
Abstract
Background:
Ulnar collateral ligament (UCL) injuries occur frequently in baseball players, and UCL reconstruction is performed when nonoperative treatment fails.
Purpose:
To compare a novel all-suture anchor method of UCL reconstruction with a method using bone tunnels (Ito method) by investigating the displacement against valgus torque and the failure strength.
Study Design:
Controlled laboratory study.
Methods:
Eight fresh-frozen cadaveric upper extremities (mean age, 82.0 years) were utilized in this study. To evaluate the displacement against valgus torque, the valgus stability test was performed for 4 anterior oblique ligament (AOL) conditions: intact AOL, resected AOL, reconstructed using the anchor method, and reconstructed using the Ito method. The load-to-failure test was performed to evaluate the failure strength of the anchor and Ito methods. Displacement against valgus load was compared between conditions using the repeated-measures 2-way analysis of variance with Bonferroni post hoc test, and failure strength between the anchor and Ito methods was compared using the unpaired t test.
Results:
Displacements of the intact AOL and anchor method were significantly greater than those of the resected AOL at both 60° and 90° of flexion (intact AOL: P = .005 and P < .001, respectively; and anchor method: P = .024 and P < .001, respectively). The displacement of the Ito method at 90° of flexion was significantly greater than that of the resected AOL (P = .003), but no significant difference was observed at 60° of flexion (P = .109). There were no significant differences in displacement between the anchor and Ito methods at any flexion angle, nor was there a significant difference in failure torque between the anchor and Ito methods (16.3 ± 3.1 vs 17.6 ± 2.3 N·m, respectively; P = .537).
Conclusion:
The displacement and failure strength against a valgus load after UCL reconstruction using a suture anchor on the ulnar side were equal to those using bone tunnels.
Clinical Relevance:
UCL reconstruction using a suture anchor on the ulnar side is simpler and less invasive than using bone tunnels, with similar outcomes.
The ulnar collateral ligament (UCL) is the primary static stabilizer of valgus stress at the elbow.13,25,29 UCL injuries are often caused by the valgus stress that occurs during the late cocking and early acceleration phases of throwing and are therefore relatively common in baseball pitchers. 14 UCL reconstruction is a well described and frequently performed surgical technique utilized to correct UCL injuries in these athletes.11,21,32,35 UCL reconstruction was first described by Jobe et al, 18 and various surgical methods have been reported to improve the rates at which athletes are able to return to play by as much as 78% to 91%.4,10,20,23,32 Despite being a well-described technique, a number of postoperative complications have been reported, with ulnar nerve-related complications being especially interesting due to their poor clinical outcomes and need for further surgical procedures.5,9,24 While the rate of ulnar nerve-related complications has decreased due to improvements in surgical methods, including selective transposition of the ulnar nerve and the muscle-splitting approach,5,9 and despite having no effect on return to play, the incidence remains high, with complications occurring in 16% of cases (121 of 756 elbows) after UCL reconstruction by the modified Jobe method. 5
Importantly, the distance to the ulnar nerve can be particularly small when creating a bone tunnel to the posterior ulna, so it is necessary to consider a less invasive method to avoid postoperative complications. Furthermore, although intraoperative cut-out between tunnels of the ulna is not a common complication, it is a potential risk in Japanese and other Asian populations due to their smaller bone size compared to Western populations. As such, the development of a less invasive method for UCL reconstruction is of increasing interest in biomechanical research. ‡
One method that we consider to be a simpler and less invasive approach utilizes only an ulnar-side suture anchor fixation. The purpose of this study was to compare the displacement and failure strength against a valgus load of this novel anchor method with an established method that uses 2 bone tunnels (Ito method). 16 We hypothesized that the stability and stiffness of the anchor method would be similar to those of the Ito method.
Methods
A total of 8 fresh-frozen cadaveric upper extremities (4 matched pairs comprised of 3 male and 1 female specimens provided by the Clinical Anatomy Laboratory of Chiba University) were utilized in this study. The age of the cadavers at death ranged from 74 to 92 years, with a mean age of 82 years. To determine the number of specimens to be included in our study, a power analysis was performed based on the primary outcome variable of displacement (mm) when the elbow was forced with a 5 N·m valgus torque. The effect size for our power analysis was based on the difference in displacement (a mean difference of 8 mm and a standard deviation of 5 mm) and failure torque (a mean difference of 4 N·m and a standard deviation of 2 N·m) reported in previous studies (β = 0.2, α = 0.05).2,3,7,15,17,25,26,31 The power analysis indicated that 7 specimens per group for the comparison of displacement, and 4 specimens per group for the comparison of failure torque were required. As such, we evaluated 8 elbows in total.
