
Abstract
Background:
There exist multiple radiographic measurements to assess patellar instability and maltracking. While originally described as a measurement predictive of patellar instability, patellar tendon–lateral trochlear ridge distance (PT-LTR) has not yet been explored as an indicative measurement of patellar maltracking in the setting of instability.
Purpose:
To assess PT-LTR in patients with instability with and without concomitant malalignment to determine whether PT-LTR may be a significant measurement in patients who exhibit patellar maltracking in addition to patellar instability, as well as to explore the relationship between patellar height and tibial tubercle–trochlear groove distance (TT-TG) to PT-LTR.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Three groups were studied, with 30 patients included in each group: (1) patients with an anterior cruciate ligament (ACL) tear without a history of patellar instability who underwent ACL reconstruction (ACLR) (control group or ACLR group), (2) patients who underwent isolated medial patellofemoral ligament reconstruction (MPFLR) for patellofemoral instability (MPFLR group), and (3) patients who underwent combined MPFLR and tibial tubercle transfer (TTT) for patellofemoral instability (MPFLR+TTT group). Intraclass correlation coefficients (ICCs) were generated to determine level of agreement in PT-LTR measurement between raters. Appropriate statistical tests were utilized for analysis.
Results:
The ICC was 0.93 for the cohort. The groups differed significantly by incidence of patella alta (Caton-Deschamps Index >1.2), in all TT-TG groupings, patella alta with TT-TG >15 mm, and patella alta with TT-TG >20 mm. The mean PT-LTR differed significantly between groups (P < .0001). Measurements for the ACLR, isolated MPFLR, and MPFLR+TTT groups were 1.15 ± 3.71 mm, 6.60 ± 6.58 mm, 12.72 ± 8.43 mm, respectively. When comparing all patients, those with patella alta, an elevated TT-TG, and a combination of both had higher PT-LTR than patients without patella alta or elevated TT-TG.
Conclusion:
The mean PT-LTR was significantly higher in patients who underwent MPFLR+TTT compared with that in ACLR controls and patients who underwent isolated MPFLR. This may reflect its role as a measurement of patellar maltracking in the setting of patellar instability. PT-LTR may be a useful tool in predicting which patients with instability may benefit from a concomitant bony realignment procedure in addition to a soft tissue stabilization procedure.
Patellar instability is a challenging clinical entity characterized by the pathological movement of the patella within and outside the trochlear groove of the femur. The reported incidence has increased, and the treatment has evolved over the past 20 years, with an overall incidence of 23.2 per 100,000 person-years for the general population. 14 Both first-time and recurrent instability can cause pain, loss of function, and long-term osteochondral damage.4,10-12 Several procedures have been used to address patellar instability, including medial patellofemoral ligament (MPFL) reconstruction (MPFLR), tibial tubercle transfer (TTT), distal femoral osteotomy, and trochleoplasty, among others, depending on the combination of contributing anatomic risk factors at play. There is limited consensus, however, on the parameters that guide surgical decision-making and the reliability of the parameters themselves.2,3
The complexity of patellar instability can be attributed to the interplay between dynamic and static stabilizers of the patellofemoral joint. 9 Any magnitude lateral force vector manifested by an excessively lateral tibial tubercle must be counteracted by soft tissue (MPFL) or bony (patellar-trochlear interaction) restraints. 7 As such, cited anatomic risk factors for first-time and recurrent patellar instability include trochlear dysplasia, patella alta, increased tibial tubercle–trochlear groove distance (TT-TG), patellar tilt, femoral anteversion, external tibial torsion, and ligamentous laxity.1,5,6,16 The TT-TG is one measurement that may indicate a combination of abnormal anatomic findings such as through knee rotation, lateralized tubercle, and/or a medialized trochlear groove in the setting of dysplasia. Abnormalities in patellar height, axial plane alignment or trochlear dysplasia may be addressed by distalizing TTT, medializing TTT, femoral rotational osteotomy or varus osteotomy, and trochleoplasty, but it is not clear whether pathological biomechanical forces are equilibrated by these interventions. Additionally, for procedures such as a medialization (with or without anteriorization) of the tibial tubercle, there is active discussion of whether the patella is medialized—and thus better constrained in the trochlear groove—by the procedure or if the medialization of the tibial tubercle manifests external rotation of the tibia. 8 Overall, it is essential to consider the vectors at play and recognize that there is a subset of patients with patellar instability who also exhibit maltracking from the presence of the aforementioned anatomic risk factors that contribute to their instability.
