
Abstract
Background:
Sumo has long been a traditional sport in Japan and is rapidly attracting enthusiasts abroad. Sumo wrestling entails a risk of impact to the cervical spine during an initial charge. Few reports are available in the English-language literature regarding radiological changes in the cervical spine in sumo wrestlers.
Purpose:
To examine radiological changes in the cervical spine in freshmen collegiate sumo wrestlers.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 53 freshmen sumo wrestlers (age, 18-19 years) who belonged to the Japan Sumo Federation underwent routine radiographic examination of the cervical spine and completed questionnaires on cervical symptoms.
Results:
Of the 53 wrestlers, 81% showed loss of lordosis, 45% showed osteophyte formation (mainly at C3-C4), 11% showed disc space narrowing (mainly at C5-C6), and 51% showed narrowing of the cervical nerve root foramina (mainly at C3-C4). Fifty-one percent had some cervical symptoms. A correlation was found between deformity of the cervical bodies (such as intervertebral disc ballooning) and cervical symptoms, but no correlation was found between cervical degenerative changes and cervical symptoms.
Conclusion:
Our data suggest that loss of lordosis, osteophyte formation, and narrowing of the cervical nerve root foramina at C3-C4 were frequently present in freshmen wrestlers and may be due to the axial load incurred prior to their collegiate careers.
Sumo has long been a traditional sport in Japan. In Japan, many sumo wrestlers start to play sumo during junior high school. Many collegiate sumo wrestlers have about 20 competitions per year and about 20 matches per competition. In training, they have about 50 initial charges per day. Since the first Sumo World Championships were held in 1992, sumo wrestling has gained popularity worldwide for both men and women. Approximately 85 countries now belong to the International Sumo Federation. Thus, sumo is enjoyed and practiced by many people and has recently become a worldwide sport.
In sumo wrestling, pain is most frequently reported from lower back, neck, knee, and shoulder injuries, while in top division wrestling, disabilities from injuries of the knee, neck, shoulder, and ankle are most commonly reported. 11 It has been reported that 91% of collegiate top division sumo wrestlers and 79% of high school top division sumo wrestlers have experienced intense burning pain about the neck. This “burner syndrome” represents one of the most common injuries seen in sumo. Although many sumo wrestlers have only mild symptoms, a few have prolonged symptoms. 12 Sumo wrestling entails a risk of impact to the cervical spine, and we have previously reported 2 instances of cervical spinal cord injuries in sumo wrestlers. 13,16 Sumo wrestlers make contact with their head and upper trunk during an initial charge, which is the same type of contact that occurs in American football, and their cervical spines suffer from an axial load.
The purpose of this study was to evaluate radiological changes in the cervical spine of freshmen collegiate sumo wrestlers in order to study the effects on their cervical spine during training prior to college, investigate the relationship between radiological changes and cervical spine symptoms, and examine the relationship between cervical radiological changes and the physical characteristics of the wrestlers.
Methods
Over a 5-year period (1999-2003), 53 freshmen collegiate sumo wrestlers who belonged to the top division in the Japanese Sumo Federation underwent medical examination with cervical radiographs, completed questionnaires about their cervical symptoms, and were assessed with regard to their physical characteristics. They had been admitted to university on the basis of their superior sumo wrestling performance during high school. Sumo wrestlers from 3 universities participated in the medical examinations from March to May each academic year, with a participation rate of 100%. Informed consent was obtained from all wrestlers before participation, and all procedures were reviewed and approved by the research ethics committee of our hospital.
For each participant, 6 routine cervical radiographs were performed, including anteroposterior, bilateral oblique, and functional lateral views (neutral, flexion, and extension positions). These radiographs were assessed for alignment, osteophyte formation, deformity of the cervical bodies, disc space narrowing, narrowing of the nerve root foramina, and diameter of the cervical spinal canal. Alignments were assessed with participants in the lateral neutral position. The alignments were divided into 4 categories: lordosis, straight, kyphosis, and S-curve. The diameter of the cervical spinal canal was measured with lateral, neutral view radiographs of the fifth and sixth cervical bodies, and the mean score was calculated.
