries.
Few studies have reported the radiological findings in sumo wrestlers’ lumbar spines. Therefore, the relationship between radiological findings and lower back symptoms is not well understood. Previously, Minami 11 reported the relationship between the mawashi (loincloth belt) (Figure 1) and the restriction of the lumbar spine motion. The motion of the sumo wrestler's lumbar spine with the mawashi was found to be restricted significantly compared with those without the mawashi, with mean restricted angles of 9.8° in L4/L5, 8.6° in L3/L4, 7.7° in L2/L3, and 4.4° in L1/L2. Because wearing the mawashi was associated with the restriction of the lower lumbar spine, we believe that it can protect the region from L4 to S1.

The mawashi worn by a sumo wrestler during a match (arrow).
The primary purpose of our study was to investigate the relationship between abnormal radiological findings and lower back symptoms in high school and freshman college sumo wrestlers. We were particularly interested in the effect of the mawashi on the spinal region from L4 to S1, because sumo wrestlers almost always use the mawashi during training. The second aim was to investigate the relationship between abnormal radiological findings and the wrestlers’ demographic characteristics. We hypothesized that the presence of abnormalities in the upper lumbar spine would be higher in these wrestlers than in the general population, possibly because of protection of the lower spine due to the mawashi, and that there would be a relationship between sumo wrestlers’ lumbar symptoms and spondylolysis.
Methods
From 2001 to 2017, a total of 55 high school and 142 freshmen collegiate members of a major class in the Japanese Sumo Federation underwent medical checks including questionnaires about their lumbar spine and lumbar radiographies. They had been admitted to high school or university based on their superior sumo wrestling performance in their junior or senior high schools. Sumo wrestlers from 2 high schools and 3 universities participated in the medical examinations from March to May in each academic year, with a participation rate of 100%. We excluded sumo wrestlers who had had lumbar spinal surgery before the medical examination, but there were no sumo wrestlers in this research who had had previous lumbar spinal surgery. All wrestlers were male. The study was approved by the research ethics committee of our hospital, and informed consent was obtained from all participants and their parents or coaches.
We obtained an anteroposterior, a lateral, and 2 oblique radiographic views of the lumbar spine from each participant. The radiographs were obtained in the standing position. The radiogram beam was focused on L3 with an anode-film distance between 1.0 and 1.2 m. A single experienced orthopaedic surgeon (Y.N.) assessed the radiographs for the following 4 indications: osteophyte formation, lumbar body deformities (eg, Schmorl nodules or wedging of vertebral bodies), spondylolysis, and disc space narrowing. Vertebral osteophytes were defined as being >2 mm in length according to the classification of Macnab. 9 Schmorl nodules were defined as clear nonmarginal defects in the vertebral endplate. We also examined the occurrence sites (lumbar body or interbody space). Abnormal radiological findings were defined as the presence of ≥1 of the above changes, which we evaluated by occurrence site (lumbar body or interbody space). In addition, we calculated the occurrence ratios of the abnormal findings between the upper lumbar spine (proximal to L4) and the lower lumbar spine (distal to, and including, L4) to evaluate whether the mawashi made any difference in lumbar spine abnormalities.
Each participant completed a custom questionnaire regarding his lower back symptoms (Table 1). Participants who responded “yes” to experiencing lower back pain for >1 week during sumo wrestling were assigned to the symptomatic group, and those with responses of “no” were assigned to the asymptomatic group. We also assessed the height, weight, BMI, sumo career, and training time per week of each participant.
Questionnaire Regarding the Lumbar Symptoms of the Participants

Statistical analysis was performed to evaluate differences between the self-reported symptomatic and asymptomatic wrestlers. The unpaired t test was used to evaluate the demographic characteristics between the symptomatic and asymptomatic groups, and the chi-square test was used to compare the lumbar spine symptoms between the groups. The level of statistical significance was set at P < .05.
Results
The mean height, weight, BMI, and duration of sumo wrestling experience of the participants were 174.0 ± 6.7 cm, 107.1 ± 22.4 kg, 35.2 ± 6.4, and 8.0 ± 3.2 years, respectively. The mean values of the physical parameters of the high school and collegiate groups are shown in Table 2. The height, weight, BMI, and duration of sumo wrestling experience of high school sumo wrestlers were significantly less than those of collegiate sumo wrestlers. However, the high school sumo wrestlers’ training time (hours/week) was significantly longer than that of collegiate wrestlers (P = .0186).
