
Abstract
Background:
Tibial tubercle osteotomy (TTO) is a well-established surgical treatment option for patients with patellofemoral disorders.
Purpose:
To determine the rate of early (≤90 day) postoperative complications after TTO and variables related to postoperative complications.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent TTO at a single academic institution within a 15-year period (2008-2022) were identified. All patients with a minimum 90-day follow-up were considered for study inclusion. Exclusion criteria were age younger than 14 years and revision surgery. Patient characteristics, surgical history, and concomitant procedures were identified, and risk factor analysis was performed to identify variables associated with early postoperative complications.
Results:
A total of 344 knees in 313 patients met eligibility criteria and were included in the final analysis. One intraoperative complication (0.3%), a premature closure of the incision before repair of the vastus medialis, was identified. There were 141 postoperative complications (138 surgical, 3 medical) in 118 patients for a complication rate of 34.3%. The most common complications were stiffness requiring a nonstandard-of-care intervention (16.3%), superficial wound infection/wound dehiscence (8.1%), and hemarthrosis/effusion requiring aspiration (5.8%). Patients experiencing postoperative complications were older (mean difference, 3.49 years; 95% CI, 1.26-5.73 years; P = .002), had a higher mean Charlson Comorbidity Index (mean difference, 0.26; 95% CI, 0.08-0.45; P = .006), and were more likely to be current smokers (P = .015) compared with patients with no complications. Inpatient surgery (defined as surgery in a hospital setting with at least 1 overnight stay) was associated with postoperative complications (odds ratio [OR], 2.29; 95% CI, 1.39-3.77; P = .001); this association remained significant generation of a multivariate model (OR, 2.07; 95% CI, 1.19-3.58; P = .010). Previous surgery on the ipsilateral knee (P < .001) and concomitant autologous chondrocyte implantation (P = .046) were also associated with postoperative complications.
Conclusion:
The study findings indicated a low intraoperative complication rate (0.3%) and a relatively high early postoperative (≤90 day) complication rate (34.3%) after TTO. Variables associated with postoperative complications included greater age, higher Charlson Comorbidity Index, surgery in an inpatient setting, previous surgery on the ipsilateral knee, and concomitant autologous chondrocyte implantation.
Keywords
Tibial tubercle osteotomy (TTO) is a well-established surgical treatment option for patients with patellofemoral disorders such as patellofemoral instability, patellar and trochlear focal chondral lesions, and patellofemoral arthritis. 21,26 When TTO is undertaken, anterior transfer of the tibial tubercle works to mechanically offload the patellofemoral joint while medialization or lateralization works to restore patellar tracking. 10,11,19 Further, TTO is frequently combined with soft tissue stabilizing procedures, biological treatment of chondral lesions, or patellofemoral resurfacing to improve patient symptoms.
Studies investigating subjective and functional outcomes of TTO have reported excellent short- and long-term results. 2,4,8 A variety of major and minor complications of TTO have been described in the literature including superficial wound infection, stiffness, tibial fracture, nonunion, neurovascular complications, and deep infection. 14,18,22,24 Overall complication rates have varied between 0% and 59%. 14,15,17,18,22 –24 This heterogeneity is reflective of differences in surgical technique, rehabilitation, and definitions of complications. Many studies do not consider minor complications such as significant effusion requiring aspiration or knee stiffness in their analysis; however, these complications are burdensome for the patient and affect quality of life. In addition, these previous studies have been limited in their ability to characterize complications and associated variables, such as patient demographics, previous surgical intervention, and concomitant procedures.
The ability to provide surgeons with a more concrete analysis of complication rates allows for a more comprehensive discussion with patients regarding perioperative and postoperative expectations. In addition, this valuable information can aid in the identification of modifiable risk factors and risk stratification. Thus, the purpose of this study was to report on the rate of intraoperative and early postoperative (≤90 day) complications of TTO surgery and associated variables from the 15-year experience of a single academic institution. By broadening the definition of complications included in this study, it was hypothesized that a higher rate of postoperative complications after TTO surgery would be identified compared with previous literature reports.
