
Abstract
Background:
The optimal graft choice for anterior cruciate ligament (ACL) reconstruction (ACLR) in the high-level cutting and pivoting athlete remains controversial. Studies have shown similar outcomes when directly comparing bone-patellar tendon-bone (BPTB) autograft versus quadriceps soft tissue (QST) autograft in the general population. However, no studies have directly compared these 2 grafts in athletes participating in cutting and pivoting sports.
Hypothesis:
It was hypothesized that, compared with BPTB autograft, the QST autograft would result in similar patient-reported outcomes and rates of retear, return to sport, and complications.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was performed on athletes participating in cutting and pivoting sports (soccer, American football, lacrosse, and basketball) who underwent primary ACLR with either BPTB autograft or QST autograft chosen by the athlete between January 2015 and January 2019. The International Knee Documentation Committee (IKDC) subjective knee evaluation and Lysholm Knee Scoring Scale were used to evaluate patient-reported outcomes. Return-to-sport and complication rates were identified. Descriptive statistics were expressed using Mann-Whitney test or Student t test for continuous variables and the chi-square test for categorical variables.
Results:
A total of 68 athletes (32 QST, 36 BPTB) were included for analysis. The percentage follow-up was 89% (32/36) for the QST autograft group and 86% (36/42) for the BPTB autograft group. The 2-year IKDC score (QST, 90.5 ± 6.6 vs BPTB, 89.7 ± 7.8) and 2-year Lysholm score (QST, 91.3 ± 7.5 vs BPTB, 90.5 ± 8.6) were similar between groups. The percentage of athletes able to return to sport within the follow-up period was also similar (88% vs 83%; P = .63). There were 2 retears requiring revision in the BPTB group (6%) and no retears in the QST group (P = .18). One contralateral ACL rupture occurred in the QST group (3%) and 4 in the BPTB group (11%) (P = .21).
Conclusion:
The QST and BPTB autografts demonstrated similar patient-reported outcomes, return-to-sport rates, and complication rates after primary ACLR at 2-year follow-up. Both autografts appear to be reliable and consistent options for ACLR in the cutting and pivoting athlete.
Anterior cruciate ligament (ACL) reconstruction (ACLR) is one of the most common knee procedures performed annually in the United States.21,27 Several graft choices including allograft, bone-patellar tendon-bone (BPTB) autograft, hamstring tendon (HT) autograft, and quadriceps soft tissue (QST) autograft have been described. Each of these options have demonstrated favorable patient-reported outcomes and complication rates with appropriate patient selection in the general population.1,2,29,30
It is well understood that athletes participating in cutting and pivoting sports are at particularly high risk for primary ACL injury and retear.13,17 Younger patients, especially adolescents, are also at higher risk for ACL graft failure compared with older patients. 6 Despite a body of literature comparing autograft options in the general and athletic populations, reports dedicated to outcomes in the high-level cutting and pivoting athlete remain limited. Accordingly, the “gold standard” in the young, high-level cutting and pivoting athlete remains controversial. Many consider BPTB autograft to be this standard for such athletes. 4 However, BPTB autografts have notable drawbacks, including extensor weakness, 24 anterior knee pain, difficulty kneeling, possible patellar fracture, patellar tendon rupture, and patellofemoral osteoarthritis.7,20 In addition, BPTB autografts should be used with caution in skeletally immature patients due to potential physeal injury. 10 Quadriceps autograft has recently increased in popularity, offering a larger graft diameter with more favorable tensile properties compared with BPTB and HT autografts. 18 Specifically, the quadriceps autograft can have nearly twice the cross-sectional area with higher load to failure and greater stiffness than the BPTB autograft.12,28
Previous studies have shown equivalent outcomes when directly comparing BPTB versus QST autograft in the general population.11,16,19 However, data are limited in athletes participating in cutting and pivoting sports. The purpose of this study was to compare the outcomes after ACLR with BPTB versus QST autografts in a cohort of pivoting and cutting athletes at a minimum of 2-year follow-up. It was hypothesized that the QST autografts would lead to similar functional outcomes, return to sport, retear rates, and complications compared with BPTB autografts in the cutting and pivoting athlete.
