
Abstract
Background:
Anatomic restoration of the humeral head is critical for successful shoulder replacement. Accurate measurements of the humeral head are essential for anatomic substitution.
Purpose:
To evaluate whether a best-fit circle of the humeral head, as determined from different projections of plain radiographs, can predict the humeral head implant size for either the left or right shoulder.
Study Design:
Descriptive laboratory study.
Methods:
Bilateral shoulder radiographs of 200 patients without arthropathy or other abnormal findings of the humeral head were evaluated. The best-fit circle was obtained based on 3 points: the medial and lateral endpoints of the anatomic neck and the lateral cortex below the greater tuberosity. This circle was drawn on 5 different radiographic projections (shoulder anteroposterior [AP], glenoid AP, outlet, axillary, and 30° caudal tilt) of the left and right shoulders of each patient, and the radius of each circle was measured. Agreement in the best-fit circle radius between the left and right shoulders was statistically analyzed using the intraclass correlation coefficient (ICC). There were 2 independent blinded observers who performed each measurement twice to evaluate inter- and intraobserver reliability.
Results:
Overall agreement in the radius between the right and left shoulders was excellent (all ICCs ≥0.990). The ICCs according to the radiographic view were 0.990 (95% CI, 0.986-0.993) for shoulder AP, 0.992 (95% CI, 0.989-0.995) for glenoid AP, 0.996 (95% CI, 0.994-0.997) for outlet, 0.994 (95% CI, 0.991-0.996) for axillary, and 0.993 (95% CI, 0.990-0.995) for 30° caudal tilt. Interobserver ICCs demonstrated a high level of precision: 0.987 (95% CI, 0.978-0.993) for shoulder AP, 0.986 (95% CI, 0.974-0.992) for glenoid AP, 0.974 (95% CI, 0.954-0.985) for outlet, 0.991 (95% CI, 0.984-0.995) for axillary, and 0.987 (95% CI, 0.977-0.993) for 30° caudal tilt. Intraobserver ICCs demonstrated excellent test-retest reliability: 0.983 (95% CI, 0.970-0.991) for shoulder AP, 0.989 (95% CI, 0.980-0.994) for glenoid AP, 0.987 (95% CI, 0.978-0.993) for outlet, 0.985 (95% CI, 0.973-0.991) for axillary, and 0.970 (95% CI, 0.947-0.983) for 30° caudal tilt.
Conclusion:
The best-fit circle to calculate the ideal size of a humeral head implant was able to be determined from different projections of plain radiographs.
Clinical Relevance:
Anatomic restoration of a deformed humeral head can be achieved using the best-fit circle of the contralateral humeral head as obtained from plain radiographs. This method can facilitate preoperative planning and postoperative evaluation in the anatomic restoration of the shoulder to avoid the problems of overstuffing.
Anatomic shoulder arthroplasty is a surgical treatment option for advanced glenohumeral osteoarthritis. Anatomic restoration of the shoulder joint is important in total shoulder arthroplasty or hemiarthroplasty. Accurate measurements of the humeral head are essential for anatomic substitution. Recent biomechanical studies have demonstrated improved rotational range of motion and glenohumeral joint kinematics after shoulder reconstruction using an anatomically accurate prosthetic humeral head. 8 The size of the humeral head implant affects soft tissue balancing, modifies the center of rotation, and alters the rotator cuff lever arms, consequently affecting the shoulder’s range of motion, strength, and function. 13,14 Restoring physiological soft tissue tension provides stability and prevents complications such as aseptic loosening and osteolysis induced by stress shielding. 7,11,12 Overstuffing decreases the shoulder’s range of motion and alters the lever arm, adding stress to the rotator cuff and potentially leading to the risk of secondary rotator cuff failure. 15,17
In advanced glenohumeral osteoarthritis, the humeral head is deformed because of loss of the humeral head height and the presence of peripheral osteophytes, making it difficult to preoperatively calculate the anatomically correct prosthetic humeral head size. 19 Sizing of the humeral head during shoulder arthroplasty is often performed at the time of surgery using trial implants, with consideration for dimensions of the prepared bone surface, the resected humeral head, the size of the glenoid component, and soft tissue balancing. 1 Preoperative implant templates are available. However, the application of these templates to preoperative radiographs to determine anatomic humeral head sizing or placement has yet to be validated. According to recent studies, the proximal humerus is defined as a best-fit sphere utilizing nonarticular landmarks that are preserved in the arthritic shoulder to accurately determine the humeral head size. It was originally described using 3-dimensional (3D) and reconstructed 2-dimensional computed tomography (CT) techniques. 19 Preoperative software is available that enables surgeons to virtually plan an anticipated procedure, including humeral implantation. 6 However, there is limited access to these technologies and software . Some preoperative simulation software is not open-access and may incur utilization costs. Others are proprietary and provided by specific implant manufacturers, which may affect the surgeon’s choice of implant. Furthermore, using these preoperative planning systems requires a CT scan obtained using specific protocols established by the software company. 6
We believe that the same results to assist in preoperative planning for humeral head size can be obtained from plain radiographs. The purpose of this study was to evaluate whether a best-fit circle of the humeral head, as determined from different projections of plain radiographs, can predict the humeral head implant size for either the left or right shoulder. We hypothesized that the size of the humeral head would be a match for both shoulders.