Mistovich et al 9 proposed a series of novel measurements, including the axial width of the patellar tendon–lateral trochlear ridge distance (PT-LTR) as a static quantification of the relationship between the extensor mechanism and its restraints. These measurements were shown to be reliable, predictable, and discriminative for patients with patellofemoral instability versus those without.
Currently, one of the most relevant questions in the world of patellofemoral instability is which patients can be successfully treated and stabilized with MPFLR alone versus which patients need to have a bony realignment concomitantly with an MPFLR to stabilize them. Thus, we sought to further confirm the interrater reliability of the PT-LTR measurement and to understand the capacity of PT-LTR to discriminate between the clinical diagnosis and treatment of patellar instability, patellar malalignment, and a control group of anterior cruciate ligament (ACL) rupture. The purpose of this study was to assess PT-LTR in patients with patellar instability both with and without concomitant malalignment. We hypothesized that PT-LTR would be higher in patients with malalignment who had undergone TTT, and therefore it may be a useful measurement in patients who have patellar malalignment and maltracking in addition to their instability. We also sought to explore the relationship between PT-TLR, patellar height, and TT-TG.
Methods
Eligibility Criteria
This was a retrospective case-control cohort study. After obtaining approval from the institutional review board (2022-1876), a retrospective chart and imaging review was performed for patients who underwent procedures performed by a single surgeon (B.E.S.S.) from January 1, 2018, through February 1, 2023. Three groups of patients were identified based on their combination of preoperative diagnosis and corresponding indicated procedure. Group 1 consisted of those who underwent ACL reconstruction (ACLR) to address an ACL tear, but without a history of patellar instability, which served as the control group (ACLR group). Group 2 consisted of those who underwent isolated MPFLR to address patellar instability (MPFLR group). Group 3 consisted of those who underwent combined MPFLR and TTT (MPFLR+TTT) to address combined patellar instability and patellar maltracking (MPFLR+TTT group). Patients who underwent ACLR were selected as the control group because they did not have patellar instability or maltracking and had magnetic resonance imaging (MRI) studies available for measurement. The patients in the MPFLR+TTT group were taken from a group of patients who were excluded from a prospective clinical study for the treatment of patellar instability with isolated MPFL and met at least 1 of 4 exclusion criteria: failed previous surgery for patellar instability, retropatellar pain from lateral patella overload syndrome >50% of their chief complaint, a jumping J sign on physical examination, and/or an unloadable inferior/lateral cartilage defect. After power analysis was performed, 30 patients from each diagnosis/treatment group were randomly selected using computer-generated randomization for inclusion, and their MRI studies were obtained. Measurement of PT-LTR, as described by Mistovich et al, 9 was performed by 5 individual raters (3 board-certified sports medicine orthopaedic surgeons (B.E.S.S., E.R.D.) and 2 orthopaedic surgery residents (B.M.A., R.D.)). Each rater evaluated all images individually and performed one measurement per patient per rater. The Caton-Deschamps Index (CDI) and TT-TG were also measured. The primary outcome investigated was the PT-LTR value with respect to the patient groups that reflected control patients, patients with patellar instability, and patients with patellar instability and malalignment. Secondary outcomes included the interrater reliability of the PT-LTR measurement as well as its relationship to patellar height and TT-TG.