Methods
After receiving approval from the hospital's institutional review board, we conducted a retrospective review of amateur high school and college athletes competing in cutting and pivoting sports who underwent ACLR with BPTB or QST autograft between January 1, 2015 and January 31, 2019. Primary ACL tears were diagnosed by clinical examination and confirmed by magnetic resonance imaging. All clinical assessments and procedures were performed by the senior author (K.J.E.), who is a fellowship-trained sports medicine surgeon whose practice includes treating recreational, amateur, and professional athletes. The senior author performs a mix of HT, BPTB, and QST autografts for ACLRs. An independent team of researcher coordinators collected all data. Only athletes actively participating in 4 cutting and pivoting sports (soccer, American football, lacrosse, and basketball) were selected for inclusion. Exclusion criteria included recreational athletes, athletes with recurrent ACL tears, multiligamentous injuries, previous meniscal surgery, and those requiring osteotomies. Athletes who did not have 2 years of follow-up data were excluded from this analysis. All included participants provided written informed consent.
The decision of graft type was based on the athlete's choice after discussing the advantages and disadvantages of various graft options, including allografts and autografts. All patients were informed of the higher retear rates observed in allografts in younger patients.3,14 Autograft options included BPTB, HT, and QST.
The advantages of tensile strength and bone-to-bone healing for the BPTB autograft were explained, as were the risks of patellar fracture and anterior knee pain. The advantages of decreased knee pain postoperatively and simplicity of graft harvesting for the HT autograft were explained, as were the risks of variable graft size and potentially increased infection rates. The advantages of a more predictable graft size, highest collagen content, and avoiding injury to the posterior compartment structures for the QST graft were explained as were the risks for increased stiffness after surgery and possibly longer recovery for developing quadriceps strength. In addition, the patient was informed that QST grafts are currently used less frequently in comparison with BPTB and HT autografts. The patient made the decision regarding graft choice after a full discussion of these advantages and disadvantages with the ability to ask questions. The patient was allowed additional days to make the decision if needed.
Surgical Technique
The procedures were performed under general anesthesia with a regional femoral block in all patients. Before harvesting the autografts, a diagnostic arthroscopy was performed to confirm the presence of a completely torn ACL.
The quadriceps tendon harvest was performed through a 2-cm transverse incision made just proximal to the superior pole of the patella. Dissection was taken down through the soft tissue identifying the quadriceps tendon. The quadriceps tendon was then cleared off using a using a key elevator. A double-bladed quadriceps tendon harvesting knife (Arthrex) was used to cut the central portion of the quadriceps tendon. A 10-mm knife was used for all cases. Once parallel incisions were made in the quadriceps tendon, the distal aspect of the graft was dissected from the proximal pole of the patella and a FiberWire suture (Arthrex) whipstitch was placed in the distal end of the graft. A cigar cutter (Arthrex) was then used to transect the proximal aspect of the graft at 65 mm for patients less than 183 cm in height, 70 mm for patients between 185 and 198 cm, and 75 mm for all athletes over 198 cm tall. The graft was then prepared removing excess soft tissue. A FiberWire suture was used to whipstitch a TightRope (Arthrex) on the femoral side and TightRope attachable button system on the tibial side. While the graft was being prepared, the defect in the central quadriceps tendon was closed with a running No. 2 FiberWire placed with a Scorpion device (Arthrex).
The BPTB autograft was harvested through a midline incision that is made from the inferior pole of the patella to the tibial tubercle. Dissection was taken down until the paratenon was identified and opened sharply. A patellar retractor was placed over the top of the patella. A bone plug (20 × 10 mm) on the central-inferior pole of the patella was marked with a cautery. A saw was then used to cut the 20 × 10 × 10-mm bone plug out in trapezoidal fashion. A 10 mm–wide strip of the central patellar tendon was then cut down to the tibial tubercle. Next, a 20 × 10 mm area was marked on the tibial tubercle with the cautery. A saw was then used to cut the bone graft and a curved osteotome used to extract the bone plugs. The bone plugs of the graft were then trimmed down to 20 × 10 mm. A TightRope was attached to the femoral bone plug and 2 passing sutures were placed on the tibial side. The graft diameter was then measured and the graft placed on tension on the back table.
