
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) surgery with quadriceps tendon (QT) grafts, both with and without a patellar bone plug, have gained popularity in recent years in the primary and revision settings. Postoperative complications occur with the use of QT autografts.
Purpose:
To systematically review the incidence of postoperative complications after primary ACLR QT autograft and compare complication rates in patients undergoing all-soft tissue QT grafts versus QT grafts with a patellar bone plug (QTPB).
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search using the 2020 PRISMA guidelines was performed by querying PubMed, Embase, and Scopus databases from database inception through August 2022. Included were evidence level 1 to 4 human clinical studies in English that reported complications after primary ACLR with QT autograft. The incidence of complications within the included studies was extracted. Differences in the incidence of postoperative complications between ACLR with QT with and without a patellar bone plug were calculated.
Results:
A total of 20 studies from 2004 to 2022, comprised of 2381 patients (2389 knees; 68.3% male) with a mean age of 27 years (range, 12-58 years), were identified. The mean follow-up was 28.5 months (range, 6-47 months). The total incidence of complications was 10.3%, with persistent postoperative knee pain being the most common (10.8%). Patients who underwent ACLR with all-soft tissue QT grafts had a 2.7-times increased incidence of anterior knee pain (23.3% vs 8.6%) and reoperations (5.9% vs 3.2%) when compared with QTPB grafts (P < .01 for both). There was no appreciable difference in total complications, graft failures, ACLR revisions, cyclops lesions, or range of motion deficit (P > .05 for all). Patellar fractures occurred exclusively after QTPB (2.2%).
Conclusion:
Complications after primary ACLR using QT autograft were recorded in 10.5% of knees, with anterior knee pain being the most common. No difference was reported in the overall incidence of complications with the use of the QT versus QTPB grafts; however, anterior knee pain was 2.7 times greater with use of a soft tissue quadriceps graft.
Despite decades of advancements in anterior cruciate ligament (ACL) reconstruction (ACLR) surgery, debate remains over the ideal graft choice. Graft choice must consider mechanical properties, integration, and the associated complication profile of each graft.6,30 Autografts of the hamstring tendon or bone-patellar tendon-bone (BTB) grafts have been used predominantly for their relative ease of harvest, well-documented tensile strength, and extensive outcome data in the literature.2,35 However, quadriceps tendon (QT) grafts, both with and without a patellar bone plug, have gained popularity in recent years in both the primary and revision setting. Specific advantages of QT grafts include increased intra-articular graft volume and collagen relative to patellar tendon grafts. 47 This has been concurrent with an effort to address the reported shortcomings of other graft options, as well as in cases where a hamstring or BTB graft was previously harvested. 38 Promising anatomic, histologic, and biomechanical characteristics, as well as recent evidence demonstrating functional outcome scores comparable with those of BTB grafts, have further compounded the growing interest in the use of QT grafts.3,40,47
Historically, the most common complications after ACLR with autograft are anterior knee pain and decreased range of motion (ROM). 44 The rates of this complication vary among ACL graft choices. A meta-analysis by Mouarbes et al 30 revealed donor-site pain rates of between 8.0% and 18.4% in QT autografts, 22.2% in hamstring tendon autografts, 40.4% in BTB autografts, and 26.0% in allografts. In QT autografts, the use of a central strip of the quadriceps offers the benefits of preserved knee flexor function with decreased risk for kneeling pain and anterior numbness, relative to the commonly used hamstring and BTB autografts.9,11,36 Nevertheless, with QT autografts, extensor mechanism weakness in the donor limb and early extension deficits have been reported as areas of concern.16,27,31 Since the QT has a rich blood supply, patients may also be predisposed to postoperative hematoma formation, particularly with added bone bleeding when a patellar plug is harvested. 39
Both all-soft tissue QT and QT with patellar bone plug (QTPB) techniques have demonstrated favorable outcomes. 11 Similar to a BTB, the use of QTPB offers the benefit of more rapid, bone-to-bone healing within the femoral tunnel and may be preferable in the setting of enlarged tunnels after failed primary reconstruction. 9 Conversely, harvesting of a patellar bone plug can increase donor-site morbidity and poses a risk for patellar fracture, which has been reported to occur in up to 8.8% of cases, especially when an eccentric harvest is performed.9,33,36,44 Despite these findings, there have been no significant differences reported regarding complications between the all-soft tissue QT and QTPB techniques.