Measurement of Axial Width of the PT-LTR
Measurement of PT-LTR on MRI was replicated from the technique outlined in Mistovich et al 9 and is shown in Figure 1. The first distal axial cut demonstrating the patellar tendon without bone is identified. The most lateral point of the patella on this cut is marked (Figure 1, circle 3). The apex of the lateral trochlear ridge is identified (Figure 1, circle 2), and a line perpendicular to the posterior condylar axis is drawn (Figure 1, line 1 through circle 2). A line perpendicular to the posterior condylar axis and through the lateral aspect of the patellar tendon is drawn (Figure 1, line 1 through circle 3). The axial width of the PT-LTR is measured from the most lateral point of the patella to the point of intersection with the perpendicular line of the apex of the lateral trochlear ridge, in line with the axial axis of the patellar tendon (Figure 1, line 4).

Patellar tendon–lateral trochlear ridge distance (PT-LTR) measurement demonstrated on magnetic resonance imaging axial cut. Line 1 represents the posterior condylar axis. Circle 2 represents the lateral trochlear ridge. Circle 3 represents the most lateral aspect of the patellar tendon. Line 4 represents the axial width of the PT-LTR.
Statistical Analysis
Measurement of PT-LTR was performed by 5 individual raters, and intraclass correlation coefficients were generated to determine level of agreement. Continuous variables were analyzed using 1-way analysis of variance or the Kruskal-Wallis test. Means and standard deviations were calculated for continuous variables (age, PT-LTR, CDI, and TT-TG). Categorical variables were analyzed using the chi-square or Fisher exact test, as appropriate. Count and percentage variables were calculated for categorical variables (sex, patella alta, TT-TG >15 mm, TT-TG >20 mm, patella alta + TT-TG >15 mm, and patella alta + TT-TG >20 mm). PT-LTR was compared by surgery type using the Kruskal-Wallis test. Post hoc pairwise comparisons were produced, and a Tukey adjustment was utilized to account for multiple comparisons. PT-LTR was compared by patella alta and defined TT-TG cutoffs (TT-TG >15 mm and TT-TG >20 mm) using an independent 2-sample t test or the Wilcoxon-Mann-Whitney test, as appropriate. Stratified analyses were then conducted to compare patients with both patella alta and TT-TG at defined cutoffs. Spearman correlations were calculated between CDI and PT-LTR, as well as TT-TG and PT-LTR.
Results
Patient Characteristics
A total of 90 patients were included for this study. The mean age was 29.31 ± 13.79 years for the ACLR group, 18.82 ± 6.55 years for the MPFLR group, and 26.65 ± 9.68 years for the MPFLR+TTT group. Patients in each surgery group appeared to differ significantly by age, with the ACLR group being the oldest and MPFLR group being the youngest (P < .05). The overall cohort was 74.4% female. There was no significant difference in sex between each group (Table 1).
Patient Characteristics and Surgery Performed a

Values are reported as mean ± SD or n (%). Boldface type indicates statistical significance. ACLR, anterior cruciate ligament reconstruction; CDI, Caton-Deschamps Index; MPFLR, medial patellofemoral ligament reconstruction; TTT, tibial tubercle transfer; TT-TG, tibial tuberosity–trochlear groove distance.
Imaging Measurements
The groups differed significantly by CDI and presence of patella alta (CDI >1.2 mm) (Table 1). The largest CDI was observed in the MPFLR+TTT group (1.29 ± 0.24 mm), followed by the MPFLR group (1.18 ± 0.16 mm) and the ACLR group (1.07 ± 0.17 mm) (P < .001). There was a statistically significant difference in the rate of patella alta between groups, with the MPFLR+TTT group having the highest rate (60%), followed by the MPFLR group (44.33%) and the ACLR group (20%) (P < .01). There was a significant difference in TT-TG between groups (P < .0001) in addition to TT-TG >15 mm (P < .0001) and TT-TG >20 mm (P < .0001). The MPFLR+TTT group had the highest TT-TG (19.36 ± 3.46 mm), followed by the MPFLR group (16.23 ± 3.78 mm) and the ACLR group (10.99 ± 3.00 mm). The MPFLR+TTT group had the highest percentage of patients with a TT-TG >15 mm (96.67%) and TT-TG >20 mm (43.33%). Lastly, there was a significant difference between each surgery group when analyzing differences between having patella alta and a TT-TG >15 mm (P < .0001) and having patella alta and a TT-TG >20 mm (P < .01), with the MPFLR+TTT group having the highest rates of each (56.37% and 23.33%, respectively).