Once graft preparation was completed, meniscal pathology was assessed. When performed, meniscal repair was completed using all-inside technique using the Fastfix 360 meniscal repair device (Smith & Nephew). Remnants of the ACL were then removed with a shaver. The medial wall of the lateral femoral condyle was cleared off. An accessory medial portal was then created in all cases. Through the accessory medial portal, the over-the-top guide was placed over the back of the lateral femoral condyle. The knee was then hyperflexed, and a spade-tipped guide pin was placed through the ACL femoral footprint and out the lateral cortex of the femur. A low-profile reamer of appropriate size (Arthrex) was then placed over the spade-tipped guide pin, and a 25-mm femoral socket was then drilled.
For the quadriceps tendon ACL, an all-inside technique was used. A tibial guide (Arthrex) set at 55° was placed on the tibial footprint. A FlipCutter of appropriate diameter (Arthrex) was then used to create a 25-mm socket. For the BPTB procedure, the same tibial guide was used and set at 55°. A guide pin was then placed through the central aspect of the tibial footprint. A fully fluted reamer was then used to create a full tunnel. For the quadriceps graft, a tibial button was used to stabilize the graft in the tibial tunnel. For the BPTB graft, we used an interference screw with a diameter 1 mm less than the graft diameter. In both techniques, the graft was tensioned with the knee in full extension and a posterior drawer placed on the knee.
Postoperatively, patients wore a lockable hinged knee brace locked in extension but were allowed to ambulate on the knee as tolerated with crutches for 2 weeks. Patients with meniscal repairs used crutches for a total of 4 weeks. At the 2-week period, the brace was unlocked to 90°, and brace use was discontinued at 6 weeks. The physical therapy protocols were the same for both groups regardless of the graft used. Focus was initially placed on gaining full range of motion of the knee followed by strengthening. Typically, jogging was allowed at 3 months with progression to sprinting. Cutting and pivoting activities were allowed at 6 months. Return to sport was determined by the senior surgeon based on appropriate progression through the rehabilitation program and physical therapist's reports regarding quadriceps strength and mobility. Return to sport was defined objectively as participation in an official game within the chosen sport within the 2-year follow-up period.
Outcomes Evaluation
Patients were divided according to graft type into the BPTB and QST groups. The International Knee Documentation Committee (IKDC) subjective knee evaluation and the Lysholm Knee Scoring Scale were administered by research coordinators and used to evaluate patient-reported outcomes for all patients. Forms were collected preoperatively and at 6, 12, and 24 months postoperatively. Retrospective chart review was utilized to obtain information regarding return to sport at previous level of competition and complications (retear, arthrofibrosis, and infection). Retear rates were assessed by performing a physical examination with negative Lachman and anterior drawer tests. Suspected retears based on physical examination were confirmed by magnetic resonance imaging. Arthrofibrosis was diagnosed with postoperative range of motion limitations later requiring manipulation under anesthesia or arthroscopic resection.
The improvement in IKDC and Lysholm scores from preoperatively to 2-year follow-up was compared between the BPTB and QST groups. In addition, we compared the rate of achieving previously established 2-year minimal clinically important difference threshold values for the IKDC (9.5 points) and Lysholm (10.6 points) between groups. 23
Statistical Analysis
Patient characteristics and knee outcome scores in each group were tested for normality with the Shapiro-Wilk test. For continuous variables, when the Shapiro-Wilk test departed significantly from normality (P < .05), the Mann-Whitney test (2 independent groups) was applied, otherwise a Student t test was utilized. The chi-square test was employed for categorical variables. A P value <.05 was considered statistically significant. Statistical analysis was performed using SPSS software Version 25.0 (SPSS Inc).
