
Abstract
Purpose
Tibial tubercle osteotomies (TTOs) are a seemingly straightforward technique; however problems with bony union, implant failure, wound infections, and fractures have been reported in the literature.
Methods
A database search identified all patients who had a TTO performed for patellofemoral instability between 1 March 2000 and 30 July 2008 by a single surgeon. The TTO technique was modified twice during the study period (December 2003 and June 2007, respectively), thereby creating three similar patient cohorts.
Results
TTOs were performed in 101 knees (90 patients), in which 34 knees (29 patients) received the blunt technique (TTO-B), 32 knees (30 patients) the sloped technique (TTO-S), and 35 knees (31 patients) the greenstick technique (TTO-G). Mean age of the patients (75 females, 15 males) was 16.0 years (range 12.2–20.2 years). Overall, six patients had complications, namely, six tibia fractures and no nonunions, for an overall complication rate of 5.9%. In the TTO-B group, four patients had four tibia fractures for an overall bony complication rate of 11.8%. In the TTO-S group, two patients had two delayed unions which developed into tibia fractures for an overall bony complication rate of 6.2%. There were no complications (0%) in the TTO-G group. No correlation was identified between TTO screw size and complications. The caudal aspect of the osteotomy was the location of the tibia fracture in five knees and the caudal screw in 1 knee, at a mean of 11 weeks postoperatively. All fractures were treated only with splint or cast immobilization and protected weight-bearing.
Conclusion
The overall bony complication rate was 5.9% for the TTOs in this study. Utilizing the TTO-G technique with rigid two-screw, bicortical fixation the complication rate could be lowered to 0%. Avoidance of periosteal stripping, and secondary cortical devascularization at the caudal aspect of the TTO appears to optimize bony consolidation, thereby minimizing fractures.
Clinical relevance
Bony complications are an infrequent problem after TTO. Greensticking the distal end of the TTO can minimize postoperative tibia fractures. Running and sports should not be permitted until complete cortical healing is documented on the lateral radiograph.
Introduction
The treatment of patellofemoral pathology has been, and continues to be, challenging. Nonsurgical management is typically the initial treatment, with surgical management indicated for specific pathologies (i.e., intra-articular loose bodies) and for selected patients whose nonsurgical treatment fails to adequately manage the patient's symptoms. Numerous surgical procedures have been reported and advocated over the years for the wide spectrum of patellofemoral problems.
Most of the surgical procedures currently used for patellofemoral instability (i.e., dislocations and subluxations) and patellofemoral pain can be classified as either proximal (proximal to the distal pole of the patella) or distal procedures, and they may be performed in an isolated or combined fashion [1–7]. The distal procedure is designed to alter the force vector at the patellofemoral articulation by moving the medial patellar tendon (i.e., tibial tubercle osteotomy or Roux–Goldthwait procedure) or creating an additional medial ligamentous tether (i.e., semitendinosus and/or gracilis tendon transfer). Of the distal procedures, the tibial tubercle osteotomy (TTO) is the workhorse technique for skeletally mature patients. This osteotomy can be performed in the coronal plane (i.e., Elmslie–Trillat procedure) or sagittal plane (i.e., Maquet-style anteriorizing osteotomy), or it can be biplanar (i.e., Fulkerson procedure), depending on the patient's pathology and the surgical goals. Over time, a variety of TTO techniques (e.g., method of osteotomy creation, determination of osteotomy alignment, and osteotomy fixation) have been described with published ratings of excellent and good outcomes ranging from 66 to 96% [1, 4, 6–12].
Complications of TTOs are uncommon and can be broadly classified into four groups: wound problems (dehiscence or infection), implant prominence and/or pain, problems with bony union of the osteotomy (i.e., delayed union or nonunion), and postoperative fracture (tibial tubercle fragment or tibial shaft). The frequency of re-operation after TTO for inadequate healing ranges from 0 to 6.6% [2, 6, 9] and up to 3.3% frequency of tibial fractures [4, 18]. The lead author's experience in preforming TTOs has led to technique alterations in attempts to minimize complications. The aim of the study reported here was to report on the bony complications of TTO performed for patellar instability utilizing three different osteotomy configurations in the adolescent patient population.