Specimen Configuration
The specimens were stored at −20°C and thawed overnight at room temperature; they comprised the distal half of the humerus, the entire forearm, wrist, and hand. The skin and subcutaneous tissues were removed, leaving the remaining soft tissues. Throughout preparation and testing, all specimens were kept moist with normal saline. The palmaris longus (PL) tendon and extensor digitorum communis (EDC) tendon of the middle finger were obtained from all specimens, and the width and length of the tendons were recorded and compared using the unpaired t test for the width and the Mann-Whitney U test for the length.
Each tendon was loaded with 2 kg of force for 10 minutes as a preload. The forearm was maintained in neutral rotation with 2 2.0-mm Kirschner wires inserted between the distal radius and ulna. The wrist was maintained in a neutral position with 2 or 3 2.0-mm Kirschner wires inserted between the radius or ulna and the carpal bones. The center of rotation of the humeroulnar joint was determined by radiography and marked by a 1.6-mm Kirschner wire inserted in the capitellum. Two ulnar bone tunnels were made 10 cm away from the center of rotation of the humeroulnar joint by a 1.6-mm Kirschner wire. Two strong strings were passed through the bone tunnels and fixed by a sewing button to pull the forearm to a valgus load of the elbow. All soft tissues of the upper arm more than 5 cm from the center of rotation of the humeroulnar joint were removed, and the humerus was exposed. The humerus was potted in a square paper carton with a height of 10 cm, length of 6 cm, and width of 4 cm containing polymethylmethacrylate cement. The humeral axis of the medial epicondyle to the lateral epicondyle, which was determined by a 1.6-mm Kirschner wire inserted into the capitellum, was kept parallel to the side of the paper carton. A straight stick was inserted into the humerus using polymethylmethacrylate cement to determine the longitudinal humeral axis. The polymethylmethacrylate cement around the humerus was grasped using a gripper fixed to the measurement table, and the longitudinal humeral axis was horizontally maintained above the floor. The elbow was held at an appropriate angle, and the 2 strong strings in the ulna were pulled vertically away from the floor to apply a valgus load to the elbow. The elbow flexion angle was controlled at 30°, 60°, 90°, and 120° by rotation of the gripper connector (Figure 1).

Apparatus configuration for the valgus stability and load-to-failure tests. Arrows indicate direction of application of valgus load.
Anterior Oblique Ligament Conditions
We investigated 4 anterior oblique ligament (AOL) conditions: intact AOL, resected AOL, reconstructed by the anchor method, and reconstructed by the Ito method (Figure 2). These conditions were compared using the valgus stability test and, to reduce bias, the stability testing was divided into 2 groups, in which 4 specimens underwent the anchor method before the Ito method (group AI), and the other 4 specimens underwent reconstruction in the reverse order (group IA) (Figure 3). The displacements of the anchor and Ito methods were compared between the AI and IA groups using the unpaired t test.

Cadaveric specimens showing the 4 study conditions: (A) intact AOL, (B) resected AOL, (C) after the anchor method, and (D) after the Ito method. AOL, anterior oblique ligament.

Flow diagram of groups AI (anchor method performed before Ito method) and IA (Ito method performed before anchor method). AOL, anterior oblique ligament.