Results
A total of 78 ACLRs were performed on cutting and pivoting athletes with either BPTB (n = 42) or QST (n = 36) autograft over the 4-year period. In the BPTB group, 6 athletes were lost to follow-up, leaving a remaining total of 36 patients in the BPTB group with 2-year follow-up (86% follow-up). In the QST group, 4 athletes were lost to follow-up, leaving a remaining total of 32 patients in the QST group with 2-year follow-up (89% follow-up). A modified CONSORT (Consolidated Standards for Reporting Trials) flow diagram is provided in Figure 1.

Flow diagram of patient enrollment. BPTB, bone-patellar tendon-bone; QST, quadriceps soft tissue.
Demographic information is included in Table 1. Mean age was 17.6 years (range, 14-22 years) for the QST and 18.3 years (range, 15-24 years) for the BPTB autograft group (P = .28). There were no significant group differences with respect to patient sex, level of participation, body mass index, involved leg, type of sports participation, or rate of concurrent meniscal surgery.
Patient and Surgery Characteristics a

BMI, body mass index; BPTB, bone-patellar tendon-bone; QST, quadriceps soft tissue.
The IKDC and Lysholm scores are reported in Figure 2. Preoperative, 6- and 12-month IKDC scores were similar between groups, as were the 2-year postoperative IKDC scores (QST, 90.5 ± 6.6; BPTB, 89.7 ± 7.8; P = .92). Two-year Lysholm scores higher than 84 (good to excellent results) were observed in 88% of patients in the QST group, and 75% in the BPTB group. 5 When stratified according to sex, 2-year IKDC scores were comparable for male (92.2) and female (89.3) athletes in the QST group, as well as for males (92.4) and females (87.3) in the BPTB cohort. Similarly, the preoperative, 6- and 12-month Lysholm scores were similar between the groups, as well as the 2-year postoperative Lysholm scores (QST, 91.3 ± 7.5; BPTB, 90.5 ± 8.6; P = .92). When isolated by sex, 2-year Lysholm scores were similar for male (92.2) and female (90.7) athletes in the QST group as well as males (93.3) and females (88.0) in the BPTB cohort.

Mean (A) IKDC and (B) Lysholm scores at the preoperative and postoperative 6-month, 1-year, and 2-year evaluations for the QST and BPTB groups. Standard error bars included. BPTB, bone-patellar tendon-bone; IKDC, International Knee Documentation Committee; postop, postoperative; preop, preoperative; QST, quadriceps soft tissue.
The percentage of athletes able to return to play within the 2-year follow-up period was similar between groups. Of the athletes in the QST autograft group, 28 (88%) returned to play within their chosen sport, and of the athletes in the BPTB autograft group, 30 (83%) returned to their sport (P = .63). The complication rates were also not significantly different between the 2 groups (Table 2). Two patient in the BPTB group sustained a graft retear, while no retears were noted in the QST group. Arthrofibrosis requiring manipulation under anesthesia and arthroscopic lysis of adhesions occurred in 4 patients in the BPTB group and 2 in the QST group. Contralateral ACL rupture occurred in 4 patients of the BPTB group and 1 patient in the QST group. There were no infections in either group.
Complication Rates a

Data are reported as n (%). ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; QST, quadriceps soft tissue.