Methods
The study protocol was approved by the institutional review board of our hospital. We retrospectively reviewed the bilateral shoulder radiographs of 200 patients seen from September 2015 to December 2018 at a single institution. All patients had shoulder pain not originating from trauma and without stiffness of the shoulder joint, arthropathy, or any other abnormal findings of the humeral head. These patients mainly had soft tissue problems not affecting the appearance of the proximal humerus on plain radiographs. They exhibited no limitation in shoulder range of motion; thus, positioning their shoulders for the axillary view was possible. Diagnoses were mostly rotator cuff–related problems without arthropathy, long head of the biceps tendon–related problems, and even cervical radiculopathy.
Because we aimed to compare both shoulders (normal on plain radiographs), we excluded patients with any deformity of the proximal humerus, including osteoarthritis, rotator cuff arthropathy, rheumatoid arthritis, avascular necrosis of the humeral head, instability with Hill-Sachs lesions, a deformed proximal humerus due to previous fractures, or osteolysis or arthropathy due to infections. The mean age of the patients was 45.15 ± 7.86 years (range, 16-55 years), and 103 patients (51.5%) were men.
The best-fit circle was drawn based on 3 points: the lateral cortex below the flare of the greater tuberosity and the lateral and medial ends of the anatomic neck (Figure 1). However, in some views, the lateral cortex below the flare of the greater tuberosity was not apparent. In these cases, the articular curvature of the humeral head was used to complete the circle. The best-fit circle of the humeral head articular portion on shoulder anteroposterior (AP), glenoid AP (Grashey view), outlet, axillary, and 30° caudal tilt radiographs was drawn using a picture archiving and communication system (Marosis m-view; Marotech) (Figure 2). The axillary and outlet views required the articular curvature to complete the circle. In other views, if the rotation of the humerus was not adequate, the articular curvature was used to complete the circle.

Glenoid anteroposterior (Grashey view) radiograph demonstrating the measurement of the best-fit circle of the humeral head. The circle covers 3 points: (A) the lateral cortex below the flare of the greater tuberosity, (B) the lateral end of the anatomic neck, and (C) the medial end of the anatomic neck.

The best-fit circle of the humeral head articular portion was drawn on (A) shoulder anteroposterior (AP), (B) glenoid AP, (C) outlet, (D) axillary, and (E) 30° caudal tilt radiographs of both shoulders for each patient.
For each patient, the radius of the circle on each radiographic projection was measured and compared with the radius of the circle on the contralateral side. Drawing the best-fit circle and measuring the radius were performed independently by 2 orthopaedic surgeons (K.K. and S.J.) who subspecialized in shoulder and elbow surgery. For each patient, the average of the measurements by each observer was used to generate the final value. Both observers repeated the measurements for all 200 patients after an interval of at least 1 month.
Statistical Analysis
The intraclass correlation coefficient (ICC) with the 95% confidence interval was used to analyze agreement in the best-fit circle radius between the left and right shoulders on each radiographic projection. Scatter plots were also generated. In addition, the ICC was used to analyze the inter- and intraobserver reliability of the measurements of the 2 observers. Intraobserver reliability was calculated from the mean difference and 95% confidence interval of repeated readings by observer 1. ICC values were interpreted as poor if <0.40, fair if 0.40-0.59, good if 0.60-0.74, and excellent if 0.75-1.00. 5 For all analyses, statistical significance was set at P ≤ .05. Statistical analyses were performed using SPSS Statistics for Windows (Version 26.0; IBM).
Results
This study demonstrated excellent overall agreement in the best-fit circle radius between the right and left shoulders on all radiographic projections (all ICCs ≥0.990). The ICCs according to the radiographic view are shown in Table 1, and scatter plots of the data sets are shown in Figure 3.
Agreement in Best-Fit Circle Radius Between Right and Left Shoulders a

a Data are shown as intraclass correlation coefficient (95% CI). P < .001 for all radiographic views. AP, anteroposterior.

Scatter plots of the best-fit circle radius (in mm) for the right and left shoulders according to the radiographic view: (A) shoulder anteroposterior (AP), (B) glenoid AP, (C) outlet, (D) axillary, and (E) 30° caudal tilt.