Methods
Study Design
The study protocol received institutional review board approval. A retrospective case-series study design was used to achieve the primary objective of identifying risk factors for early (≤90 day) postoperative complications after TTO surgery. Patients experiencing at least 1 postoperative complication were identified and compared with those experiencing no complications.
Patients
We performed a query of the administrative database at a single academic institution using the Current Procedural Terminology code 27418 (TTO) to identify patients who underwent a TTO starting January 1, 2008, and with a minimum 90-day follow-up. All patients who underwent a primary TTO procedure with a minimum 90-day follow-up were considered for inclusion. Exclusion criteria were inadequate follow-up, unavailable medical records, age less than 14 years, and revision surgeries. Patients were included regardless of concomitant injuries or previous surgical procedures (except previous TTO). All patients were treated by 1 of 8 fellowship-trained sports medicine orthopaedic surgeons. The indication for all TTO procedures included 1 or more of the following: recurrent patellar instability, focal patellofemoral chondral lesions, or patellofemoral arthritis not amendable to conservative treatment with anti-inflammatories, activity modification, and therapy. The surgical approaches were not standardized for this study, and an appropriate correction was determined at the discretion of the attending surgeon.
Data Collection
The clinical and operative notes of all eligible patients were reviewed, and demographic, operative, and postoperative data were recorded. Intraoperative and early postoperative complications including stiffness, hemarthrosis/effusion requiring aspiration, hardware complications, neurovascular complications, and wound complications were assessed. Chondroplasty was considered as debridement of articular cartilage, separate from drilling or microfracture procedures. For the purposes of this study, stiffness was defined as any medical or surgical intervention for restricted range of motion including the use of corticosteroids (oral or intraarticular) or dynamic/static progressive bracing. Superficial wound infection/wound dehiscence was defined as the prescription of antibiotics in response to documented wound concerns or clear description of gross wound abnormalities. All episodes of deep infection required a return to the operating room for irrigation and debridement. Symptomatic hardware was considered as patient-reported pain at the hardware site. All medical complications (ie, deep vein thrombosis, pulmonary embolism, urinary tract infection, death) were recorded. Outpatient surgery was defined as any surgery performed in an ambulatory surgical center or any surgery performed in a hospital setting with same-day discharge. Any surgery performed in a hospital setting requiring at least 1 overnight stay was classified as inpatient. No patients operated on at an ambulatory surgical center required transfer to a hospital setting. Study data were collected and managed using REDCap (Vanderbilt University), a secure web-based software platform, hosted at the OrthoCarolina Research Institute. 12
Statistical Analysis
Descriptive statistics were calculated for all continuous and categorical variables. Continuous variables are reported as mean and standard deviation, whereas categorical variables were reported as frequencies with percentages. A Wald chi-square (χ2) test was used to analyze categorical variables and a t test was used to test the difference in means for continuous variables. A P value ≤.05 was considered statistically significant. A post hoc analysis of complications occurring in the inpatient versus outpatient setting was performed using multivariate regression modelling. All statistical analysis was performed using SAS Version 9.4 (SAS Institute). An a priori power analysis was not performed, as all eligible patients were included in the study.
Results
After inclusion and exclusion criteria were applied, 344 eligible knees in 313 patients were included in the final analysis (Figure 1). A total of 118 knees (34.3%) experienced early postoperative complications, while 226 knees (65.7%) did not. The mean age at operation was 27.2 ± 10.2 years, and 68% of patients were female.

CONSORT flowchart of patient inclusion. CONSORT, Consolidated Standards of Reporting Trials; TTO, tibial tubercle osteotomy.
Baseline Demographics
Bivariate analysis revealed association of postoperative complications with age, Charlson Comorbidity Index (CCI), and smoking status (Table 1). Patients experiencing postoperative complications were older (mean difference, 3.49 years; 95% CI], 1.26-5.73; P = .002) had a higher mean CCI (mean difference, 0.26; 95% CI, 0.08-0.45], P = .006), and were more likely to be current smokers (odds ratio [OR], 2.86; 95% CI, 1.26-6.66; P = .015). Surgery occurring in an inpatient setting was also associated with postoperative complications (OR, 2.29; 95% CI, 1.39-3.77; P = .001).