The purpose of the present study was to systematically review the incidence of postoperative complications and adverse events after primary ACLR with QT autograft and compare complication rates between the all-soft tissue QT and QTPB techniques.
Methods
Search Strategy and Selection Criteria
This systematic review was conducted according to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines. 32 The PubMed, EMBASE, and Scopus databases were searched on August 16, 2022, by 2 independent authors (initials blinded for peer-review) using the following Boolean search criteria: ((Anterior cruciate ligament) OR (ACL)) AND (Quadriceps Tendon) AND (Reconstruction). The inclusion criteria consisted of evidence level 1 to 4 human clinical studies published in English or English-language translation reporting the presence or absence of complications after primary ACLR using a QT autograft, either with or without a patellar bone plug. Exclusion criteria consisted of cadaveric, animal, or biomechanical studies, case reports, review articles, expert opinions, and studies without any report of complications after primary ACLR with QT autograft. Studies reporting on revision procedures or studies that included concomitant ligamentous repair or reconstruction procedures (posterolateral corner, lateral extra-articular tenodesis, medial collateral ligament, posterior cruciate ligament, lateral collateral ligament) were not included. Studies in which concomitant meniscal repair or partial meniscectomy was performed were not excluded to more accurately reflect clinical practice, as concomitant meniscal pathology is commonly encountered during ACLR. 21
Two authors (G.J. and T.T.) independently screened the articles by title, abstract, and full text, as appropriate. Initial title and abstract screening was performed on 1939 studies, from which 85 full-text studies were assessed for eligibility. Any disagreements were discussed with a third author (E.M.), and a consensus was reached. Ultimately, 20 full-text studies meeting inclusion/exclusion criteria were eligible for data extraction (Figure 1).
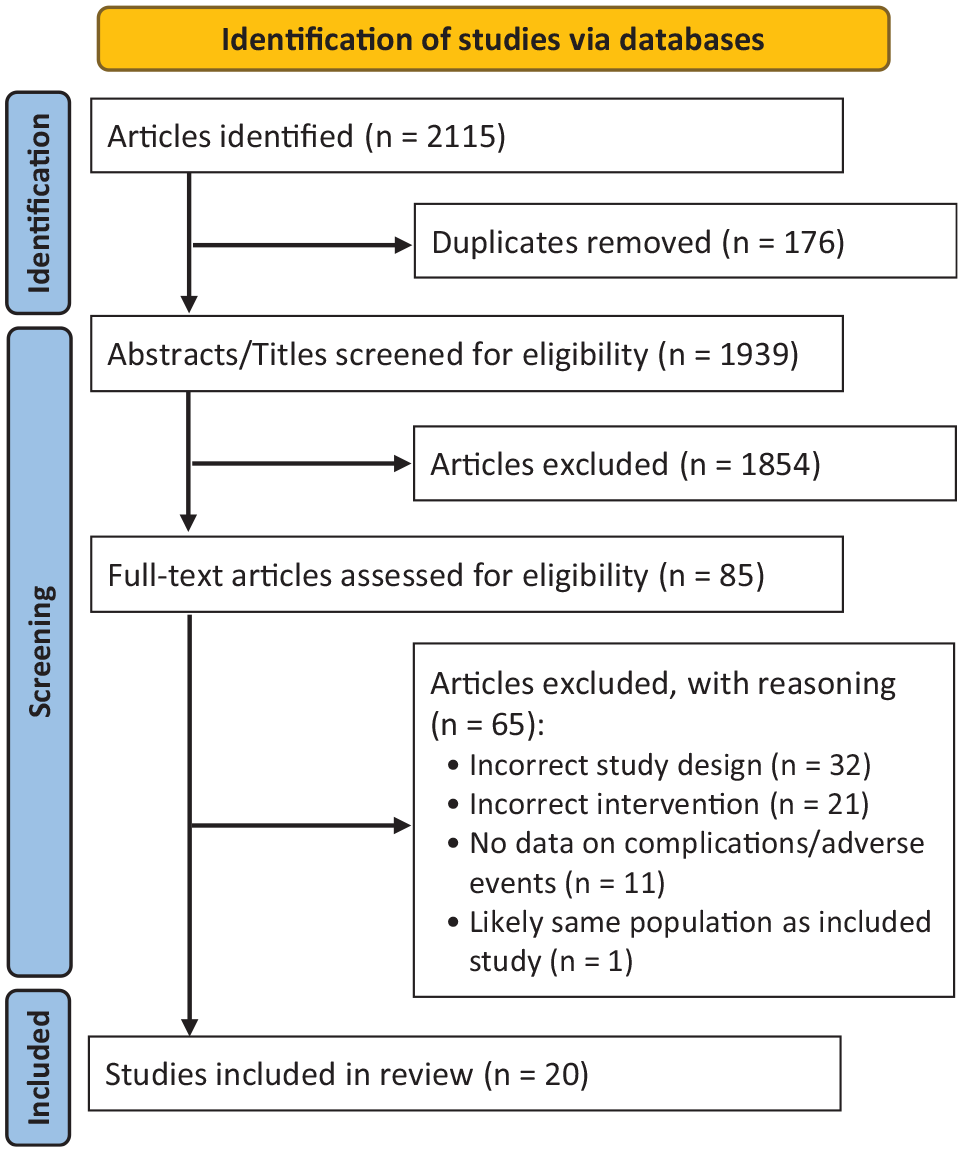
PRISMA diagram demonstrating study selection process. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis
Data Extraction
A customized Microsoft Excel Version 16.63 spreadsheet was created to extract all relevant data from included studies. Study characteristics, including author name, year, study design, patient number, sex, age, follow-up, and graft type, were then extracted. In addition, the details of adverse events and complications collected were as follows: total failures, reoperations, ACL revisions, patellar fracture, cyclops lesion, ROM deficit, and persistent instability. If complications or adverse events did not fit into the aforementioned categories, they were recorded as “other.” Failure was defined by traumatic or nontraumatic ACL graft rerupture.