Interrater Reliability
Measurements of PT-LTR were first analyzed using the full cohort of patients and then stratified by surgery. The level of agreement between raters was moderate (0.67) to highly coordinated (0.93) (Table 2). For the purpose of continued analysis, the most senior rater's (B.E.S.S.) measurements were utilized.
Interrater Reliability a

ACLR, anterior cruciate ligament reconstruction; ICC, intraclass correlation; MPFLR, medial patellofemoral ligament reconstruction; TTT, tibial tubercle transfer.
Based on the 95% CI of the ICC estimate, values <0.5, between 0.5 and 0.75, between 0.75 and 0.9, and >0.90 are indicative of poor, moderate, good, and excellent reliability, respectively.
Relationship Between Surgery and PT-LTR Measurement
The mean PT-LTR differed significantly by surgery. Mean PT-LTR measurements were 1.15 ± 3.71 mm (lowest) for the ACLR group, 6.60 ± 6.58 mm for the isolated MPFLR group, and 12.72 ± 8.43 mm (highest) for the MPFLR+TTT (P < .0001) (Table 3). The variability in PT-LTR measurement was statistically significantly different based on the type of surgery performed (Table 4, Figure 2).
PT-LTR by Surgery Performed a
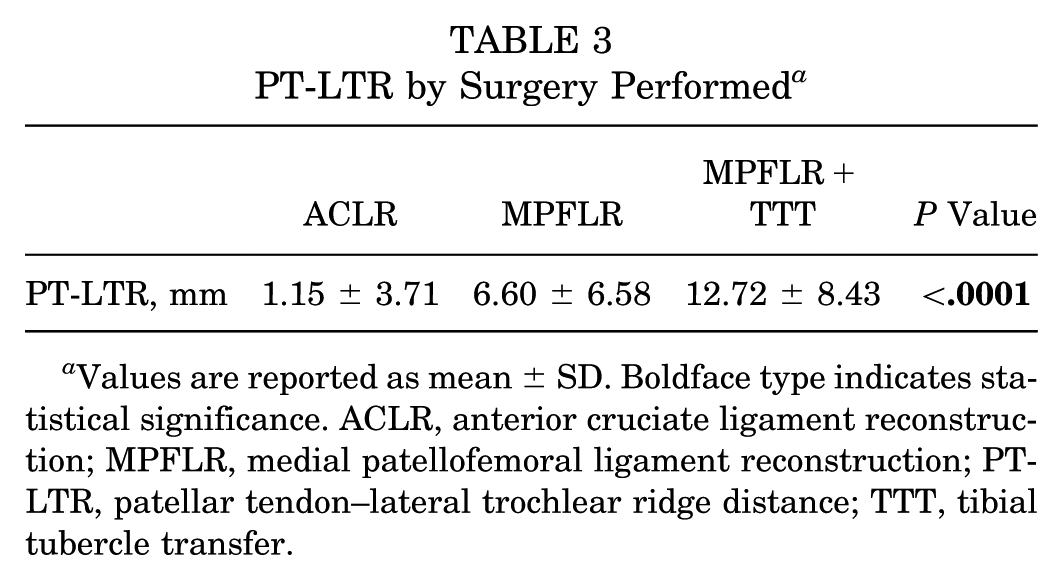
Values are reported as mean ± SD. Boldface type indicates statistical significance. ACLR, anterior cruciate ligament reconstruction; MPFLR, medial patellofemoral ligament reconstruction; PT-LTR, patellar tendon–lateral trochlear ridge distance; TTT, tibial tubercle transfer.