Baseline Demographics of Patients With and Without Postoperative Complications a
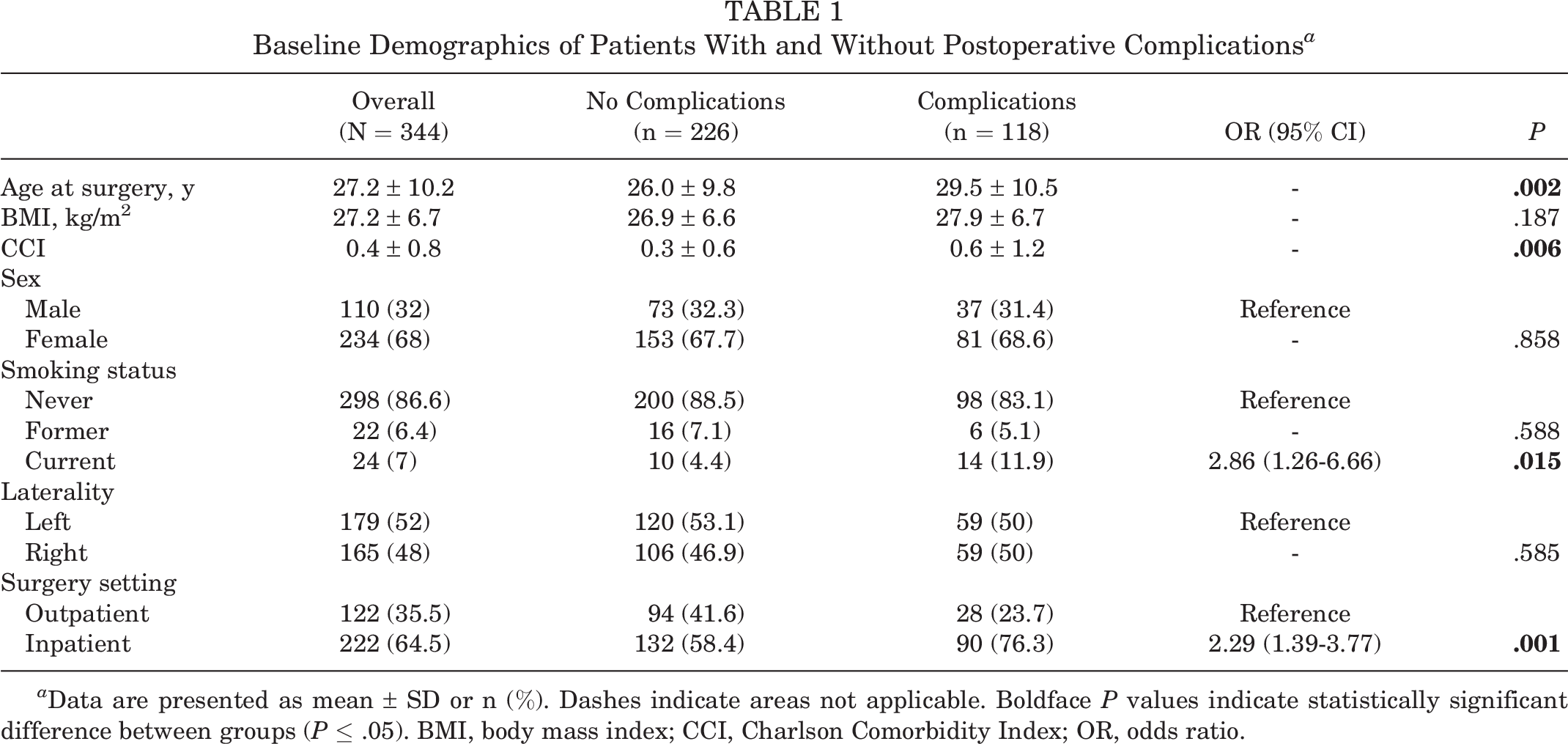
a Data are presented as mean ± SD or n (%). Dashes indicate areas not applicable. Boldface P values indicate statistically significant difference between groups (P ≤ .05). BMI, body mass index; CCI, Charlson Comorbidity Index; OR, odds ratio.