Questionnaires about spine-related symptoms of the participants included information regarding whether they had neck pain or radiating pain from the neck to the arm continuing for more than 1 week, either at present or in the past during sumo wrestling. Wrestlers with responses of “yes” were assigned to the symptomatic group, while those with responses of “no” were assigned to the asymptomatic group. In addition, we assessed their height, weight, body mass index (BMI), sumo career, and training time per week.
Statistical analysis was performed with either the unpaired t test or the Mann-Whitney U test to evaluate the relationship between cervical radiological changes and physical characteristics. The chi-square test was used to analyze the relationship between the radiological changes and the cervical spine symptoms. The level of statistical significance was set at P < .05.
Results
The symptomatic group consisted of 27 sumo wrestlers (51%), and the asymptomatic group consisted of 26 sumo wrestlers. Their age was 18 or 19 years, and all of them were male. The physical characteristics are shown in Table 1.
Characteristics of Participants

On radiographs of cervical spine alignment, 15 of the sumo wrestlers (6 symptomatic and 9 asymptomatic) had lordosis, 26 wrestlers (11 symptomatic and 15 asymptomatic) had straight alignment, 8 wrestlers (7 symptomatic and 1 asymptomatic) had kyphosis, and 4 wrestlers (2 symptomatic and 2 asymptomatic) had S-curve alignment (Figure 1). Thus, only 28.3% of the wrestlers had lordosis.

Radiographs of cervical spine alignment in lateral neutral position. (A) Lordosis, (B) straight alignment, (C) kyphosis, and (D) S-curve.
Twenty-four wrestlers (45%) had osteophyte formations in the cervical body, mainly at C3-C4 (Figure 2). Twenty-two wrestlers (42%) had a deformity of the cervical body, mainly at C3 and C6 (Figure 3). In the upper cervical spine, the deformity was due to intervertebral disc ballooning, while in the lower cervical spine, the deformity was due to a flat vertebral body. Six wrestlers (11%) had disc space narrowing; 50% of these (3/6 cases) were between the fifth and sixth cervical bodies. No relationship was found between these deformities and the physical characteristics of the wrestlers.

Osteophyte formations in the cervical body. (A) Osteophyte formation in the upper posterior of the fourth cervical body (arrow). (B) Frequency of osteophyte formation.

Deformity of the cervical body. (A) Intervertebral disc ballooning in the third and fourth cervical bodies (arrows). (B) Frequency of deformity of the cervical bodies.
Twenty-seven wrestlers (51%) had narrowing of the nerve root foramina, mainly in the third and fourth foramina (Figure 4), and 56% of these cases entailed bilateral narrowing. A higher BMI (P = .0306) and a longer sumo career (P = .0396) were found to be risk factors for narrowing of the nerve root foramina.
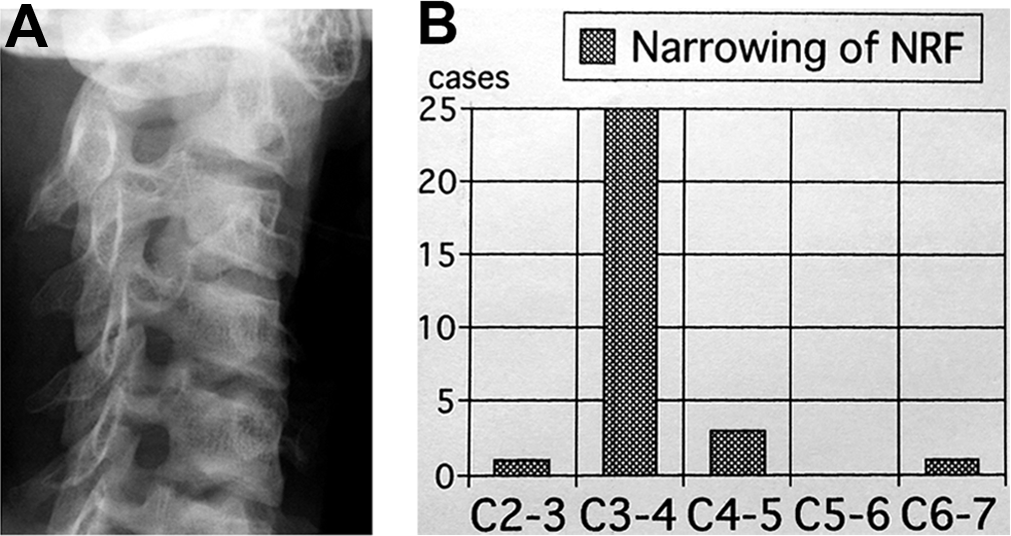
Narrowing of the nerve root foramina. (A) Narrowing of the nerve root foramina in the third and fourth foramina. (B) Frequency of narrowing of the nerve root foramina.