At the 2-year postoperative assessment, the QST group IKDC score improved 40.4 points and Lysholm improved 39.9 points compared with preoperative scores (Table 3). Similarly, the BPTB group IKDC score improved 39.1 points and Lysholm improved 38.6 points over the 2-year period. Every patient in both groups achieved the previously established 2-year minimum IKDC (9.5 points) and Lysholm (10.6 points) values (Table 3). 23
Postoperative Outcome and MCID Threshold Achievement a
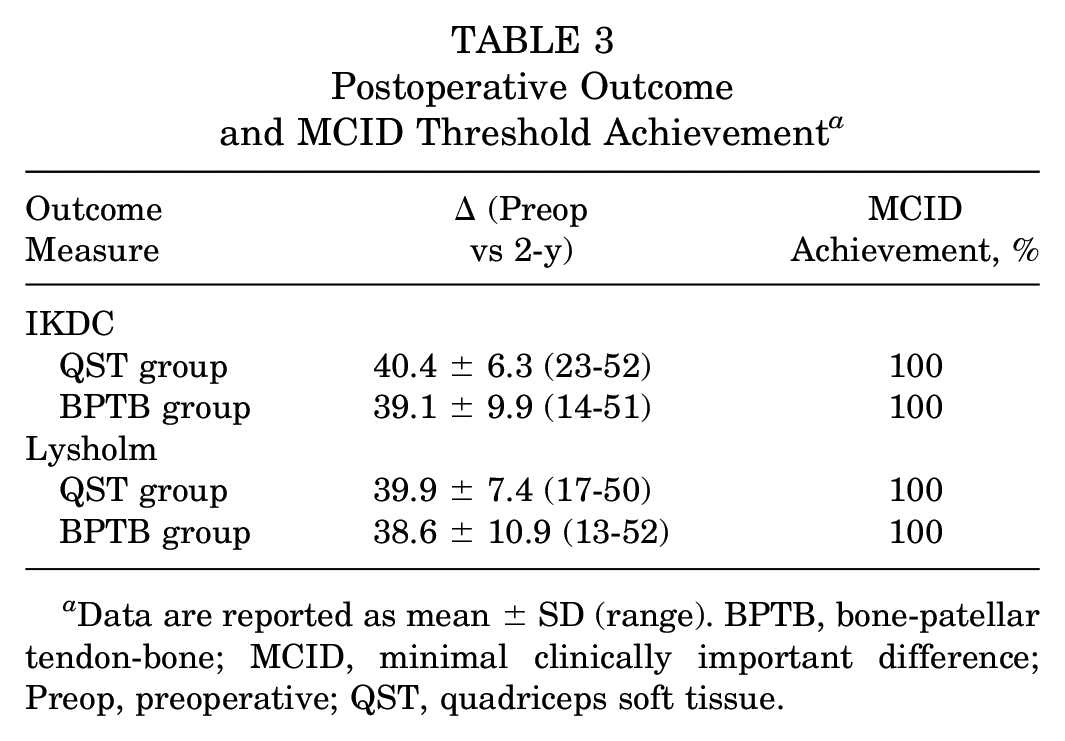
Data are reported as mean ± SD (range). BPTB, bone-patellar tendon-bone; MCID, minimal clinically important difference; Preop, preoperative; QST, quadriceps soft tissue.
Discussion
In this retrospective study, we found similar patient-reported outcomes and return-to-sport rate at the 2-year follow-up in cutting and pivoting athletes who underwent ACLR with BPTB versus QST autografts. Complication rates including retear, arthrofibrosis, and contralateral ACL tears were also similar between the 2 study groups.
Our results revealed similar patient-reported outcome scores between the 2 cohorts. Two-year Lysholm scores higher than 84 (good to excellent results) were observed in 88% of patients in the QST group and 75% in the BPTB group. 5 When further isolated by sex, 2-year Lysholm scores were similar for male (92.2) and female (90.7) athletes in the QST group but were slightly superior in male athletes (93.3) compared with female (88.0) athletes in the BPTB cohort. This is consistent with previous reports comparing outcomes of QST and BPTB graft reconstructions that have failed to show any notable differences with respect to function, patient-reported outcomes, or residual laxity.9,15 Specifically, a systematic review and meta-analysis by Mouarbes et al 22 compared outcomes of quadriceps tendon autograft, BPTB, and HT autografts in 2856 subjects and found that QST autografts had comparable functional outcomes and graft survival when compared with BPTB grafts. However, this review included heterogeneous patient populations without a specific focus on cutting and pivoting athletes. 22 Results in our series reflect the current literature in that there were similar functional outcomes between QST and BPTB autografts, although further studies in the athletic population may offer more clarity.