Complication Rates
There was 1 intraoperative complication (0.3%) in which there was accidental closure of the incision before reattachment of the vastus medialis to the patella. The incision was reopened and the vastus medialis repaired without further complication. There were 141 early (≤90 day) postoperative complications in 118 knees (34.3%) (Table 2). In all, 138 surgical postoperative complications occurred. There was a 16.3% rate of stiffness, an 8.1% rate of superficial wound infection/wound dehiscence, and a 5.8% rate of hemarthrosis/effusion requiring aspiration. Of the 56 patients with stiffness, 9 (2.6% of cohort) required a return to the operating room for lysis of adhesions and/or manipulation under anesthesia. Deep infections requiring irrigation and debridement occurred at a rate of 2.0%. Three medical postoperative complications occurred: a pulmonary embolism in 2 patients (0.6%), 1 of which resulted in death (0.3%).
Postoperative Complications a

a 141 complications (138 surgical, 3 medical) in 118 patients.
b Expressed as percentage of total cohort (N = 344).
Previous Surgical Interventions
Patients experiencing postoperative complications were more likely to have had previous surgical intervention of any type on the ipsilateral knee (OR, 2.43; 95% CI, 1.54-3.84; P < .001). Specifically, previous chondroplasty and/or loose body removal (OR, 2.77; 95% CI, 1.73-4.43; P < .001), lateral release with or without medial imbrication (OR, 1.94; 95% CI, 1.13-3.36; P = .017), partial meniscectomy (OR, 4.04; 95% CI, 1.19-13.7; P = .025), and synovectomy/plica excision (OR, 3.37; 95% CI, 1.36-8.39; P = .009) were all associated with postoperative complications (Table 3).
Surgical History of Patients With and Without Postoperative Complications a
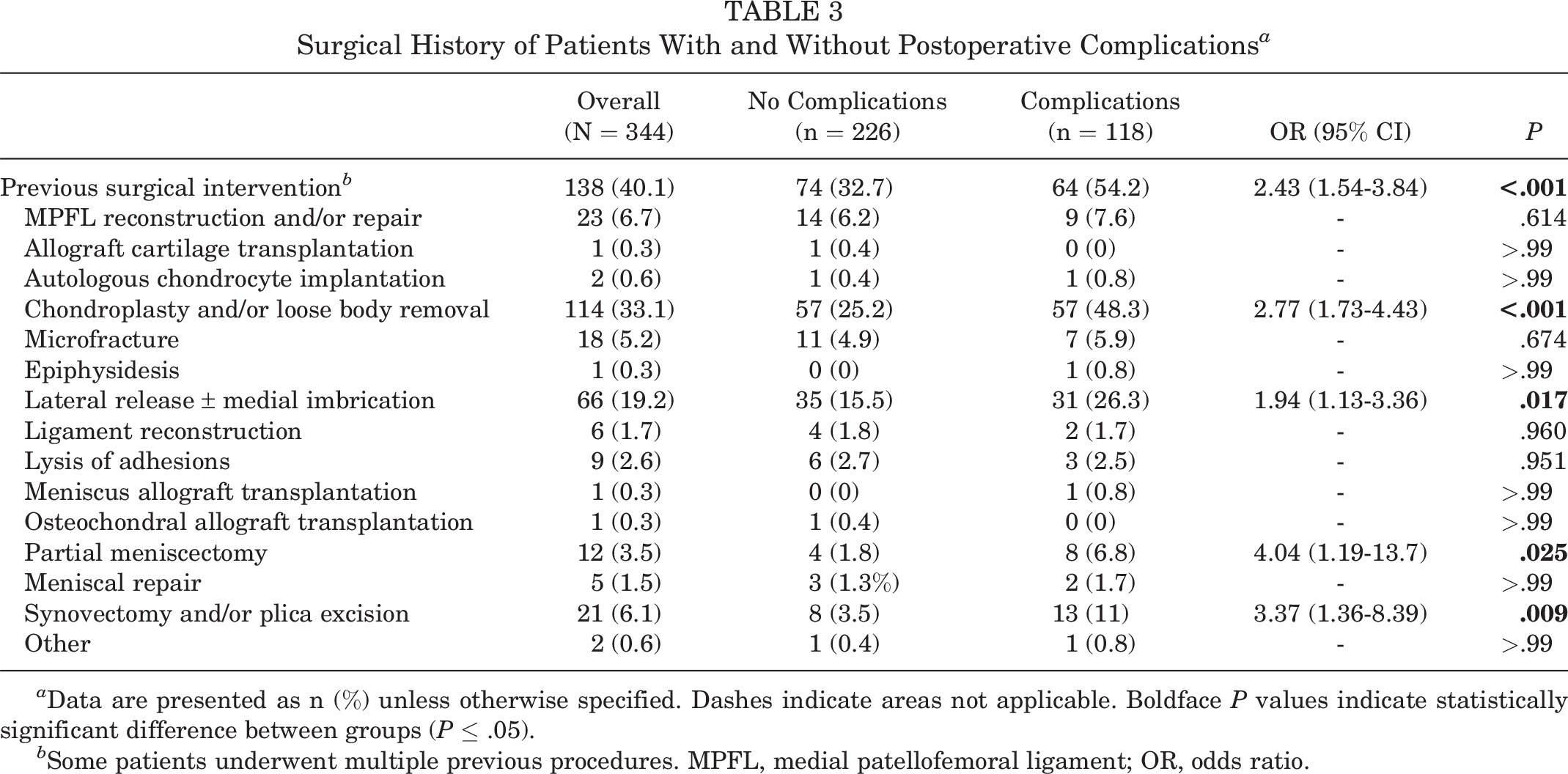
a Data are presented as n (%) unless otherwise specified. Dashes indicate areas not applicable. Boldface P values indicate statistically significant difference between groups (P ≤ .05).