Characteristics of the Sumo Wrestlers According to Age Group a
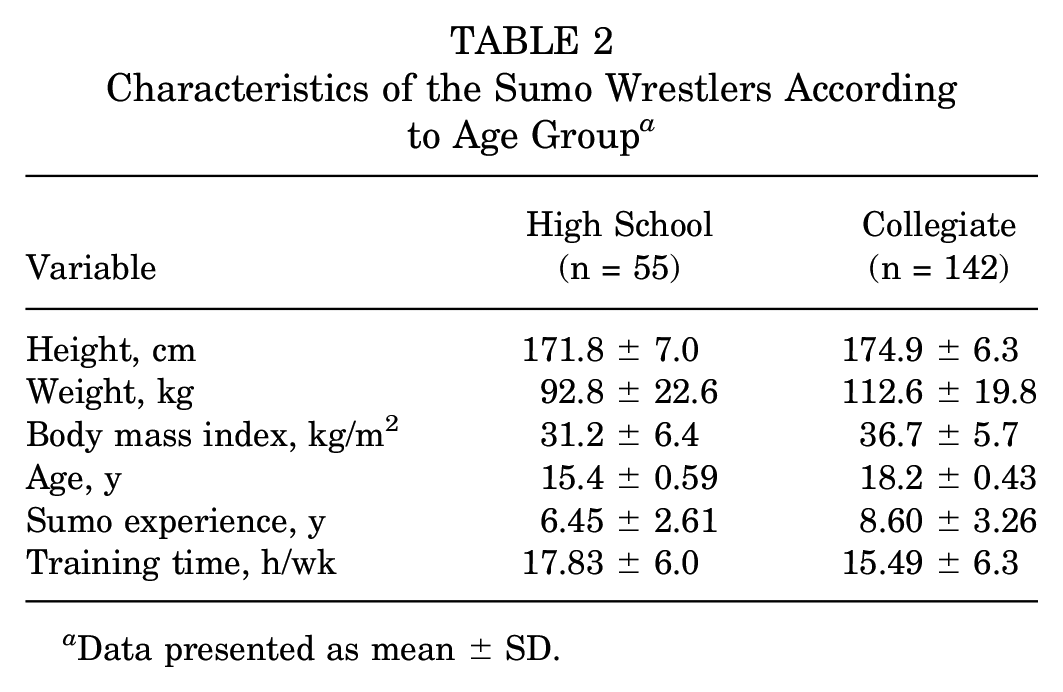
Data presented as mean ± SD.
The symptomatic group consisted of 91 sumo wrestlers (46.2%) and the asymptomatic group 106 (53.8%) wrestlers. A total of 24 high school (43.6%) and 67 collegiate (47.2%) sumo wrestlers had lower back symptoms. The lower back symptoms were not significantly associated with their demographic characteristics (Table 3).
Characteristics of the Sumo Wrestlers According to Lower Back Symptoms

On radiographs of lumbar spine alignment, 41 of the 55 (74.6%) high school sumo wrestlers were in lordosis, and 14 (25.5%) were straight. Of the 142 collegiate sumo wrestlers, 93 (65.5%) were in lordosis and 49 (34.5%) were straight. No significant difference in the ratio of physiological lordosis was observed between the high school and college cohorts (P = .2925).
Ten wrestlers (5.1%) had osteophyte formations in the lumbar body, comprising 1 high school (1.8%) and 9 collegiate participants (6.3%) (Figure 2, A-C). In collegiate wrestlers, 7 of 12 lumbar body osteophytes (58.3%) appeared in the upper lumbar spine and 5 (41.7%) in the lower lumbar spine. Concerning intervertebral level, 8 of 11 osteophytes (72.7%) appeared in the upper lumbar spine and 3 (27.3%) in the lower lumbar spine of collegiate sumo wrestlers. There was a significant difference in training time between participants with and without osteophytes (20.9 ± 18.6 vs 15.9 ± 4.9 hours/week, respectively; P = .0136) (Figure 2D).