Materials and methods
A surgical database search identified all patients who had a TTO performed for patellofemoral instability between 1 March 2000 and 31 July 2008 by a single surgeon at one of our two tertiary-care children's hospitals. Minimum follow-up was 6 months postoperative, no patients were lost to follow-up, and outpatient clinic notes and radiographs in each patient's medical record were reviewed. No patients during the study period who underwent a TTO were excluded from the study. All patients had closed proximal tibial physes. In knees with patellar dislocations (recurrent a/o loose bodies), TTOs are typically combined with proximal soft-tissue procedures, mainly open lateral retinacular release and medial retinacular imbrications. Knees with symptoms attributable to patellar subluxation (i.e., patellar “popping” with pain, no history of patellar dislocation, etc.) are typically treated with an arthroscopic lateral retinacular release and open tibial tubercle osteotomy. The third diagnosis in which TTOs are utilized is in the knee with anterior knee pain [13]. In this group, the primary surgical management, after failure of nonoperative treatments, is typically an arthroscopic lateral retinacular release. A small subset of these patients fails to achieve an adequate clinical response to the lateral release, and in this very selective group an open tibial tubercle osteotomy (Maquet or Fulkerson-style) may be an option.
During the study period the TTO technique was modified based on the identification of bony complications at the osteotomy site and proximal tibia. The technique was altered in December 2003 and June 2007, respectively, and this fortuitously created three comparable patient cohorts in terms of patellofemoral pathology. The only aspects of this technique that were changed during the study period were the caudal end of the osteotomy and the screw sites. Otherwise, the surgical technique and decision-making process into the use of the tibial tubercle osteotomies did not change (and remain unchanged up to the present). All of the TTOs were performed under direct vision utilizing a water-cooled saw blade while protecting the soft tissues. The use of a saw permits the creation of a smooth surface osteotomy which, when fixation is placed, enables direct opposition of the osteotomy surfaces. The use of an osteotome for the TTO creates an uneven osteotomy which can leave gaps and poor opposition when fixation is placed. Only the distal aspect of the TTO was modified during the study period. In the early group of patients (March 2000 to December 2003), the distal cut of the osteotomy was made using a saw blade in the transverse plane, at a 90° angle to the anterior tibial cortex after subperiosteal stripping of the osteotomy site (TTO-B). In the middle group of patients (December 2003 to June 2007), the osteotomy site was subperiosteally stripped, but the osteotomy was gradually tapered or sloped to exit the anterior tibia at a less than a 45° angle (TTO-S) (see Fig.2). In the late group (post-June 2007), the oscillating saw was utilized for the proximal aspect of the osteotomy (with subperiosteal dissection), but distally the osteotomy was completed with an osteotome (without subperiosteal dissection) and without exiting the tibial cortex anteriorly, but by greensticking the anterior tibial cortex (TTO-G). Osteotomized tibial tubercles were then shifted medially (±anteriorly) from 9 to 14 mm, depending on the pathology, to achieve a Q-angle of between 5 and 10°. Two bicortical screws were placed in a lag fashion across the osteotomy spaced between 25 and 30 mm apart to stabilize the osteotomy. See Fig. 1 for an illustration demonstrating each of the three types of osteotomies.