Statistical Analysis
The incidence of reported complications and adverse events was calculated. If a study did not report the presence or absence of the complication in question, it was not included in the calculation of incidence for that specific complication. To further analyze potential group differences between QT and QTPB grafts, a 2-proportion z test was performed. The statistical significance for this review was set to P < .05.
Results
Demographic Data
A total of 20 studies with a total pooled sample of 2381 patients (2389 knees) were identified and evaluated. # The mean patient age was 27 years (range, 12-58 years), and 68.3% of patients were male (1626of 2381). The mean follow-up was 28.5 months (range, 6-47 months). There was 1 study with level 1 evidence, 15 5 studies with level 2 evidence,12,13,18,25,27 10 studies with level 3 evidence, ** and 4 studies with level 4 evidence.11,23,24,46 The characteristics of the included studies are summarized in Table 1.
Study Characteristics a

QT, quadriceps tendon; QTPB, quadriceps tendon with patellar bone plug.
Overall Complications
The overall incidence of reported complications after primary ACLR with a QT graft was 10.3% (246 of 2389 knees). The most commonly reported complication was anterior knee pain, with a 10.8% incidence (91 of 843 knees), as reported in 11 studies. †† The second most common complication was the development of a cyclops lesion, with an estimated incidence of 4.9% (23 of 472 knees; reported in 4 studies).5,17,18,25 The incidence of instability was estimated at 4.4% (9 of 206 knees; reported in 4 studies)18,22,24,40; patellar fracture at 2.2% (n = 10 of 464 knees; reported in 5 studies)14,18,23,24,46; ROM deficit at 2.2% (n = 11 of 500 knees; reported in 4 studies)13,14,18,23; and infection at 1.4% (n = 4 of 286 knees; reported in 6 studies).1,13,27,25,46,15 The surgical failure rate in the pooled sample was 3.1% at a mean 38.1-month follow-up (n = 72 of 2354 knees; reported in 19 studies). ‡‡ The reoperation rate was estimated at 4% (n = 93 of 2313; reported in 18 studies), §§ with revision ACLR being the most common reoperation, reported in 2.4% of knees (n = 55 of 2313; reported in 18 studies) (Tables 2 and 3). §§
Overall Incidence of Complications After ACLR With All-Soft Tissue QT Graft a

ACLR, anterior cruciate ligament reconstruction; DVT, deep venous thrombosis; IR, incidence rate; QT, quadriceps tendon; ROM, range of motion.