Anchor Method
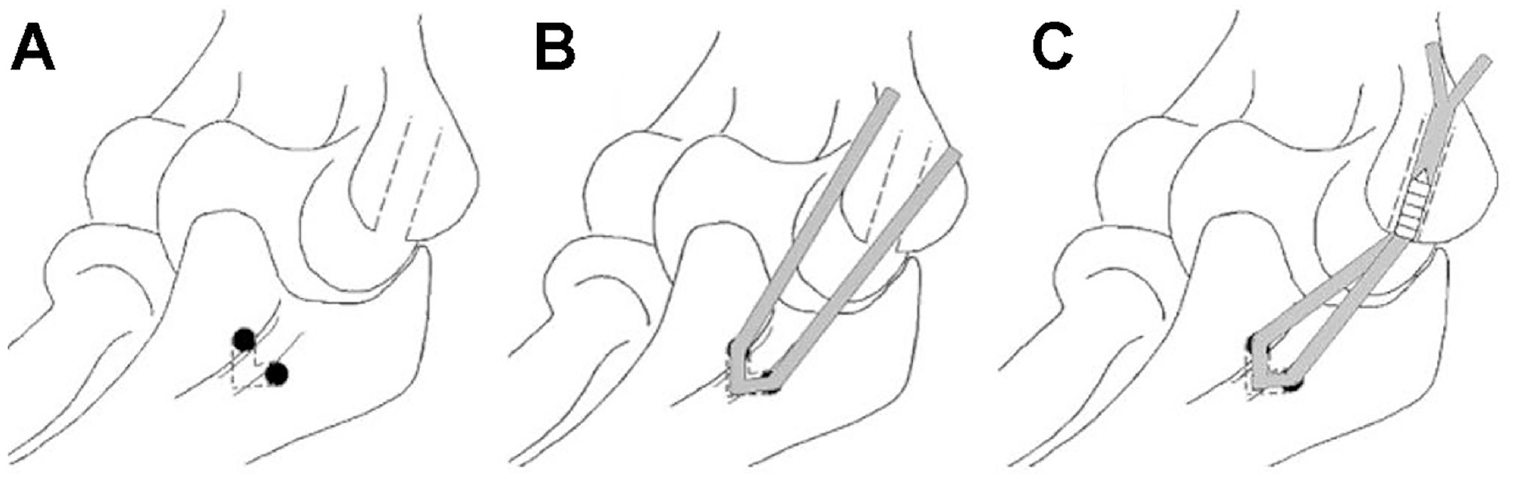
A 2.8-mm metal suture anchor (Twinfix; Smith & Nephew) was placed at the center of the native ligament footprint of the sublime tubercle, 10 mm distal to the joint line. On the humeral side, if the specimen was group IA, we used the same 5-mm bone tunnel as in the Ito method. For group AI, a 1.2-mm Kirschner wire was drilled into the medial epicondyle at the native ligament footprint as a guide pin, until the wire breached the far cortex of the medial epicondyle. Subsequently, a 5-mm bone tunnel was created through this Kirschner wire and the far cortex of the medial epicondyle was again breached (Figure 4A). The graft was folded in half and fixed to the suture anchor of the sublime tubercle using mattress and Krackow sutures (Figure 4B). Both graft ends were then passed through the humeral tunnel. Maximal manual tension was applied to the graft with the elbow in 60° of flexion, elbow varus, and forearm in the neutral position. A 5-mm absorbable interference screw (Milagro; Mitek) was inserted into the bone tunnel of the medial epicondyle to fix the graft ends with maximal manual tension applied (Figure 4C).

Procedure for the anchor method. (A) A 5-mm bone tunnel was created to the medial epicondyle, and the far cortex of the medial epicondyle was again breached. (B) The graft was folded in half and fixed to the suture anchor of the sublime tubercle. (C) A 5-mm absorbable interference screw was inserted into the bone tunnel of the medial epicondyle.
Ito Method
The Ito method, initially described by Ito in 2011, 16 is often performed in Japan. As the Ito method is similar to the Jobe and docking methods on the ulnar side and has been clinically proven to perform well in stability and load-to-failure biomechanical testing, we chose this technique to compare our novel anchor method with.9,17,20,21,23,31,34 A 3.5-mm drill was used to create bone tunnels on the anterior and posterior aspects of the sublime tubercle, connected by a bone bridge of approximately 2 cm. The tunnels were created approximately 15 mm distal to the joint line. On the humeral side, if the specimen was in group AI, we used the same 5-mm bone tunnel as in the anchor method. For group IA, we created a new 5-mm bone tunnel to the medial epicondyle using the same protocol as that of the anchor method (Figure 5A). The graft was then passed through the ulnar and humeral tunnels (Figure 5B). Subsequently, the graft was fixed using the same protocol as that of the anchor method (Figure 5C). Although the original Ito method uses a cortical bone screw from the ulna to fix the graft on the humeral side, we used an interference screw as we wanted to follow the same protocol as that of the anchor method and considered the strength of the cortical bone of the cadaveric specimen to be low.
Procedure for the Ito method. (A) A 5-mm bone tunnel to the medial epicondyle was created using the same protocol as that of the anchor method. (B) The graft was passed through the ulnar and humeral tunnels. (C) The graft was fixed using the same protocol as that of the anchor method.