The interobserver ICCs were excellent (all ICCs ≥0.974), demonstrating a high level of precision, regardless of the radiographic view. The intraobserver ICCs demonstrated excellent test-retest reliability (all ICCs ≥0.970). The inter- and intraobserver reliability values according to the radiographic view are shown in Table 2.
Interobserver and Intraobserver Reliability of Best-Fit Circle Radius Measurements a
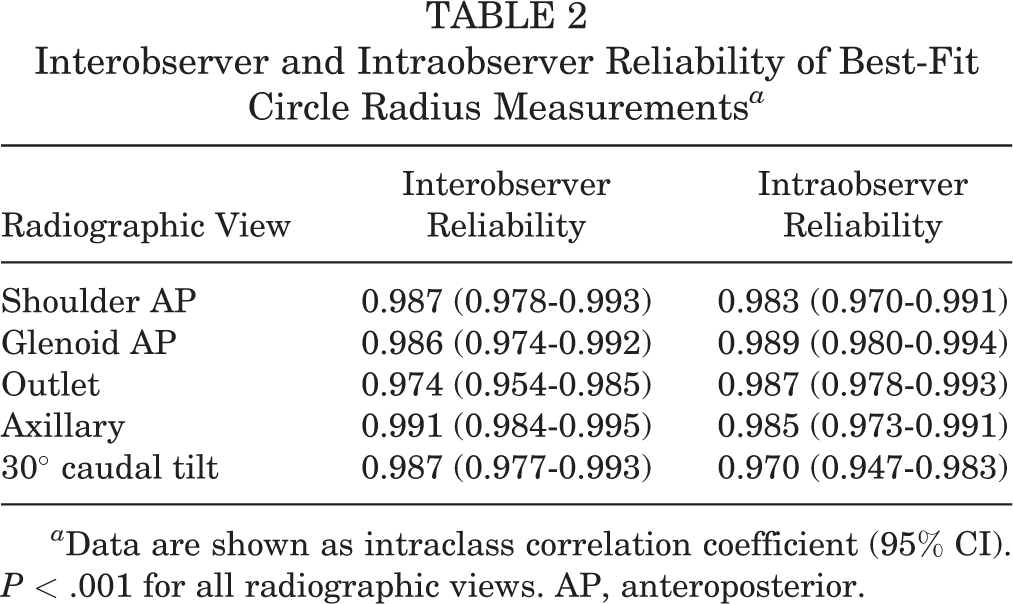
a Data are shown as intraclass correlation coefficient (95% CI). P < .001 for all radiographic views. AP, anteroposterior.
Discussion
There was excellent agreement in the best-fit circle radius between the right and left shoulders, regardless of the radiographic view (all ICCs ≥0.990; P < .001 for all). Similarly, we found excellent inter- and intraobserver reliability when measuring the best-fit circle radius across all radiographic views (all ICCs ≥0.974 and ≥0.970, respectively; P < .001 for all).
Anatomic shoulder replacement for glenohumeral arthritis is associated with excellent outcomes if the surgeon can restore the normal kinematics of the glenohumeral joint via accurate sizing of the prosthesis and soft tissue tensioning. 2,4,15 However, because the articular surface is generally deformed from the arthritic process, it is often difficult to accurately assess the correct size of the premorbid humeral head. 1
Recent studies have reported the size of the humeral head in anatomic shoulder replacement. Youderian et al 19 demonstrated and validated the concept using CT to demonstrate that a sphere superimposed on specific preserved extra-articular landmarks of the proximal humerus or a circle in the midcoronal plane can accurately predict the humeral head size in glenohumeral osteoarthritis. Savin et al 16 used a 3-point measurement technique based on conventional radiographs to predict the humeral head size utilizing extra-articular landmarks within a small margin of error.
Their studies had limitations. Youderian et al 19 reported that the humeral head was measured via 3D imaging after CT. Various software has recently been developed for preoperative planning of the anatomic humeral head based on CT scans of sufficient quality to allow 3D reconstruction. 18 However, it is difficult to perform accurate 3D CT in all hospitals. Savin et al 16 reported that only a single radiographic projection with external rotation at 15° (best view based on 3 nonarticular landmarks) in the AP dimension was used. It is difficult to determine the humeral head size accurately using only 1 radiographic view. We identified a best-fit circle based on 5 radiographic views to represent the full shoulder more accurately.
We have demonstrated that a circle formed by nonarticular landmarks or a combination of nonarticular landmarks and the articular surface in both shoulders was consistent on shoulder AP, glenoid AP (Grashey view), outlet, axillary, and 30° caudal tilt radiographs. The circles in the 5 radiographic views were matched on both shoulders. Anatomic restoration of a deformed humeral head can be achieved using the opposite humeral head. Humeral head sizes were similar with regard to the left and right shoulders in the same patient; therefore, using the opposite shoulder (if not deformed) is a way to estimate the implant size for the operative shoulder.