Pairwise Comparisons Between PT-LTR and Surgery Type a
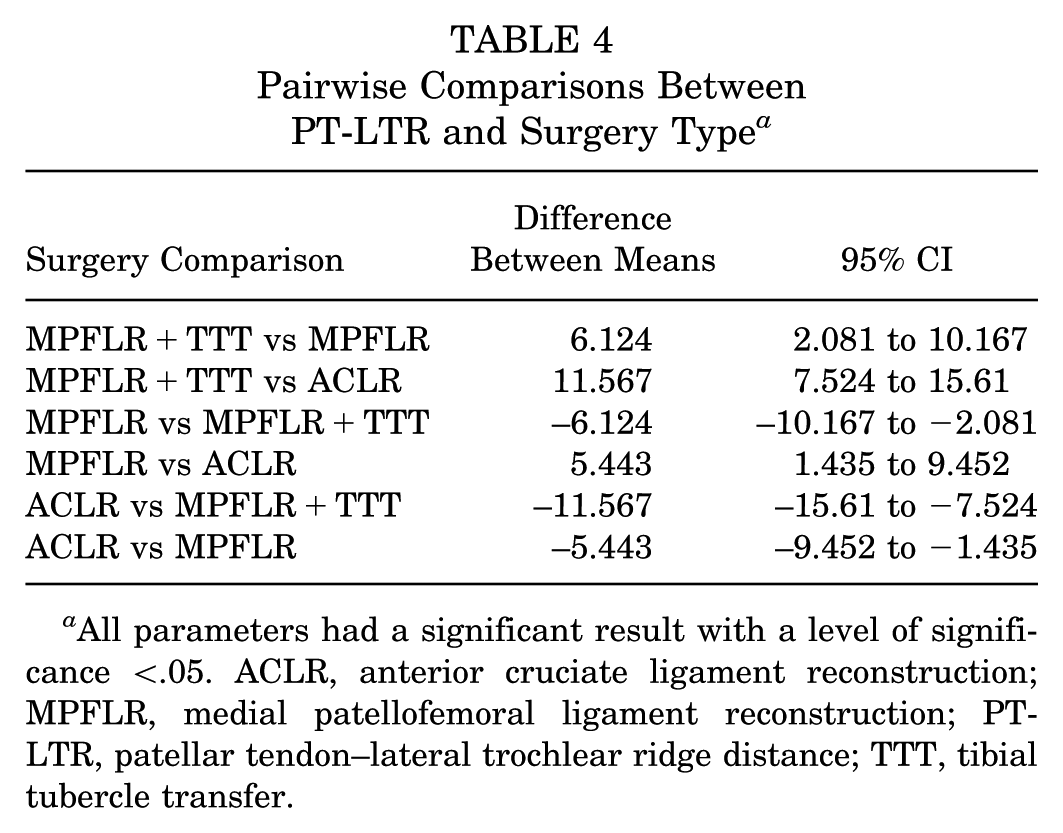
All parameters had a significant result with a level of significance <.05. ACLR, anterior cruciate ligament reconstruction; MPFLR, medial patellofemoral ligament reconstruction; PT-LTR, patellar tendon–lateral trochlear ridge distance; TTT, tibial tubercle transfer.

Mean patellar tendon–lateral trochlear ridge distance (PT-LTR) by surgery group. ACLR, anterior cruciate ligament reconstruction; MPFL, medial patellofemoral ligament reconstruction; TTT, tibial tubercle transfer.
PT-LTR Compared by Alta and TT-TG
When comparing PT-LTR by patella alta (CDI >1.2 mm), PT-LTR differed significantly across all groups. The mean PT-LTR measurements in patients with patella alta and without patella alta were 9.07 ± 8.20 and 5.32 ± 7.53, respectively (P = .03) (Table 5). The mean PT-LTR was significantly higher in patients with a TT-TG >15 mm (11.42 ± 7.36 mm) compared with those with a TT-TG ≤15 mm (1.05 ± 4.07 mm) (P < .0001). The mean PT-LTR was also significantly higher in patients with a TT-TG >20 mm (14.92 ± 7.35 mm) compared with those with a TT-TG ≤20 mm (4.83 ± 6.87 mm) (P < .0001). Patients with both patella alta and a TT-TG >15 mm had a statistically significantly higher mean PT-LTR (11.63 ± 7.69 mm) compared with those who did not meet those criteria (4.63 ± 7.19 mm) (P = .0001). Furthermore, patients with both patella alta and a TT-TG >20 mm had a statistically significantly higher mean PT-LTR (15.26 ± 6.85 mm) compared with those who did not meet those criteria (5.92 ± 7.63 mm) (P = .0037). A Spearman correlation showed that there appeared to be a strong, positive correlation (0.76; P < .0001) between TT-TG and PT-LTR and a weak correlation (0.2851; P = .0071) between CDI and PT-LTR (Table 6).