Incidence of Complications After ACLR with All-Soft Tissue QT by Graft Type a

Dashes indicate areas not applicable. Boldface P values indicate statistically significant difference between graft types (P < .05). ACLR, anterior cruciate ligament reconstruction; DVT, deep venous thrombosis; IR, incidence rate; QT, quadriceps tendon; QTPB, quadriceps tendon with patellar bone plug; ROM, range of motion.
Subgroup Analysis (QT vs QTPB)
When comparing outcomes of ACLR using all-soft tissue QT versus QTPB, 35.5% (847 knees) of knees used an all-soft tissue QT, while 64.5% (1542 knees) used a QTPB. No significant difference was appreciated between groups in the overall reported incidence of complications. The reported incidence of anterior knee pain and reoperations were significantly higher with use of an all-soft tissue QT graft (P < .00001 and P = .01, respectively) (Table 3). Patellar fractures were only reported with the use of the QTPB (2.2%; 10 of 464 knees). There was no significant difference between groups in ACLR revisions, cyclops lesions, or ROM deficits (P > .05 for all). While not significant, patients undergoing QTPB had higher rates of failures (3.1 vs 1.6; P = .06), while those undergoing all-soft tissue QT had a great number of total complications (12.3% vs 9.6%, P = .08).
Discussion
The main findings from this study were that the reported incidence of postoperative complications across studies examining ACLR using a QT autograft is 10.3%, with persistent anterior knee pain being the most common. The failure rate at a mean follow-up of 38.1 months was estimated at 3.1%, with a reoperation rate of 4%. The incidence of overall complications was similar after ACLR using all-soft tissue QT versus QTPB grafts, while higher rates of anterior knee pain were appreciated in patients treated with an all-soft tissue QT graft.
Our review of the available literature yielded a 10.8% incidence rate of anterior knee pain throughout 11 studies reporting on complications after ACL using QT autograft. †† That rate is lower than that reported in BTB graft cohorts. Specifically, a retrospective study by Geib et al 11 of 191 patients reported anterior knee pain to be present in 26% of patients after BTB ACLR, and a previous systematic review by Mouarbes et al 30 showed a rate of anterior knee pain in BTB ACLR as high as 40.4%. Interestingly, on subgroup analysis, all-soft tissue QT grafts had a significantly higher rate of persistent anterior knee pain relative to QTPB, reflecting the multifactorial physiopathology behind anterior pain after graft harvest. Comparable with the anterior knee pain observed after hamstring autograft harvest, this finding aligns with the concept that donor site morbidity of a bone plug harvest is likely not the only factor responsible for this complication. 28
Although there is currently no consensus on the etiology of knee pain associated with ACLR, in a case series examining patient-reported pain when pulling tension was applied to the graft with a hook, Biedert et al 4 demonstrated that ACL grafts present noxious sensory innervation, suggesting that anterior knee pain in ACLR may be associated more with mechanical forces on the graft itself than with donor site morbidity. This is further corroborated by literature consistently finding lower donor site morbidity in QT grafts than in BTB grafts.8,29 Other plausible etiologies for the development of anterior knee pain in ACLR include incomplete closure of the QT defect after harvest, scar orientation, and effective implementation of rehabilitation protocols emphasizing recovery of terminal extension. Failure to obtain full knee extension postoperatively, as well as quadriceps weakness, regardless of the type of graft used, are associated with anterior knee pain due to relative overload of the patellofemoral joint as a result of deconditioning after the procedure.7,28,37 A study by Hunnicutt et al 17 corroborated these findings in all-soft tissue QT graft use, with the authors reporting decreased quadriceps strength and increased extension deficit, particularly in female patients. A possible explanation behind the increased anterior pain rate found in all-soft tissue QT versus QTPB is the potential for more aggressive and more proximal dissection of the quadriceps in all-soft tissue graft harvest, in an effort to maximize graft length, which may lead to decreased extensor mechanism strength postoperatively. Further study is warranted to confirm this as a potential etiology behind the increased rate of anterior knee pain.
Postoperative loss of knee ROM is historically among of the most commonly encountered complications after ACLR. Our review found a 2.2% rate of postoperative loss of ROM among included studies using QT and QTPB grafts. That value is likely underestimated, as most studies reported ROM as mean angular values as opposed to the proportion of patients in which it occurred. Furthermore, the 4.9% incidence of cyclops lesions in our pooled sample suggests an additional cohort of patients that had impaired terminal extension at follow-up.