b Some patients underwent multiple previous procedures. MPFL, medial patellofemoral ligament; OR, odds ratio.
Concomitant Procedures
A total of 341 patients (99.1%) underwent a concomitant procedure in addition to TTO, the most common of which was chondroplasty and/or loose body removal (65.4%), lateral release with or without medial imbrication (58.4%), and medial patellofemoral ligament (MPFL) reconstruction and/or repair (47.4%) (Table 4). The only concomitant procedure associated with postoperative complications was autologous chondrocyte implantation (ACI) (OR, 2.07; 95% CI, 1.01-4.22; P = .046). Specifically, among the 34 patients who underwent concomitant ACI, the most common complications included stiffness in 10 patients (29.4%), superficial wound infection/wound dehiscence in 4 patients (11.8%), and hemarthrosis/effusion requiring aspiration in 2 patients (5.9%).
Concomitant Procedures in Patients With and Without Postoperative Complications a

a Data are presented as n (%) unless otherwise specified. Dashes indicate areas not applicable. Boldface P values indicate statistically significant difference between groups (P ≤ .05). MPFL, medial patellofemoral ligament; OR, odds ratio.
b Some patients underwent multiple concomitant procedures.
Post hoc Inpatient Versus Outpatient Analysis
As demonstrated in Table 1, the inpatient surgery setting was found to be associated with postoperative complications. Bivariate associations between age, CCI, year of surgery, BMI, previous knee surgery, sex, and smoking status were further assessed. A multivariate model adjusting for these factors was fit and a backward elimination variable reduction approach was used to eliminate the least significant variables from the model. After generation of the final model, the association between inpatient surgery and postoperative complications remained significant (OR, 2.07; 95% CI, 1.19-3.58; P = .010).