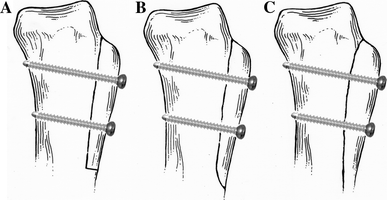
Three types of tibial tubercle osteotomies (TTO) performed during the study period (1 March 2000 to 30 July 2008) by a single surgeon. Osteotomy types:

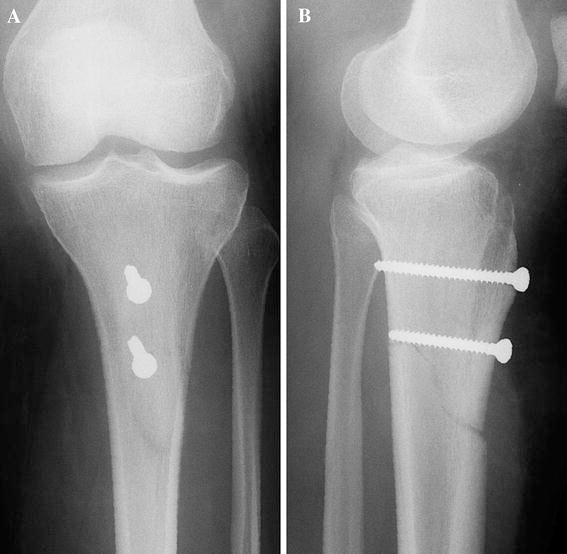
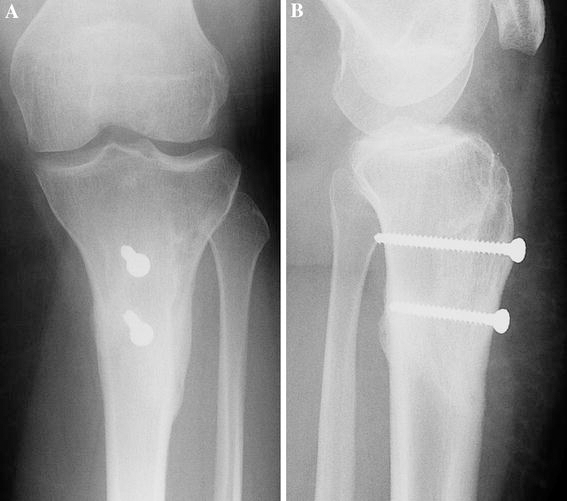
Seventeen-year-old female with left knee chronic patellar dislocations. Intra-operative lateral radiograph demonstrating TTO-S and fixation
The anteroposterior inclination of the osteotomies varied depending on the preoperative symptoms and the status of the patellofemoral articular cartilage. The majority of patients underwent arthroscopy at the time of TTO. Arthroscopy was performed immediately prior to the open patellar realignment for patellar dislocations and at the time the arthroscopic lateral release was performed. Arthroscopy at these times enabled precise assessment of the articular cartilage of the patella and femoral trochlea and the identification of pathology that could not be visualized by open arthrotomy (i.e., tibiofemoral articular cartilage pathology, meniscal tear, etc.) [5]. A more coronal plane osteotomy is utilized to maximize the correction of the coronal plane malalignment (i.e., quadriceps or Q-angle). However, the presence of significant changes to either the patellar or femoral trochlea articular surfaces will alter the inclination of the osteotomy to a more oblique osteotomy that medializes and slightly anteriorizes the fragment [5]. Regardless of osteotomy inclination, all fragments were ≥10 mm in anteroposterior thickness for the proximal 6 cm of the osteotomy. There was no difference between the three groups in the ability to attain the desired amount of surgical correction. Two screws, placed in a bicortical fashion, were utilized to permit interfragmentary compression across the osteotomy. Different screw sizes were utilized during the study period, and the possible association of screw size to complications was analyzed. A drain was placed over the osteotomy site to minimize the chance of the patient developing a postoperative wound hematoma. All drains were removed the morning after surgery.
Following surgery, the operative limbs were placed in a knee immobilizer or hinged knee brace (locked in full extension). Weight-bearing was limited to toe touch for 6 weeks postoperatively to minimize the risk of fixation failure, tubercle, or tibia fracture. Knee range of motion exercises and gentle physiotherapy were initiated after the first postoperative outpatient evaluation at 7–10 days postoperatively. At 6 weeks, radiographs typically demonstrated early union (obscuration of osteotomy), permitting the gradual return to full weight-bearing on the operative limb, and physiotherapy was increased. At the 3-month evaluation, light jogging was initiated with progression to running. Patients are typically allowed to participate in sporting activities at 4.5 months postoperatively, provided there is adequate radiographic evidence of TTO healing, knee range of motion, and near-normalization of leg strength. The postoperative protocol did not change during the study time period.