(A) Sagittal radiograph of lumbar spine showing osteophyte formation (arrow) in the lumbar body. (B and C) Prevalence of osteophytes in collegiate and high school sumo wrestlers: (left) lumbar body and (right) interlumbar body space. (D) Lumbar osteophyte formation with relation to mean training time. Error bars represent SD.
Of the total, 48 wrestlers (24.4%) had deformities in the lumbar body, comprising 13 high school (23.6%) and 35 collegiate (24.7%) wrestlers (Figure 3, A-C). In collegiate wrestlers, 19 of 50 deformities (38.0%) appeared in the upper lumbar spine and 31 (62.0%) in the lower lumbar spine, while in high school wrestlers, 10 of 21 deformities (47.6%) appeared in the upper lumbar spine and 11 (52.4%) in the lower spine. Concerning intervertebral level, 23 of 50 deformities (46.0%) were in the upper lumbar spine and 27 (54.0%) in the lower lumbar spine of collegiate sumo wrestlers. In high school participants, 10 of 16 deformities (62.5%) were in the upper lumbar spine and 6 (37.5%) in the lower spine. There was a significant difference in weight between participants with and without lumbar body deformities (113.2 ± 20.0 vs 105.1 ± 22.8 kg, respectively; P = .0286) (Figure 3D).

(A) Sagittal radiograph demonstrating Schmorl nodules in the L3 and L4 lumbar bodies (arrows). The lowest vertebral body was S1 (arrowhead). (B and C) Prevalence of deformities in the lumbar body (Schmorl node or wedged vertebral body) in collegiate and high school sumo wrestlers: (left) lumbar body and (right) interlumbar body space. (D) Lumbar body deformity in relation to mean weight. Error bars represent SD.
There were 25 cases (12.7%) with spondylolysis in the lumbar body, comprising 8 high school wrestlers (14.6%) and 17 collegiate wrestlers (12.0%) (Figure 4). Spondylolysis appeared mainly at the fifth lumbar body, was bilateral, and was mainly pseudoarthrosis. Five wrestlers (2.5%) had disc space narrowing in the lumbar body; all were collegiate wrestlers (3.5%) (Figure 5). Concerning the interlumbar space, disc space narrowing was noted in the upper lumbar spine in 3 of 5 cases (60.0%) and in the lower spine in 2 of 5 (40.0%) cases, all in collegiate wrestlers. A total of 69 wrestlers (35.0%) had abnormal radiological findings in the lumbar body, which were seen in 18 high school (32.7%) and 51 collegiate participants (35.9%). There were no significant differences in demographic characteristics between cases of spondylolysis, disc space narrowing, or abnormal radiological findings in the lumbar body.

(A) Oblique radiograph of the lumbar spine demonstrating spondylolysis at L5 (arrow). Prevalence of spondylolysis in the lumbar body of (B) collegiate and (C) high school sumo wrestlers.

(A) Sagittal radiograph of lumbar spine showing disc space narrowing at L4-L5 and L5-S1 (arrows). (B) Prevalence of the disc space narrowing in collegiate sumo wrestlers.
Regarding the relationship between lumbar symptoms and radiological findings, there was a significant difference between the symptomatic and asymptomatic wrestlers with regard to presence of spondylolysis. Nineteen of the 91 (20.9%) symptomatic group wrestlers and 6 of the 106 (5.7%) asymptomatic group wrestlers had spondylolysis in the lumbar body (P = .0028) (Table 4). There were no significant differences in the occurrence ratios of the abnormal radiological findings between high school and collegiate wrestlers (symptoms, P = .4669; osteophytes, P = .3490; lumbar body deformities, P = .9999; spondylolysis, P = .8030; disc space narrowing, P = .3643; abnormal radiographic findings, P = .7986).
Comparison of Radiologic Findings Within the Symptomatic and Asymptomatic Groups a

Data are shown as number of participants. Boldface P value indicates statistically significant difference between groups (P < .05).