Post hoc analysis revealed that inpatients were older (mean difference, 3.16 years; 95% CI, 0.94-5.38; P = .005), had a higher BMI (mean difference, 1.63; 95% CI, 0.14-3.12; P = .033), and a higher CCI (mean difference, 0.23; 95% CI, 0.05-0.42; P = .015) (Supplemental Table S1). Inpatients were more likely to have undergone previous surgery on the ipsilateral knee (OR, 4.02; 95% CI, 2.41-6.71; P < .001), as well as concomitant MPFL reconstruction and/or repair (OR, 2.28; 95% CI, 1.44-3.61; P < .001), concomitant allograft cartilage transplantation (OR, 8.77; 95% CI, 1.14-67.21; P = .037), and concomitant ACI (OR, 21.13; 95% CI, 2.85-156.5; P = .003) (Supplemental Table S2). Regarding type of postoperative complication, stiffness (OR, 4.65; 95% CI, 2.04-10.63; P < .001) and hemarthrosis/effusion requiring aspiration (OR, 5.29; 95% CI, 1.21-23.21; P = .027) were associated with inpatient surgery (Supplemental Table S3).
Discussion
The findings from this study of 15-year data at a single academic institution indicated that variables associated with early postoperative complications after TTO surgery include greater age at surgery, higher CCI, inpatient surgery, previous surgical intervention on the ipsilateral knee, and concomitant ACI. There was a low intraoperative complication rate (0.3%) and a relatively high early postoperative complication rate (34.3%). The most common complications included stiffness (16.3%), superficial wound infection/wound dehiscence (8.1%), and hemarthrosis/effusion requiring aspiration (5.8%).
The rates of complications of TTO surgery in the literature vary widely, with rates ranging between 0% and 59%. 14,15,17,18,22 –24 In a review of 21 TTO studies, Saltzman et al 24 reported a cumulative 79 complications among a total of 1055 knees (8% of cohort). The most common complications included recurrent patellar dislocation (1.9%), proximal tibia fractures (1.8%), and tibial tubercle fractures (1.3%). Postoperative infection and intraoperative complications occurred at rates of 0.5% and 0.2%, respectively. Of note, 15 of the 21 included studies reported a follow-up period >2 years, reflecting the longer-term focus of the studies compared with this study, which focused on complications occurring within the first 90 days of surgery. Similarly, in a review of 787 TTOs from 19 studies, Payne et al 22 reported an overall complication rate of 4.6%. In a retrospective cases series of 17 knees undergoing anteromedial tibial tubercle transfer, Klinge and Fulkerson reported symptomatic hardware necessitating removal in 10 patients (59%). 15 Similar to the findings of this study, in a series of 163 knees undergoing TTO, Lundeen et al 18 reported an overall complication rate of 29.5%.
The difference in published rates of postoperative complications is reflective of significant variability in study design. The higher rate observed in this study is likely due to a more comprehensive list of complications analyzed, including stiffness and hemarthrosis/effusion requiring aspiration. Ultimately, differentiating complications from the expected postoperative course remains difficult and subjective. Specifically, transient complications such as stiffness and hemarthrosis/effusion requiring aspiration may be seen as a mere inconvenience by surgeons, but substantially limiting by patients. The incidence and natural history of unexpected and undesirable postoperative events are important to consider as their documentation contributes to a more accurate and thorough understanding of the early postoperative course.
Rather than reporting the rates of arthrofibrosis requiring surgical intervention, we reported on the frequency of stiffness requiring a nonstandard-of-care intervention (ie, surgical intervention, oral or intraarticular corticosteroids, static progressive bracing). The overall rate of stiffness was 16.3%, while the rate of stiffness requiring a return to the operating room for lysis of adhesions and/or manipulation under anesthesia was 2.6%. Regardless of definition, restricted range of motion remains prevalent after TTO. The most common complication reported by Lundeen et al 18 was arthrofibrosis requiring surgical intervention (10.4%). In patients undergoing TTO with concomitant cartilage repair, Merkely 20 reported an arthrofibrosis rate of 22.0%. The rate reported by Schmiesing et al 25 was 8.8%. In addition to providing novel data, the approach used in this study gives patients and physicians greater insight into potential rehabilitation obstacles and allows for better counseling regarding patient expectations in the early postoperative period. Aggressive therapy and noninvasive treatment modalities were frequently effective in addressing postoperative stiffness; however, it is important to remain mindful of the cost and risk associated with nonstandard-of-care interventions.