The database search identified 90 patients (75 females, 15 males) with 101 knees that satisfied the criteria for inclusion (Table 1). The mean age of the study cohort was 16.0 years (range 12.2–20.2 years) There were 53 left knees and 48 right knees, and staged bilateral knee surgeries involving TTOs were performed in 11 patients. The median length of the symptoms was 24.0 months (range 2–138 months). Twenty-five knees had undergone previous surgeries. There were 34 knees in the TTO-B group, 32 in the TTO-S group, and 35 in the TTO-G group. Diagnoses at the time of surgery were: patellar dislocations in 77 knees, patellar subluxations in 14 knees, and patellofemoral pain in ten knees.
Comparison between procedures (n = 101)
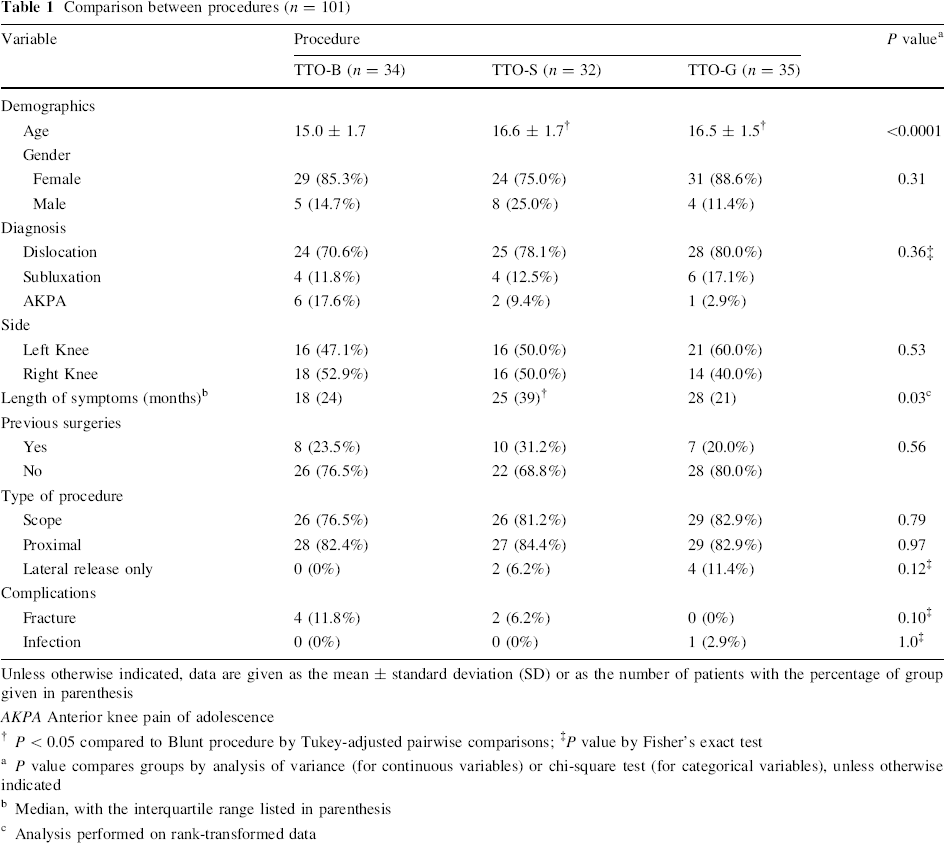
Unless otherwise indicated, data are given as the mean ± standard deviation (SD) or as the number of patients with the percentage of group given in parenthesis
AKPA Anterior knee pain of adolescence
P < 0.05 compared to Blunt procedure by Tukey-adjusted pairwise comparisons;
P value by Fisher's exact test
P value compares groups by analysis of variance (for continuous variables) or chi-square test (for categorical variables), unless otherwise indicated
Median, with the interquartile range listed in parenthesis
Analysis performed on rank-transformed data
Between-group comparisons of continuous variables were performed using analysis of variance (ANOVA). When the overall ANOVA model was significant (P < 0.05), Tukey-adjusted P values are reported for pairwise comparisons that are significant. In general, chi-square tests were used for between-group comparisons of categorical variables. However, when cell sample sizes in the contingency table were small, Fisher's exact test was used instead. Due to the lack of normality of the data distribution for the length of symptoms, these data were rank-transformed prior to analysis. The data analysis was generated using SAS software, ver. 9.1.3 of the SAS System for Linux (SAS Institute., Cary, NCA).