PT-LTR Compared by Patella Alta and TT-TG a

Values are reported as mean ± SD. PT-LTR, patellar tendon–lateral trochlear ridge distance; TT-TG, tibial tuberosity–trochlear groove distance.
Spearman Correlation a
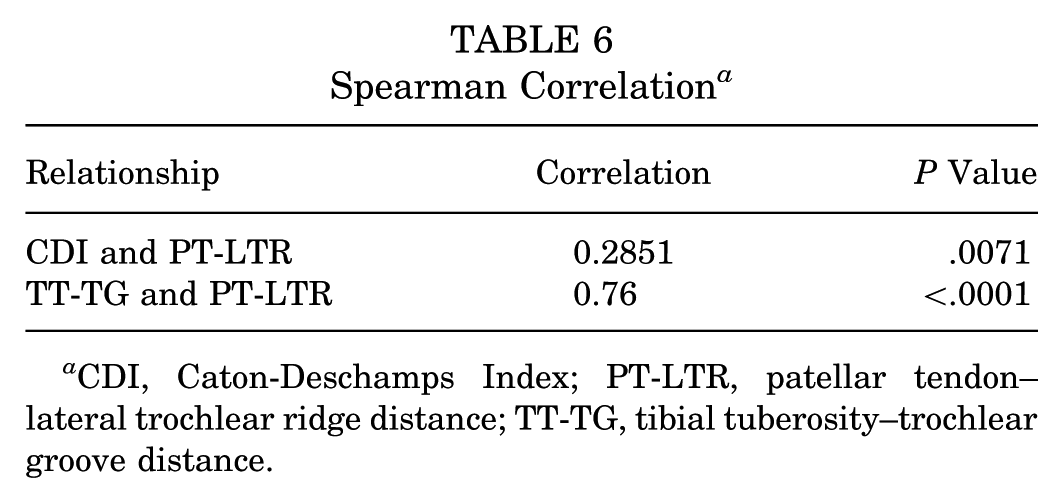
CDI, Caton-Deschamps Index; PT-LTR, patellar tendon–lateral trochlear ridge distance; TT-TG, tibial tuberosity–trochlear groove distance.
Discussion
Patellofemoral instability remains a common and complex problem lacking consensus on the optimal treatment algorithm. Multiple surgical procedures have been described to treat patellofemoral instability, and many measurements have been described to identify patients at risk of instability and aid in surgeon's operative planning. However, these measurements in isolation are unable to account for all possible pathologies within the patellofemoral joint that contribute to a patient's instability and/or maltracking. This study sought to understand if PT-LTR may be a useful tool in the assessment of patients with concomitant patellofemoral maltracking in addition to their instability. It was found that PT-LTR varied significantly between groups, with patients who received an MPFLR+TTT (representing the group of patients with maltracking in addition to instability) having the highest mean PT-LTR when compared with both control patients and patients who underwent isolated MPFLR (representing patients with instability without significant maltracking). Results from this work highlight the potential of PT-LTR as a useful quantification of the vectors at play in patients with malalignment in the setting of patellar instability. Additionally, it explored the relationship between PT-LTR, patellar height, and TT-TG and found that patients with patella alta, elevated TT-TG, or a combination of both had a higher mean PT-LTR.
Mistovich et al 9 first described PT-LTR to quantify the extent to which the patellar tendon extends laterally beyond the lateral trochlear ridge, providing a more direct measure of patellar containment within the trochlea compared with traditional measurements like the TT-TG. They determined PT-LTR to be 73% sensitive and 89% specific for patellofemoral dislocation. This measurement has also been validated in the context of recurrent patellar dislocations, where it was found to be significantly different between patients with and without recurrent instability, further underscoring its clinical utility. 9 While these studies have analyzed the PT-LTR measurement as a predictor of instability, our study found that the mean PT-LTR is significantly higher in patients who underwent MPFLR+TTT compared with that in controls and patients who underwent isolated MPFLR. This may reflect the measurement's role in identifying patellar malalignment in the setting of instability.