Testing Protocol and Measurements
The valgus stability test was performed as per a previous study using a 50 N (5 N·m) valgus torque with loading of 1 mm/s using a traction system (Autograph; Shimadzu). 31 To determine the displacement against a valgus load, the displacement of the actuator was monitored using a personal computer. The displacement was measured under the 4 AOL conditions using the same protocol, with preload of 0.1 to 0.5 N·m applied 3 times, followed by a 5-N·m valgus moment to the elbow. The displacement was measured with the elbow at 90°, 60°, 30°, and 120° of flexion, in that order. To evaluate the influence of multiple measurements, such as tendon stretching and soft tissue damage, the displacement at 90° of flexion was measured again after measurements at each angle were completed when the anchor and Ito methods were tested, and the results of the first and second measurements were compared using a paired t test.
After the valgus stability test of the intact AOL, each specimen was dissected to expose the UCL using a muscle-splitting approach. A longitudinal incision was made in the posterior one-third of the common flexor mass adjacent to the flexor carpi ulnaris. The flexor muscle was gently separated from the UCL-capsular complex, and retractors were placed to fully expose the AOL. The AOL was resected to create a model of complete insufficiency. After the measurement of displacement in the resected AOL condition, the 2 reconstruction methods were performed in the order shown in Figure 3, and valgus stability tests were performed for each. The PL tendon was used as a graft in the first reconstruction, and the EDC tendon of the middle finger was used in the second reconstruction.
After the valgus stability test, the load-to-failure test was performed at 90° of flexion in the specimen using either the anchor method (group IA) or Ito method (group AI). The elbow was loaded at 1 mm/s until ultimate mechanical failure of the construct occurred. The maximal torque (N·m) and location of failure were recorded for each specimen.
Statistical Analysis
A repeated-measures 2-way analysis of variance (ANOVA) with a Bonferroni post hoc test was used to compare the displacements against a valgus load of the 4 AOL conditions (intact AOL, resected AOL, reconstruction by the anchor method, and reconstruction using the Ito method), and those of across flexion angles. An unpaired t test was used to compare the failure strength of the anchor and Ito methods. P < .05 was considered statistically significant in tests of statistical inference. All statistical analyses were performed using JMP Pro Version 17.0.0 (Statistical Discovery) and based on the opinions of statisticians.