Discussion
The study's main findings were as follows. Ten wrestlers (5.1%) had osteophyte formations in the lumbar body (1 high school [1.8%]; 9 collegiate [6.3%]). Regarding interbody space, 8 osteophytes (72.7%) appeared in the upper lumbar spine. There was a significant difference in training time between wrestlers with versus without osteophytes (P = .0136). Of the total, 48 wrestlers (24.4%) had deformities in the lumbar body (13 high school [23.6%]; 35 collegiate [24.7%]). Concerning interbody space, 23 deformities (46.0%) appeared in the upper lumbar spine of collegiate, and 10 (62.5%) of high school, wrestlers. There was a significant difference in weight between wrestlers with versus without lumbar body deformities (P = .0286). A total of 25 wrestlers (12.7%) had spondylolysis in the lumbar body (8 high school [14.6%]; 17 collegiate [12.0%]). Five wrestlers (2.5%) had disc space narrowing in the lumbar body; all were collegiate wrestlers. Regarding interbody space, there were 3 cases of disc space narrowing (60.0%) in the upper lumbar spine of the 5 collegiate wrestlers. Of the total, 69 wrestlers (35.0%) had ≥1 abnormal radiological finding in the lumbar body. Finally, there was a significant difference in spondylolysis between the self-reported symptomatic and asymptomatic wrestlers (P = .0028). Our results might show that spondylolysis and the formation of Schmorl nodules appeared between elementary and junior high school, whereas osteophytes appeared between junior and senior high school. Disc space narrowing occurred in senior high school or possibly afterward, in our opinion.
In a study of athletes participating in the 2016 Summer Olympic Games, 52 of the 100 (52%) athletes who received cervical, thoracic and lumbar spine magnetic resonance imaging (MRI) showed moderate-to-severe spinal disease. 23 The highest sport-specific incidence of moderate-to-severe spinal disease was seen in diving athletes (67%). Weightlifting had the second highest incidence (67%). Athletes >30 years old had the highest rate of moderate-to-severe spinal disease on MRI (65%). In sumo wrestlers in the current study, the rate of abnormal radiological findings was 35%, which is high.
In collision sport studies, 67% of collegiate football players had low back pain, but only 1.6% required surgery. 10 Continuing to play American football through 2 years of high school was a risk factor for the onset of lower back pain. 12 In weightlifting, a prospective 3-year cohort MRI study of 12 child and adolescent weightlifters revealed abnormal lumbar findings in 11 participants. Children and adolescents undergoing resistance training at the competition level could have irreversible changes in the lumbar vertebrae without symptoms. 21 It was reported that pediatric patients represented only 0.4% of their lumbar discectomy population, with 50% of the disc herniations sustained during athletic activity. 21 Children who participate in collision sports and weightlifting are at increased risk for lumbar disc herniation because of the increased axial forces exerted on the spine during hyperflexion and hyperextension. 16 In our study, 46% of sumo wrestlers had some lumbar symptoms. However, none required lumbar spine surgery, consistent with the above reports.
In the Japanese general population, the prevalence rates of lumbar spondylosis in the age groups ≤39, 40-49, 50-59, 60-69, 70-79, and ≥80 years were 14.3%, 45.5%, 72.9%, 74.6%, 85.3%, and 90.1%, respectively, in men. 25 Nemoto et al 14 reported that 6 of 90 (6.7%) young adults in the Japanese military aged from 18 to 20 years had abnormal radiological findings in their lumbar spine. In 74 parachuting instructors with a mean age of 33 years, the degenerative radiological changes in the lumbar spine were identified in 26%. 2 In the current study, 69 wrestlers (35.0%) had abnormal lumbar body radiological findings, which is a larger ratio than that in the abovementioned reports. Imagama et al 4 reported that age was significantly negatively correlated with the lumbar lordosis angle. In our study, 68% of the all sumo wrestlers had lumbar lordosis, and no wrestlers had lumbar kyphosis.