The best-fit circle method can also be applied to evaluate postoperative plain radiographs (Figure 4). A best-fit circle was drawn on the undeformed humeral head of the opposite shoulder. The same circle was then applied to the deformed humeral head, predicting the size of the original humeral head. The predicted size of the humeral head implant was adequate in both cases. However, in the first case, 1 of the 3 points on the best-fit circle did not match: the lateral cortex below the flare of the greater tuberosity showed overstuffing. This finding suggests that better restoration would have been achieved if the cut had been made at a lower level of the humeral neck. In the second case, all 3 points matched, and the resulting restoration of the native humeral head was good. Applying the best-fit circle method to predict the actual humeral head implant size requires the placement of a calibration marker on the patient for reference. However, the incidence of bilateral glenohumeral osteoarthritis is 3.1% to 7.7% according to Ibounig et al. 10 Consequently, the best-fit circle method may be ineffective in these patients.

(A) Osteonecrotic deformity of the humeral head in the left shoulder of one patient and (B) osteoarthritic changes in the humeral head in the right shoulder of another patient. A best-fit circle was drawn on the undeformed humeral head of the opposite shoulder, and then, the same circle was applied to the deformed humeral head, predicting the size of the original humeral head.
Limitations
Our study is not without limitations. First, we assumed that the humeral head was a sphere that could be replaced with a circle in various directions. However, the humeral head is not a perfect sphere, and its radius of curvature in the AP dimension (axial plane) is smaller than in the superoinferior dimension (coronal plane), with an average ratio of 0.92. 9 According to 1 anatomic study, 88.2% of humeral heads do not differ more than 1 mm in the axial and coronal planes, confirming that the majority of shoulders form true spheres. 3
Second, we measured a circle using the 3-point nonarticular landmark technique. However, it was difficult to capture 3 points on all simple radiographs, and if only 1 or 2 points were confirmed, we used the articular portion of the humeral head in place of the third point. Savin et al 16 utilized a slightly more precise 3-point nonarticular landmark technique because the articular surface is spherical in the center and may be more elliptical in the periphery, which may decrease the reliability of the articular surface measurements. 9
Third, although the humeral head size can be determined accurately via preoperative imaging, the actual humeral head size used is influenced by other surgical factors. Differences between planned and actual humeral head sizes can be attributed to variable locations of the osteotomy site and the definition of the anatomic neck location or the angle of osteotomy in relation to the humeral shaft. We estimated the size of the preoperative humeral head using only 5 radiographic views without evaluating other conditions, leading to possible differences in the size of the humeral head during the actual operative procedure.
Finally, the study was performed on patients without arthropathy or other abnormal findings of the humeral head. Therefore, radiological comparisons were made with the normal contralateral shoulder. Most patients did not require additional evaluations, such as CT, and no patients underwent arthroplasty. Consequently, we did not conduct comparisons with the conventional measurement method. The best-fit circle method applied preoperatively in actual clinical practice, in most cases, matched the humeral head implant size chosen intraoperatively, in the range of implant sizes provided by the manufacturer. For example, the measurement by the best-fit circle method was 43 mm, and the actual implant used was 41 or 44 mm (implants were provided in sizes with 3-mm differences: 38, 41, 44, 47, 50, and 53 mm). Comparisons of the humeral head implant size predicted by the best-fit circle method with the conventional measurement method and with the actual size of the humeral head implant chosen intraoperatively should be a focus of research in the future.
Despite these limitations, our study demonstrates that the size of the humeral head was similar bilaterally based on simple multidirectional radiographic analysis, thus confirming the humeral head size of the contralateral shoulder when the humeral head is deformed because of advanced glenohumeral arthritis.
Conclusion
The best-fit circle to calculate the ideal size of the humeral head implant was able to be determined from different projections of plain radiographs. Using this method, anatomic restoration of the deformed humeral head can be achieved using the humeral head of the contralateral shoulder. This method can facilitate preoperative planning and postoperative evaluation in the anatomic restoration of the shoulder to avoid the problems of overstuffing.
Footnotes
Acknowledgment
The authors acknowledge Seon-Ah Cha, MD, PhD (Division of Endocrinology and Metabolism, Department of Internal Medicine, Wonkwang University Sanbon Hospital), for assisting with statistical analysis. It is because of her hard work, diligence, and attention to detail that this study was possible.
Final revision submitted March 17, 2023; accepted April 14, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St Vincent’s Hospital (VC19RESI0008).