In this study, the rate of effusion/hemarthrosis requiring aspiration was 5.8%. Effusions and hemarthrosis requiring aspiration are associated with low rates of iatrogenic infection and carry little long-term risk but do limit patient quality of life and negatively impact a patient’s ability to engage in therapy.
The documented rate of superficial wound infection/wound dehiscence in this study was 8.1%. In a cohort of 122 patients undergoing TTO, Johnson et al 14 reported a wound breakdown rate of 2.5% and an infection rate of 0%. The cumulative rate of superficial infection/wound dehiscence reported by Lundeen et al 18 was 2.4%. When considering knee osteotomy procedures more generally, superficial infection rates of 1% to 9% have been reported. 1 A lack of clear objective criteria defining superficial wound infections makes comparison between studies difficult. Cultures are rarely obtained in the postoperative clinical setting and therefore diagnosis is made on the basis of clinical manifestations (ie, drainage, erythema, edema, and warmth). To reduce subjectivity, superficial wound infection/wound dehiscence was defined as the prescription of antibiotics in response to documented wound concerns or a clear description of gross wound abnormalities. This definition is likely more liberal than most; however, even if true clinical suspicion of infection is minimal, the prophylactic prescription of antibiotics is not risk-free and should be considered carefully.
No association between sex or BMI and postoperative complications was observed; however, those experiencing complications were older (mean difference, 3.49 years; 95% CI, 1.26-5.73; P = .002), had a higher mean CCI (mean difference, 0.26; 95% CI, 0.08-0.45; P = .006), and were more likely to be current smokers (OR, 2.86; 95% CI, 1.26-6.66; P = .015). In a study published by Cotter et al 5 characterizing rates of adverse events after osteotomy procedures about the knee, among the 505 patients that underwent TTO, no patient variables were found to increase the odds of an adverse event. Specifically, similar to the findings of this study, sex and BMI were not found to be significant predictors. Conversely, the authors did not find smoking to be associated with adverse events; however, the local vasoconstrictive properties of nicotine and the resulting negative influence on outcomes after surgery are well documented. 7
Previous surgical intervention on the ipsilateral knee was associated with the occurrence of postoperative complications. Patients with complications had undergone previous surgery 54.2% of the time versus 32.7% in those without complications (P < .001). Overall, regardless of complication status, 40.1% of all patients had undergone previous surgery on the affected knee, reflecting the complexity involved in the treatment of patellofemoral pathology. Although there is a paucity of data relating the influence of previous surgical procedures to outcomes after TTO surgery, scar tissue formation, potential for previous bacterial seeding, and alteration of the bony and/or soft tissue structures of the knee in patients with previous surgery may explain the increased complication risk. Further, the association between previous surgery and complications could be reflective of a higher baseline level of knee pathology in these patients.
The only concomitant procedure associated with postoperative complications was ACI, which was performed in 14.4% of those with complications and 7.5% of those without (P = .0046). Specifically, among the 34 patients who underwent concomitant ACI, the most common complications included stiffness in 10 patients (29.4%), superficial wound infection/wound dehiscence in 4 patients (11.8%), and hemarthrosis/effusion requiring aspiration in 2 patients (5.9%). Regarding the combination of TTO and ACI, Zarkadis et al 30 reported on a series of 73 knees undergoing patellofemoral ACI, of which 66 underwent concomitant TTO. Despite a relatively high rate of return to work (78%), the complication rate was 36%, reflecting the complexity of this combination of procedures. Gillogly and Arnold 9 reported improvements in multiple patient-reported outcome scores including the International Knee Documentation Committee, Lysholm, modified Cincinnati Knee Rating System, and 12-Item Short Form Health Survey scores in patients undergoing combined ACI and TTO. Trinh et al 27 reported that outcomes of combined ACI and patellofemoral osteotomy were superior to isolated ACI in patients with patellofemoral chondral defects. Overall, these data suggest that, although patients undergoing combined TTO and ACI may experience complications at a higher rate than those undergoing isolated TTO, as the result of the correction of malalignment and offloading of chondral lesions, combined TTO and ACI remains an appropriate treatment option for patients with malalignment and full-thickness chondral lesions.