The mean diameter of the cervical spinal canal was 16.4 mm (range, 13.5-19 mm). No relationship was found between the diameter of the cervical spinal canal, the participants’ cervical symptoms, and other deformities shown on their cervical radiographs.
With regard to the relationship between cervical symptoms and radiological changes, a significant correlation (P = .0382, chi-square test) was noted between deformities of the cervical body and the cervical symptoms of the participants. Fifteen of the 26 wrestlers in the symptomatic group and 7 of 27 wrestlers in the asymptomatic group had a deformity of their cervical body.
Thirty-eight wrestlers (72%) had degenerative radiographic changes such as osteophyte formation, disc space narrowing, or narrowing of the nerve root foramen. No relationship was found between degenerative radiographic changes and the participants’ physical characteristics or between radiological changes and cervical spine symptoms.
Discussion
We found that freshmen sumo wrestlers frequently had abnormalities on cervical spine radiographs. In a report by Gore 5 on radiographic findings in the cervical spine of asymptomatic persons, the majority had cervical lordosis, with a mean angle of 18°. The most frequent sites of degenerative changes and the most severe changes were at C5-C6 and C6-C7. In a magnetic resonance imaging (MRI) study of the cervical spine in healthy teenage male volunteers, 17% had degenerative findings and 2% had disc space narrowing and foraminal stenosis. 9,17 In our study, the sumo wrestlers had more degenerative changes and loss of lordosis in their cervical spine than these healthy volunteers. 5,9,17
In a study of American football players, Tsukimura 23 reported that only 40.6% had physiological cervical lordosis. Albright et al 2 reported on 75 first-year football recruits who underwent radiography of their cervical spine after playing football in high school but before playing in college. Of these participants, 32% had 1 or more of the following: occult fractures, vertebral body compression fractures, intervertebral disc space narrowing, or other degenerative changes; only 13% admitted to a previous history of neck symptoms. The development of early degenerative changes or intervertebral disc space narrowing in this group was attributed to the effect of repetitive axial loading of the cervical spine as a result of head impact from blocking or tackling. The mechanism of cervical spine loading in American football is similar to that seen in sumo wrestling.
In another study, front-row rugby players exhibited significant radiographic evidence of cervical spine degenerative changes compared with non–rugby playing controls; most of the changes existed in the lower cervical spine. 6 In an MRI study of rugby players, 20% of the junior rugby players already had anterior cervical osteophytes at the C6-C7 level. 3 Posterior and anterior osteophytes were observed in 29 senior and veteran players (83%), compared with 10 of 30 (33%) age-matched control participants. In the rugby players, the height of the vertebral bodies of the lower cervical spine decreased with age, whereas in the control participants the vertebral body height remained stable with age. Similar to the findings in the rugby players, 22 wrestlers (42%) in our study had deformity of the cervical body.
In a study of soccer players, Sortland et al 19 reported that the onset of degenerative changes among 43 athletes occurred 10 to 20 years earlier, and with a slightly increased frequency, than in males of a similar age group. Heading blows resulted in injuries to the vertebral bodies, the intervertebral joints, and the discs in the lower part of the cervical spine, primarily with hyperextension or compression strains. It was postulated that these changes were due to high-impact and/or low-impact recurrent trauma to the cervical spine caused by heading the ball. 10 It is also noteworthy that a Japanese study found cervical osteophytes in 9 of 12 players who made extensive head plays. 8 The sumo wrestlers in our study had the same or greater rates of cervical degenerative changes compared with the athletes in the above-mentioned studies.