Results
At the time of TTO, other concomitant techniques were performed in 90 knees. Diagnostic knee arthroscopy was performed in 81 knees (80.0%): in 26 knees of the TTO-B group (76.5%), 26 knees of the TTO-S group (81.2%), and 29 knees of the TTO-G group (82.9%) (Table 1). Arthroscopic patellar shaving chondroplasty was performed in 17 knees (16.8%): in three knees of the TTO-B group (8.8%), five knees of the TTO-S (15.6%) group, and nine knees of the TTO-G (25.6%) group. Nine knees (8.9%) underwent the removal of loose bodies [TTO-B, 2 knees (5.9%); TTO-S, 2 knees (6.2%); TTO-G, 5 knees (14.3%)]. Proximal realignment (medial retinacular imbrications and open lateral retinacular release) was also performed in 84 knees, and arthroscopic lateral release was performed in six knees. Overall, six patients had complications: six tibia fractures, and no nonunions, for an overall bony complication rate of 5.9%. There were no wound hematomas.
Postoperatively, in the TTO-B group there were four proximal tibial metaphyseal fractures and no nonunions or delayed unions, for a bony complication rate of 11.8%. The fractures in this group all initiated at the anterior tibial cortex, specifically the distal transverse osteotomy, and propagated posteriorly to the posterior tibial cortex. In the TTO-S group, there were two delayed unions which progressed to tibia fractures, for a bony complication rate were 6.3%. One of the fractures started at the distal osteotomy and the other at the distal screw. In the TTO-G group, there was one deep implant infection but no tibial fractures, delayed unions, or nonunions, for a bony complication rate of 0%.
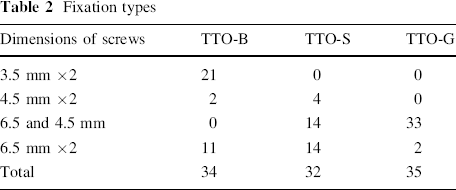
All constructs utilized two AO screws placed in a lag fashion with bicortical purchase. The breakdown of fixation type is detailed in Table 2. There were four fractures in the TTO-B group, and fixation in those cases were 2- 3.5-mm screws in one knee, 2- to 4.5-mm screws in one knee, and 2- to 6.5-mm screws in two knees. In the two TTO-S fractures, the fixation was 2- to 4.5-mm screws in one knee and 2- to 6.5-mm screws in the other knee. Statistical analysis of the association of the screws to fractures is challenging due to the four fixation screw types and small sample size (see Table 2). No correlation could be identified between TTO screw size and complications. There were no fixation failures in any patient (i.e., screw breakage, fracture of the TTO fragment, or screw pull-out).
Fixation types
The distal aspect of the osteotomy was the location of the tibia fracture in five knees (at the anterior tibial cortex) and the distal screw in one knee, at a mean of 11 weeks (8–14 weeks) postoperatively, see Figs. 3 and 4. Fractures occurred during walking activities in five patients and running in one patient. All six fractures (4 in TTO-B group and 2 in TTO-S group) had sagittal or coronal angulations <5° and were treated nonsurgically with a splint or cast immobilization with uneventful bony union. Based on radiographic findings, there were two suspected delayed unions in the TTO-S group. Both of these patients returned to the operating room and the knees underwent bone grafting and revision of fixation (3 and 7 months postoperatively, respectively). Interestingly, at the time of surgery, both osteotomies demonstrated bridging cortical union, so the osteotomy fixation was exchanged and supplementary bone grafting were performed in both knees.