Bivariate analysis demonstrated an association between inpatient surgery and early postoperative complications (OR, 2.29; 95% CI, 1.39-3.77; P = .001), and this association remained significant after the generation of a multivariate model (OR, 2.07; 95% CI, 1.19-3.58; P = .010). Comparison of specific complications revealed higher rates of stiffness (P < .001) and hemarthrosis/effusion requiring aspiration among inpatients (P = .027). Notably, no complications including superficial wound infection/wound dehiscence (P = .428), deep infection (P = .264), or emergency room visits for pain (P = .912) were more common among the outpatient cohort. Although inpatient surgery remained an independent risk factor for postoperative complications on multivariate analysis, given the differences in baseline characteristics between inpatient and outpatient cohorts, these findings potentially reflect the preference of surgeons to perform complex surgeries on higher-risk patients in the inpatient setting. The results of this study further demonstrate that with appropriate patient selection, outpatient TTO surgery can be performed safely without increased risk of early postoperative complications.
The study findings are corroborated by a recent retrospective cohort study published by Doran et al 6 in which the authors compared complications between patients undergoing osteotomies about the knee in the inpatient versus outpatient setting. Despite potential concerns regarding neurovascular compromise, compartment syndrome, and postoperative pain control, among 531 patients (222 outpatient, 309 inpatient), the authors reported no differences in complication (P = .833), readmission (P = .503), or reoperation (P = .503) rates between the 2 groups in the 90-day postoperative period. The transition to outpatient surgery is one of several tactics being utilized to increase the value of health care while decreasing costs. Several studies have demonstrated the safety and efficiency of outpatient arthroplasty surgery with preliminary data now emerging suggesting that osteotomy surgery may also be amenable to this environment. 3,6,13,16,28,29
Limitations
This study is not without limitations. The retrospective design limits the objectivity of the reported findings and precludes high-level evidence appropriate for treatment guidelines. Further, this study did not consider or analyze the role of anatomic factors such as patella alta, trochlear dysplasia, excessive lateral patellar tilt, tibial tubercle-trochlear groove distance, and lateral femoral condyle hypoplasia. Evolution and heterogeneity in surgical practice, skill, and technology were not considered. The post hoc inpatient versus outpatient analysis is limited by selection bias, as evidenced by the differences in baseline demographics. Although a multivariate model was generated to account for potential confounding variables, it remains possible that certain relevant variables were not considered. Nonetheless, this heterogeneity reflects the importance of appropriate risk stratification when determining patient appropriateness for outpatient surgery. In addition, the variety in previous and concomitant procedures included in this study increases the external validity of the reported findings. Lastly, this study is strengthened by the overall large cohort size, and it should be noted that 341 of the 413 surgeries (82.5%) performed during the study period were included in the final analysis.
Conclusion
These 15-year data reveal that there is a low intraoperative complication rate (0.3%) and a relatively high early postoperative (≤90 day) complication rate (34.3%) after TTO surgery. Variables associated with postoperative complications include greater age, higher CCI, surgery in an inpatient setting, previous surgery on the ipsilateral knee, and concomitant ACI.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231194367#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231194367 - Early Postoperative Complications and Associated Variables After Tibial Tubercle Osteotomy: A 15-Year Experience From a Single Academic Institution
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231194367 for Early Postoperative Complications and Associated Variables After Tibial Tubercle Osteotomy: A 15-Year Experience From a Single Academic Institution by Alexander N. Berk, Kennedy K. Gachigi, David P. Trofa, Dana P. Piasecki, James E. Fleischli and Bryan M. Saltzman in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted March 31, 2023; accepted May 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.P.T. has received grant support from Arthrex and education payments from Arthrex, Peerless Surgical, and Smith & Nephew. D.P.P. has received education payments from Peerless Surgical and consulting fees from Zimmer Biomet. J.E.F. has received education payments from Peerless Surgical, nonconsulting fees from Smith & Nephew, and hospitality payments from Arthrex. B.M.S. has received grant support from Arthrex; education payments from Arthrex, Peerless Surgical, and Smith & Nephew; consulting fees from Bioventus; and royalties from Nova Science Publishers. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Wake Forest University (No. IRB00086639).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.