Patellar fracture was found to occur in 2.2% of the pooled sample. There is still a paucity of literature on patellar fracture after QTPB harvest relative to BTB harvest. Although rare, patellar fractures are a devastating consequence and directly related to weakened bone after graft harvest.10,41,43 A study by Fu et al 10 describes eccentric harvest, harvesting of more than 50% of the anteroposterior thickness or of the mediolateral width, and stress risers at the corner of the graft harvest site as potential risk factors for iatrogenic patellar fracture after QTPB ACLR. 33 In a biomechanical analysis, Perry et al 33 demonstrated significantly less remaining patellar bone in a lateral column QT graft harvest compared with a medial column harvest, potentially demonstrating a risk for patellar fracture.
In terms of graft failure and revision, incidence rates of 3.1% and 2.9%, respectively, were observed. Those are in line with previously reported failure and revision rates, regardless of graft type. Specifically, Kaeding et al 20 reported an ipsilateral graft tear rate of approximately 4% in the Multicenter Orthopaedic Outcomes Network (MOON) cohort, comprised 2683 patients at minimum 2-year follow up. Moreover, data from 21,846 patients in the Swedish National Knee Ligament Register who underwent primary single-bundle ACLR yielded a 3.2% revision rate at 2 years. 42 Meanwhile, Lind et al 26 reported higher revision rates in patients undergoing ACLR using QT autografts (4.7%) when compared with BTB (1.5%) or hamstring grafts (2.3%) in their retrospective study of the Danish Knee Ligament Registry. However, the influence of graft size, fixation type, use of bone plug and overall technique were not analyzed as separate variables. 26 Further studies are needed to elucidate the reasons behind potential differences in failure rates after ACLR using QT autograft.
Limitations
The present review is not without limitations. Both full-thickness and partial-thickness grafts were included in the sample without differentiation, as (1) not every included study described their surgical technique in sufficient detail, and (2) current literature still shows no differences in outcomes and complications between full- versus partial-thickness grafts. In addition, study designs may affect the reporting of complications and adverse events as they are impacted by recall or information bias, possibly altering the frequency and severity of adverse events reported. Specific concerns surrounding the use of QT grafts often include the potential for postoperative hematoma and a less favorable cosmetic appearance. These factors, however, were not reported consistently throughout the available literature, highlighting the need for more detailed reporting of complications in future prospective studies. However, the study by Todor et al 45 did observe that 12% of patients were unsatisfied with the postoperative cosmetic aspect of the surgery. In addition, the inclusion of retrospective studies also downplays the incidence of resolved postoperative loss of ROM, as they are subject to recall bias since patients are not as likely to remember and report transient issues. Therefore, reported outcomes may differ between study designs. Furthermore, the mean follow-up of the included studies was relatively short mean (28.5 months). Ultimately, as is the case in all systematic reviews, our search strategy and eligibility criteria might have unintentionally precluded the inclusion of relevant data.
Conclusion
Complications after primary ACLR using QT autograft were recorded in 10.5% of knees, with persistent knee pain being most common. No difference was reported in the overall incidence of complications with the use of the QT versus QTPB grafts; however, persistent knee pain was 2.7 times greater with use of a soft tissue quadriceps graft.
Footnotes
Final revision submitted March 28, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.R.M. has received education payments from Medwest Associates. O.A.O. has received education payments from Medwest Associates. D.M.K. has received education payments from Arthrex, Elite Orthopedics, and Smith & Nephew; honoraria from Encore Medical; hospitality payments from Stryker; and grant support from Arthrex. N.N.V. has received consulting fees from Arthrex, Smith & Nephew, Medacta, and Stryker; nonconsulting fees from Arthrex; education payments from Medwest Associates; royalties from Arthrex, Smith & Nephew, and Graymont Professional Products; speaking fees from Arthrex; and hospitality payments from Relievant Medsystems. J.C. has received education payments from Smith & Nephew and Arthrex; consulting fees from Smith & Nephew, Vericel, Arthrex, DePuy Synthes Products, and Linvatec; nonconsulting fees from Smith & Nephew, Linvatec, and Arthrex; hospitality payments from Stryker; and grant support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.