Anteroposterior (
Anteroposterior (
Both TTOs healed following surgery. There was one deep implant infection in the TTO-G group. Revision surgery was performed in three knees (2 TTO revisions for delayed unions and 1 infected screw removal). Overall, nine knees (9%) underwent screw removal (8 for painful a/o prominent implants and 1 for infection).
Discussion
Tibial tubercle osteotomies are important surgical techniques in the operative management of patellar instability. Overall the surgical approach is relatively straightforward, and the osteotomy a low-risk technique. Despite this, postoperative complications of wound infection and dehiscence, osteotomy nonunion/delayed union, implant prominence, implant failure, and fracture (tibial tubercle or tibial shaft) have been documented [4, 6, 9, 14–20]. Bony complication rates (nonunion/delayed union and tibial shaft/tubercle fragment fractures) have been reported in up to 3.3% of patients [19].
Healing at the osteotomy site can be affected by host factors (i.e., patient age, concomitant medical problems, and previous surgery) and surgical issues (i.e., osteotomy depth, fixation type, and postoperative rehabilitation). Delayed union of the osteotomy is not uncommon, but osteotomy nonunion is rare and has only been reported in adults [14, 17]. The frequency of re-operations after TTOs for inadequate healing ranges from 0 to 6.6% [2, 6, 9]. In this study, there were two delayed unions that underwent revision surgery in the TTO-S group. In both of these surgeries, exploration of the osteotomy site revealed bridging cortical bone medially and laterally at the osteotomy site. The indication for these repeat operations was slow, incomplete osteotomy healing on a lateral radiograph of the proximal tibia. Because of the findings at surgical revision, we do not recommend surgery based solely on radiographic lucency at the site of the osteotomy. In adolescents, revision should be considered for clinical symptoms (pain), implant failure (screw fracture or loosening), or definite evidence of osteotomy nonunion at 6 months postoperatively. If there is evidence of slow healing radiographically, activity limitation is recommended until solid union is demonstrated.
The technique of TTO reported in this study was uniform, except for the caudal end of the osteotomy. A water-cooled sagittal saw was utilized for the creation the osteotomy. After translation of the osteotomy, the smooth osteotomy surface permitted complete bony apposition along the entire extent of the osteotomy by rigid two-screw compression fixation. In addition, the typical thickness of the osteotomized tibial tubercle was approximately 9–1.2 cm, which assured that the osteotomy extended into the metaphyseal cancellous bone. The frequency of iatrogenic tibial tubercle fracture reported in the literature is up to 6.6% of knees, but no such fracture occurred in our study, likely due to the thicker TTO fragment and the fact that the fragment was nearly tricortical in cross section [2, 6, 21]. These factors likely contributed to the fairly consistent bony healing across the proximal 3–4 cm of the osteotomy in this study. The consistently problematic area in the TTO-B and TTO-S groups was at the distal aspect of the TTO, with delayed resolution of the anterior tibial cortex osteotomy defect. In the first two osteotomy techniques, the periosteum was stripped off of the anterior tibia at the level of the osteotomy. The third osteotomy technique does not strip the periosteum, rather, it leaves it intact distally, and the osteotomy does not violate the anterior tibial cortex. Koeter et al. [4] describes the difference between the TTO-B vs. TTO-S in great detail, both technically and diagrammatically. Although no data were reported on tibial fractures in their study, the authors did comment that they always performed a TTO-S for their patients and avoided the TTO-B because of their concern that a distal transverse osteotomy in the tibial “can create a stress riser”.