Athletic injuries to the cervical spine resulting in damage to the spinal cord are infrequent but catastrophic events that have been associated with water sports, 1 football, 22 rugby, 4,18 and other activities. However, cervical spinal cord injuries associated with sumo are rare. Two of the authors (Y.N., K.M.) of the present study have provided medical care at various sumo championships for the Japan Student Sumo Federation for about 20 years; however, apart from the 2 cases described in the present study, we have never witnessed any spinal cord injuries. We therefore consider sumo to be a relatively safe sport. Sumo wrestlers report the occasional incidence of burning pain in the cervical spine region. We found that 91% of collegiate top division sumo wrestlers belonging to the West Japan Student Sumo Federation claim to have experienced burning pain, which includes mild cases that occurred on tachiai, or the initial charge. 12
Only 5 cases of cervical spinal cord injury associated with sumo have been previously reported. 7,13,16,20,24 The first report involved a 16-year-old recreational sumo wrestler who pushed his opponent with his head on the initial charge and suffered neck hyperextension, which led to a fracture of C2 and cervical cord injury. 7 The second report involved a C1-C2 dislocation and a cervical spinal cord injury in an 18-year-old boy with os odontoideum who was thrown down. 20 A third report entailed a C4-C5 cervical disc herniation in a 25-year-old professional sumo wrestler due to repeated constant force on the neck during the initial charge. 24 The fourth report described a 31-year-old amateur sumo wrestler who fell on the crown of his head with his neck held by his opponent and sustained an atlantoaxial dislocation and a central cervical spinal cord injury. 13 The fifth report was on a high-level collegiate sumo wrestler who had anterior dislocation of C7 on T1 and a cervical spinal cord injury. 16 He was pushed down near the edge of the dohyo, or sumo ring, while the back of his head was placed on the abdomen of his opponent, resulting in hyperflexion of his cervical spine. These participants did not have any degenerative changes or congenital abnormalities except for the 1 patient with os odontoideum.
The characteristics of degenerative cervical spine changes in sumo wrestlers are osteophyte formation and narrowing of the nerve root foramina, mainly between the third and fourth cervical bodies. Torg et al 21 proposed that traumatic C3-C4 level injuries resulting from athletic activity are due to axial loading. Sumo wrestlers make contact with their head and upper trunk during an initial charge, which is the same type of contact that occurs in American football. In our study, a higher BMI and a longer sumo career were found to be risk factors in narrowing of the nerve root foramina. Osteophyte formation and narrowing of the cervical nerve root foramina of the third and fourth cervical vertebrae are possibly due to the axial load incurred during sumo training in junior and senior high school.
Compared with the results of Nakagawa et al, 14 who examined radiological changes in the cervical spine of amateur sumo wrestlers of all ages, we found a similar frequency of osteophyte formation and narrowing of the nerve root foramina in freshmen collegiate wrestlers. However, the frequency of disc space narrowing differed between the amateurs and the freshmen wrestlers. Therefore, we concluded that disc space narrowing of the fifth and sixth cervical vertebrae occurred during sumo training in university and after graduation from university. In a study by Nakagawa, 15 however, it was thought that degenerative changes of the cervical spine did not worsen if the sumo wrestler retired. In Japan, many sumo wrestlers continue to compete until they are about 30 or 35 years old.
The limitations of this study were the small number of cases (N = 53) and the lack of age-matched controls. Another weakness of this study was that comparison groups were historical (from other studies), which introduces variability in the radiological techniques used to evaluate these changes. Further, this was a time zero study, thus we did not follow the athletes over time to determine whether they developed cervical symptoms or additional abnormalities as their career progressed.
In summary, we examined radiological changes in the cervical spine in 53 freshmen collegiate sumo wrestlers who belonged to the Japan Sumo Federation. Cervical spine abnormalities and degenerative changes were frequently seen in this cohort. A correlation was found between cervical body deformities and cervical symptoms but not between cervical degenerative changes and cervical symptoms.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Research Ethics Committee of the National Hospital Organization, Kyoto Medical Center.