In the context of patellofemoral pathology, both the PT-LTR and TT-TG are measurements used to assess patellofemoral instability, but they differ in their specific applications and diagnostic accuracy. The PT-LTR is a novel measurement that quantifies how well the trochlea contains the patella, showing high reliability and specificity for patellofemoral dislocations. It demonstrated an area under the curve (AUC) of 0.876, with a sensitivity of 73% and specificity of 89% when the PT-LTR is ≥5.55 mm, making it a highly discriminative measure for patellofemoral instability. On the other hand, the TT-TG has been utilized as an assessment for patellofemoral malalignment, with an AUC of 0.806 and both sensitivity and specificity of 76% when the TT-TG is ≥13.5 mm. 12 However, the elements that comprise the TT-TG are unclear, and this measurement may represent a constellation of factors, including through knee rotation, a lateralized tubercle, a medialized trochlear groove in the setting of dysplasia, genu valgum, and femoral anteversion. It is also important to note that the TT-TG can vary significantly between imaging modalities as well as with varying degrees of knee flexion. 3 In the current study, PT-LTR was significantly higher in patients with patella alta, TT-TG >15 and >20 mm, and a combination of both patella alta and an elevated TT-TG. Hence, PT-LTR may be useful in identifying patients who have a combination of anatomic factors contributing to maltracking that further exacerbates their instability risk.
Patellar maltracking in the setting of patellofemoral instability has also been found to be associated with the presence of multiple factors including trochlear dysplasia, patella alta, and limb torsion. The presence of a high-grade J sign on preoperative physical examination has been explored as a surrogate marker for maltracking.13,15-18 The utility of PT-LTR to identify maltracking in a single measurement may help to guide surgeons to further investigate the presence of the aforementioned abnormalities and aid in the planning of the optimal treatment approach.
The current study serves as a pilot study for understanding the role of PT-LTR in instability with malalignment. Future work with a larger cohort, such as that from the multicenter JUPITER study, will seek to further understand on a larger scale if patients with recurrent postoperative instability or suboptimal outcomes after isolated MPFLR have significantly elevated PT-LTR compared with those patients successfully treated with an isolated MPFLR. Additionally, the postoperative alteration of PT-LTR and its effect on patient outcomes will be assessed in the subset of patients in this multicenter study who underwent TTT. Lastly, the individual components of the TT-TG will be investigated to better understand how they relate to the PT-LTR.
Limitations
This study is not without limitations. First, we focused on axial plane measurements only and understand measurements in the sagittal and/or coronal planes may provide further value. Second, as with other measurements, it is possible that knee position (ie, degree of flexion) at time of MRI could influence the measurement. However, all MRI examinations in this study were performed with standard protocols, helping to mitigate this variation. Additionally, the patients included in the MPFLR+TTT group were a heterogeneous mix who underwent a combination of anteriorization, medialization, and distalization, depending on their type of maltracking. Additionally, these patients were treated by a single high-volume patellofemoral surgeon with a referral practice at a single institution, and their results may not be generalizable to the community at large; however, the measurement itself likely maintains its utility in any setting.
Conclusion
Results from this study demonstrate that mean PT-LTR is significantly higher in patients who underwent combined MPFLR+TTT compared with controls and patients who underwent isolated MPFLR. These findings may reflect its role as an additional measure of patellar malalignment in the setting of patellar instability. Given these findings, further exploration of PT-LTR is warranted, as it may be a useful tool in predicting which patients may benefit from a bony procedure in addition to a soft tissue stabilization procedure.
Footnotes
Final revision submitted October 1, 2025; accepted November 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.R.D. is a consultant for CONMED. B.E.S.S. has received research support from CONMED and AOSSM/OREF, and is a consultant/speaker for Arthrex; her spouse has received consulting fees and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital for Special Surgery (2022-187).