There have been a wide variety of fixation methods reported for TTOs: staples, one versus two versus three screws, unicortical versus bicortical fixation, and implant size/diameter [1, 4, 6, 7, 9–12, 15, 16, 20, 22, 23]. During the time period covered by our study, there was a gradual shift in implant use from two small fragment screws (2× 3.5 mm) to large fragment screws (2× 6.5 mm) to the present-day two-screw method (1× 6.5 mm and 1× 4.5 mm). As demonstrated in Table 2, the most common technique currently being used is that involving a 4.5-mm fully-threaded cancellous screw placed in a lag fashion distally and a partially-threaded 6.5-mm screw placed proximally. The more prominent of the two screws is usually the distal 4.5-mm screw; hence, to minimize prominence, the use of the countersink is necessary to sink the screw head as deep as possible. Data analysis failed to find any association between fixation and complications. Late postoperative screw removal has been reported to be as high as 48% of patients [4, 6]; in comparison, only 8.9% of knees (9 removals in 101 knees) in our study required screw removal. There were no complications associated with screw removal.
In our study, tibial shaft fractures occurred in 5.9% of knees (6 fractures in 101 knees). This complication has been reported for TTOs performed for patellofemoral pathology and for total knee arthroplasty revision [4, 14–16, 18–20]. Stetson et al. have published the largest series of postoperative fractures after tibial tubercle osteotomy [19], reporting 2.6% of knees (6/234 knees) with a proximal tibia fracture, all within 13 weeks of surgery. All fractures occurred after a change of weight-bearing status from partial to full weight-bearing. Five of the six fractures healed with nonsurgical management, and all healed with less than 5° of angulation. In the six tibial fractures, two fractures started near the screw fixation, two at the proximal osteotomy, and two at the distal osteotomy.
The distal aspect of the TTO appears to be an important factor in the risk of a tibial shaft fracture. Bellemans et al. reported on four proximal tibial fractures in 53 Fulkerson osteotomies (7.5%), all of which occurred 4–7 weeks after surgery [15]. Radiographic analysis in this study demonstrated that all fractures occurred at the proximal tibia at the level corresponding with the distal end of the osteotomy. In the description of their osteotomy technique, the authors state that no “formal osteotomy of this distal connection” was performed and the “tibial tubercle always remained attached to the tibia through this distal base”. However, the figure published in this report appears to be a TTO-B. Additionally, the literature reports a 2.6% (2/60 knees) to 3.3% (6/234 knees) frequency of tibial fractures in the TTO-S [4, 19]. Of the five studies published which used the TTO-G configuration, no tibial shaft fractures were reported out of 286 knees [1, 6, 9, 21, 22].
Based on the findings of our study and those of previously published reports, recommendations can be made to minimize the occurrence of bony complications after TTO. In this study, the differences between the groups did not reach statistical significance (P = 0.1), and analysis of the study sample demonstrated that 130 patients would be needed with the same distribution and fracture occurrence to reach the statistically significant P < 0.5 level. It is up to the clinician to make the assessment if the difference between the groups is clinically significant (11.8 vs. 6.2 vs. 0%). In the authors’ opinion, the data are sufficiently compelling to recommend the TTO-G technique over the TTO-B and TTO-B techniques. The osteotomy technique should aim to create an osteotomy which enters into the cancellous bone, thereby avoiding an osteotomy which is completely intracortical, in order to optimize bony union and minimize the chance of tibial tubercle fragment fracture. Distally, the osteotomy should not exit the anterior tibial cortex; instead, an osteotome should be used to come close (1 cm) to but not violate the anterior cortex [18]. The osteotomy is then manually translated medially by greensticking the distal connection, and then fixation is placed to maintain the corrected position. The postoperative weight-bearing on the operative limb should be limited (nonweight-bearing or toe-touch), and physiotherapy should be conservative, focusing on regaining range of motion during the first 6 weeks [15, 18, 19]. Transition to higher level activities should be permitted only after complete bony union has been demonstrated radiographically [15, 17, 19].
Conclusion
In this study, the overall bony complication rate was 8.9% for TTOs. Utilizing the TTO-G technique with rigid two-screw, bicortical fixation, the bony complication rate were lowered to 0%. Incomplete, greenstick-style distal osteotomy and the avoidance of periosteal stripping appears to optimize bony consolidation, thereby minimizing postoperative fractures.