We found similar rates of arthrofibrosis between the 2 cohorts. Our findings align with previous reports of acceptable risk of arthrofibrosis and contralateral ACL tears utilizing quadriceps tendon graft.25,26 Other studies have also evaluated donor site morbidity as a long-term complication. GorSchewsky et al 9 noted a significantly higher rate of donor site morbidity in the BPTB group compared with the QST group. Lund et al 19 reported less kneeling pain, graft site pain, and sensitivity loss in QST grafts compared with BPTB, despite similar anterior knee stability and subjective outcomes. The systematic review and meta-analysis by Mouarbes et al 22 found that quadriceps tendon autografts had comparable functional outcomes and graft survival, but they had less donor site morbidity than BPTB grafts and better functional scores than HT autograft reconstructions. Taken together, these data suggest that quadriceps tendon autograft may afford a similar complication rate with less graft site morbidity when compared with the patellar tendon autograft.
It remains important to evaluate complication rates with regard to retears and contralateral ACL tears between different graft types. In our series, there were similar retear rates, with no retears in the QST and 2 retears in the BPTB cohort. In contrast to this study, a Danish study using results from a large knee ligament registry noted that patients treated with QST grafts, with or without a bone block, had higher revision rates than those treated with BPTB or HT grafts. Both younger patients and those involved in sports were at particularly high risk if treated with QST grafts; however, the QST cohort reported a greater share of meniscal and cartilage injuries at the time of surgery. In addition, as mentioned by the authors, the registry included a mix of techniques and harvesting systems in obtaining QST grafts. 17 In our series, the share of meniscal injuries were similar between groups and all procedures were performed by a single surgeon using 1 technique and harvesting system. The rate of contralateral ACL tears was similar between groups, indicating that 1 particular graft type does not put athletes at increased risk of injury to the contralateral ACL. Finally, the percentage of athletes able to return to sport within the 2-year follow-up period was similar between groups. Taken together, these findings suggest athletes were able to return to the highest level of play within 2 years of ACLR without an increased risk of retears or rupture of the contralateral ACL. The similar return to sport provides context to the comparable complication rates as athletes participating in contact sports have known higher risk of reinjury. Studies with a higher power, prospective design, or more control could offer more insight into the return-to-sport factors and risk of revision or retear between these 2 graft options in the athletic population. 8
Limitations
Our study has several limitations. First, it is limited in nature as a retrospective study. Although the series was a consecutive group of patients treated by a single surgeon, there is inherent possibility of selection bias between the 2 cohorts as there was no structured randomization. However, our comparison between the 2 cohorts revealed similar demographic differences. Second is the lack of rigorous statistical power analysis and possibility of a type 2 error given the size of our patient cohorts. Sample size estimations were performed on 2-year IKDC and Lysholm scores to determine the number of participants required to generate a statistically significant difference between the 2 groups. Assuming an alpha of .05 and power of 80%, the sample size required to generate a difference between the 2-year IKDC scores for BPTB and QST groups were 1828 and 1609, respectively. Similarly, the 2-year Lysholm scores for BPTB and QST groups required sample sizes of 1898 and 1670, respectively. Third, our return-to-play criterion is particularly prone to confounding variables as it is dependent on the athlete's desire to continue playing his or her chosen sport. We chose to include it in our analysis because it may serve as an indicator whether the athlete was able to return to the highest level of play without restrictions. In addition, it provides context to the potential increased risk of complications if groups were discovered to differ substantially with regard to return to sport. Future studies may consider a more objective criterion for measuring the athlete's ability to safely return to athletics without restrictions. Lastly, our analysis did not include objective biomechanical factors that may reveal further differences between the 2 groups.
Conclusion
The optimal ACL graft in high-level athletes participating in cutting and pivoting sports remains in question. In our comparison of quadriceps autograft compared with BPTB autograft in this athletic population, similar patient-reported outcomes, 2-year IKDC scores, 2-year Lysholm scores, and retear rates were identified. These findings suggest that the QST autograft may be as effective as BPTB autografts in cutting and pivoting athletes, may allow athletes to return to play without an increased risk for retear and should be brought up in the graft selection discussion with these athletes.
Footnotes
Final revision submitted April 10, 2023; accepted May 4, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.V.T. has received education payments from ImpactOrtho. K.J.E. has received education payments from Goode Surgical and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from WCG IRB (No. 20216101).