Results
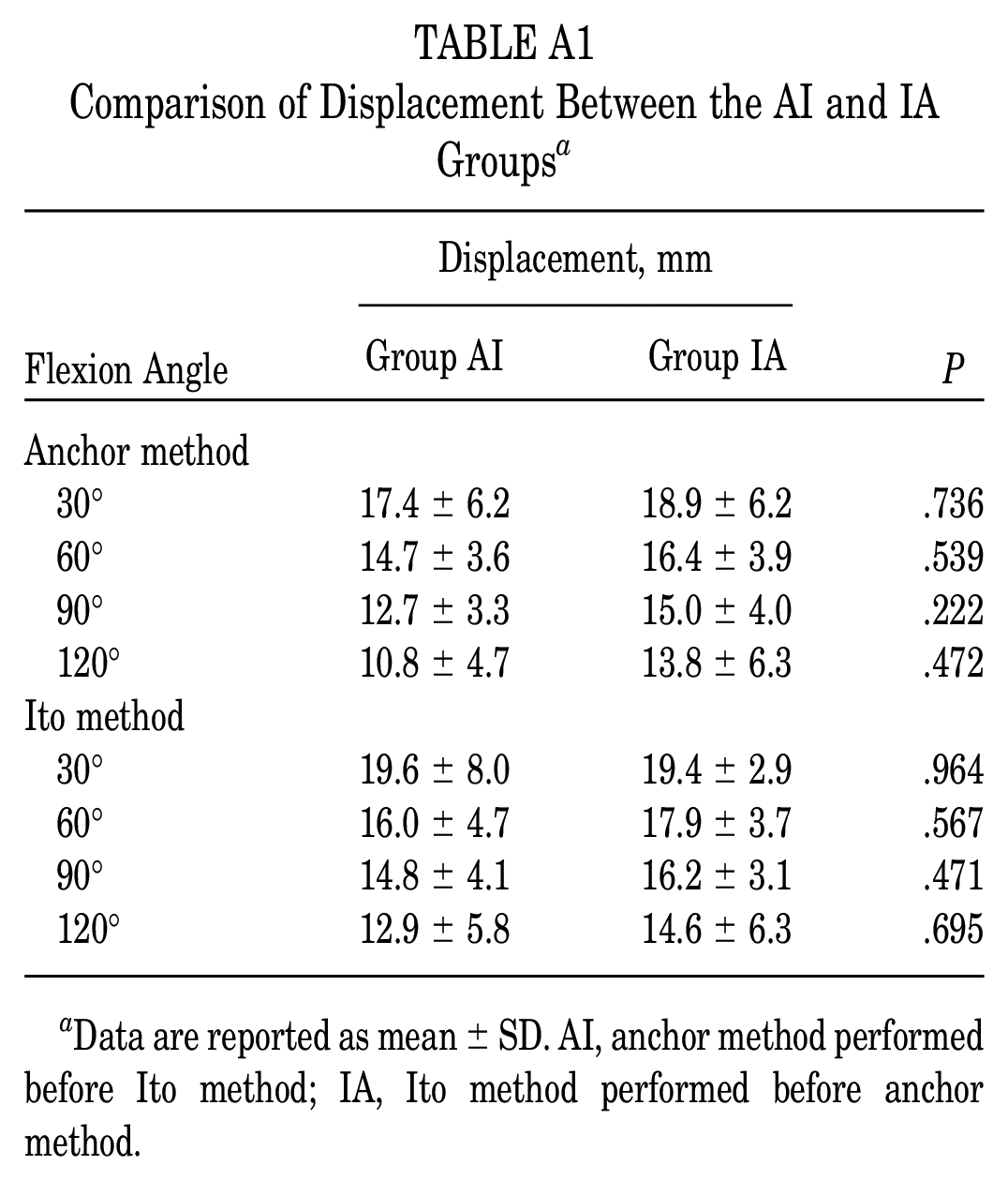
Complete datasets for the 4 AOL conditions were obtained for all 8 specimens. All 8 specimens included a PL tendon and an EDC tendon of the middle finger. The mean widths of the PL and EDC tendons were 3.58 ± 0.17 and 3.53 ± 0.25 mm (P = .668), and the mean lengths were 18.6 ± 1.8 and 19.4 ± 2.0 cm (P = .337). Comparison of displacement between the AI and IA groups indicated that there were no differences according to order that the specimens underwent reconstruction, for either the anchor or Ito methods (Appendix Table A1). Further, there was no significant difference in displacement at 90° of flexion between the first and second measurements, for either the anchor or Ito methods (Appendix Figure A1).
The mean displacement at 30°, 60°, 90°, and 120° of elbow flexion are listed in Table 1. There was a significant difference in the displacements at 60° and 90° of flexion (P < .001 for both). Post hoc testing indicated that the displacements of the intact AOL and anchor method at both 60° and 90° of flexion were significantly smaller than that of the resected AOL (P ≤ .012 for all) (Table 2). While the displacement of the Ito method was significantly smaller than that of the resected AOL at 90° of flexion (P = .002), there was no significant difference at 60° of flexion. Although the displacement at 30° was significantly larger than that at 120° for both the intact AOL and resected AOL (P < .001 for both), the difference in displacement between the anchor and Ito methods was not significant at any angle of flexion. The displacement trends for each flexion angle are shown in Figure 6.
Results of the Valgus Stability Test a

Data are reported as mean ± SD. Boldface P values indicate statistically significant difference between the 4 conditions (P < .05, repeated-measures 2-way ANOVA). ANOVA, analysis of variance; AOL, anterior oblique ligament.
Results of Post hoc Tests of Significant Differences Between Conditions a

Boldface P values indicate statistical significance (P < .05). AOL, anterior oblique ligament; CI, confidence interval; MD, mean difference.