Osteophytes were identified in 6.8% of parachuting instructors. 2 In Japanese military adults with a mean age of 38.5 years, osteophytes were observed in 39 of 85 patients (46%), showing the greatest prevalence in L4 followed by L5 and L3. 14 In reinforcement workers and house painters, osteophytes were most frequently observed at L3/L4. 18 In the normal population, studied by Shao et al, 20 osteophytes occurred most frequently at level L4 in men. Schmitt et al 19 reported that high jumpers and athletes in throwing disciplines have a higher risk of developing lumbar spine vertebral osteophytes, even if body constitution were a preselection factor. In former professional football players, significantly higher prevalence of osteophytes at levels T12, L1, L2, and L4 was found in football players than in the control group. 15 The mechanical loading due to heavy work and excess activity causes the osteophyte formation, especially in the lumbar spine. In the present study, 10 wrestlers (5.1%) had osteophyte formations in the lumbar body, and 8 osteophytes (72.7%) appeared in the upper lumbar spine. Because the use of mawashi restricts the movement of the lower lumbar spine of a sumo wrestler, this can protect the region from L4 to S1. The prevalence of osteophytes in the upper lumbar spine was greater than that in the general population, 20 and we speculate the mawashi can add stress to the upper lumbar spine and result in these radiographic findings.
There have been several papers about deformities in the lumbar bodies or degenerative disc diseases in athletes. Schmorl nodules were identified in 8.1% of parachuting instructors 2 and were significantly more common in young elite skiers (46%) compared with controls (0%). 24 In the present study, 48 wrestlers (24.4%) had deformities in the lumbar body, which were mainly Schmorl nodules. There appeared 23 deformities (46.0%) in the upper lumbar spine of collegiate sumo wrestlers and 10 (62.5%) of that of high school wrestlers. MRI has shown that as many as 95% of asymptomatic players have radiological abnormalities of the lumbar spine, generally at the L4/L5 and L5/S1 levels. 17 Abdalkader et al 1 investigated the degenerative disc diseases in athletes participating in the Rio de Janeiro Olympic Games. 1 L4/L5 and L5/S1 levels were the most affected in mild cases (46%) and in moderate cases (82%). In our study, 5 collegiate wrestlers (3.5%) had disc space narrowing in the lumbar body, and 3 of these 5 had narrowing (60.0%) in the upper lumbar spine. The prevalence of Schmorl nodules and disc space narrowing in the upper lumbar spine was high and may have resulted from using the mawashi.
Sterba et al 22 suggested that combined flexion, axial rotation, and compression generated the highest stress conditions contributing to the risk of spondylolysis. Adolescent participants in sports requiring repetitive flexion, hyperextension, and rotation of the spine (such as gymnastics, football, dance, and weightlifting) are at a greater risk of developing spondylolysis. 7 It has been our observation that sumo wrestlers often experience hyperextension of the lumbar spine when pushed down near the edge of the dohyo (the playing area of a sumo bout). Hyperextension from torsion of the lumbar spine can also occur if a wrestler throws his heavy opponent down. In college football players, the rate of spondylolysis was only 4.8% in athletes compared with 6.0% in controls. 6 In pole vaulters, the prevalence rates of lumbar spondylolysis and intervertebral disc degeneration were 28.6% (6/21) and 38.1% (8/21), respectively. 3 In the present study, 25 wrestlers (12.7%) had spondylolysis in the lumbar body, comprising 8 high school (14.6%) and 17 collegiate (12.0%) wrestlers. Iwamoto et al 5 reported that an abnormality such as spondylolysis was the most significant risk factor for low back pain in high school and college football players. Lundin et al 8 investigated 134 former top athletes from different sports and found no correlation between back pain and specific radiologic abnormalities. In our study, there was a significant correlation between lumbar symptoms and spondylolysis.
Limitations
The limitations of this study are the following: First, we studied only moderate cases (197 cases), and the cases with abnormal radiographic findings in the lumbar spine were small. Second, this was a case series study, and a longitudinal study would have had advantages. Third, there was the absence of a control group of individuals of similar gender and age. Fourth, to elucidate the effects of mawashi, further research to prospectively investigate the relationship between the use of the mawashi and the intervertebral level is needed. Fifth, we did not perform interrater testing of the radiographic findings. Last, we had no advanced imaging such as computerized tomography or MRI of the lumbar spine.
Conclusion
In the current study, almost one-third of sumo wrestlers had abnormal radiological findings in the lumbar spine. There was a significant correlation between the lumbar symptoms and spondylolysis. Further studies and research are needed to evaluate the natural history of these radiographic findings and the effects of wearing the mawashi.
Footnotes
Final revision submitted May 2, 2023; accepted May 19, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyoto Medical Center (ref No. 15-054).