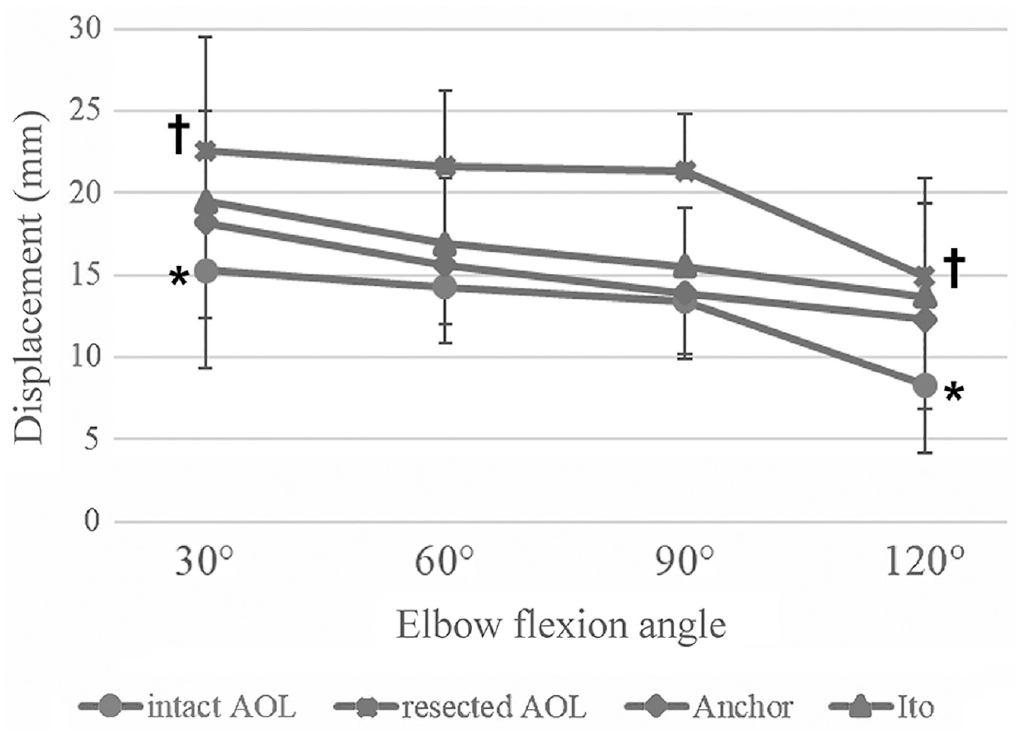
Comparison of mean displacement in valgus stability at 30°, 60°, 90°, and 120° of flexion between the 4 AOL conditions. Although the displacement at 30° was significantly larger than that at 120° for the intact AOL and resected AOL (*†P < .001 for both), there were no significant differences in displacement at any flexion angle between the anchor and Ito methods. Error bars represent standard deviation AOL, anterior oblique ligament.
There was no significant difference in the load-to-failure torque between the anchor and Ito methods (Table 3). With regard to the location of the failure, loosening of the interference screw occurred in 6 elbows (3 in each of the anchor and Ito methods), cut-out of the ulna in 1 elbow in the Ito method, and supracondylar fracture of the humerus in 1 elbow in the anchor method.
Results of Load-to-Failure Testing

Discussion
Overall, we observed no significant differences in displacement at any angle of flexion or in the failure strength between the anchor and Ito methods. As both methods were performed on the same specimens, this study has the advantage of removing individual donor biases such as differences in bone quality. On the other hand, although the displacements against a valgus load at 60° of flexion in both the anchor and Ito methods were significantly higher than that of the resected AOL, there was no significant difference in the stability at 90° of flexion between the Ito method and resected AOL. Furthermore, similar to a previous study, the change in displacement at 30° to 120° of flexion in the 4 AOL conditions was different. 31 In other words, it was most unstable at 30° and stabilized as the angle increased. In contrast, there were differences in the displacement trends between the 2 reconstructed elbows and the others (Figure 6).
Regarding the difference in the displacement of the anchor and Ito methods when compared with the resected AOL, it is possible that the Ito method caused a loss of stability when the flexion angle changed from 60° (fixed position in this study). On the other hand, there was no significant difference in the load-to-failure torque between the anchor and Ito methods. This result is especially valuable, as we used the same donor (right or left side) for both methods. In contrast, Dugas et al 12 reported the failure torque of the docking method as 21.02 N·m, and Leasure et al 25 reported that of the modified Jobe method as 20.9 N·m. Although we preserved soft tissue including flexor muscles similarly to these studies, the failure torques of the anchor and Ito methods in our study were smaller than those described previously. This may be due to differences in measurement methods and the older age of the specimens in this study.
The intact elbow was generally most lax to valgus torque at 30° of flexion, 22 and the displacement at 30° tended to be low across all 4 AOL conditions in this study. In this study, although the displacement at 30° was significantly greater than that at 120° in intact AOL and resected AOL, there was no corresponding significant difference between the anchor and Ito methods. In other words, the influence of the reconstructed AOL against valgus load was suggested to be reduced by increasing elbow extension and flexion angles, similar to a previous study. 1 This could be attributed to the fact that the anchor and Ito methods do not reconstruct the complete anatomy. The AOL is functionally composed of anterior and posterior bands, with the anterior band functioning as the primary restraint of the elbow joint from 0° to 60° of flexion, and the posterior band functioning as the primary restraint from 60° to 120° of flexion.6,27,30,33 It is therefore possible that the anchor and Ito methods may be unable to completely replicate these functions. It is important to note that, whereas UCL reconstruction is performed frequently in baseball pitchers, the elbow flexion angle during pitching differs between pitching forms: for example, approximately 90° of flexion in overhead throwing and 30° in sidearm throwing. 22 It is therefore important that the stability at each angle after reconstruction is similar to that of the intact AOL and, as such, other anatomic reconstruction methods might be preferable.
We consider the anchor method to be simpler and less invasive than techniques that use bone tunnels, as it requires minimal anterior and posterior dissection to the sublime tubercle and no procedure to pass the graft tendon through the bone tunnels of the ulna. Furthermore, the ulnar bone loss in the anchor method is less than that occurring when using the bone tunnels method, and as such, revision surgery may be easier. In this study, while ulnar cut-out was observed in 1 case, it occurred without anchor failure. As an accurate technique is required to create stronger bone tunnels, the Ito method can be difficult to perform. In contrast, the anchor method could be considered superior in this regard, as it is simpler to perform and requires less surgical skill.
Limitations
This study has several limitations that should be acknowledged. First, similar to other cadaveric studies, the mean age of the specimens in this study was 82 years, which is older than that of typical UCL reconstruction patients. Second, we evaluated only the initial displacement and failure strength against a valgus load. Third, only a single loading cycle was evaluated. As repeated cyclic loading in the elbow occurs during pitching, a repeated valgus load would more closely mimic the conditions than a single load. To reproduce the surgery, we preserved soft tissue, including flexor muscles and, to prevent damage to these soft tissues, we chose not to load on repeated valgus torque. Furthermore, although it is possible for a single load to result in measurement error, the stability of the first measurement at 90° of flexion in this study was similar to that of the second measurement. Thus, any soft tissue damage due to the valgus load and the effect of tendon stretching is most likely minimal, and the measurement error is subsequently thought to be small. Finally, while the EDC tendon was used as a graft, the width and length of the EDC tendon were similar to those of the PL tendon, and there was no significant difference in the displacement at 30° to 120° of flexion between groups AI and IA in either the anchor or Ito methods. Therefore, the effect of the difference in grafts was considered to be small.
Conclusion
The displacement against a single valgus load was comparable between the novel anchor method and the Ito method at 30°, 60°, 90°, and 120° of flexion in this cadaveric study. Furthermore, the failure strength obtained using the suture anchor method was comparable with that obtained using the bone tunnel method. UCL reconstruction using a suture anchor on the ulnar side is a simpler and less invasive method than using bone tunnels, with similar outcomes.
Footnotes
Appendix
Comparison of Displacement Between the AI and IA Groups a
| Flexion Angle | Displacement, mm | P | |
|---|---|---|---|
| Group AI | Group IA | ||
| Anchor method | |||
| 30° | 17.4 ± 6.2 | 18.9 ± 6.2 | .736 |
| 60° | 14.7 ± 3.6 | 16.4 ± 3.9 | .539 |
| 90° | 12.7 ± 3.3 | 15.0 ± 4.0 | .222 |
| 120° | 10.8 ± 4.7 | 13.8 ± 6.3 | .472 |
| Ito method | |||
| 30° | 19.6 ± 8.0 | 19.4 ± 2.9 | .964 |
| 60° | 16.0 ± 4.7 | 17.9 ± 3.7 | .567 |
| 90° | 14.8 ± 4.1 | 16.2 ± 3.1 | .471 |
| 120° | 12.9 ± 5.8 | 14.6 ± 6.3 | .695 |
Data are reported as mean ± SD. AI, anchor method performed before Ito method; IA, Ito method performed before anchor method.
Final revision submitted April 20, 2023; accepted May 4, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chiba University Graduate School of Medicine (approval No. 4234).