
Abstract
Purpose:
To compare the outcomes of total shoulder arthroplasty (TSA) with posterior capsule plication (PCP) and reverse shoulder arthroplasty (RSA) in patients with primary osteoarthritis, posterior subluxation, and bone loss (Walch B2).
Patients and methods:
All shoulders undergoing anatomic TSA with PCP were retrospectively identified (group 1, G1) and compared to shoulders undergoing RSA (group 2, G2) for Walch B2 osteoarthritis. There were 15 patients in G1 (mean (SD) age and follow-up of 70.5 (7.5) years and 42.8 (18.4) months, respectively) and 16 patients in G2 (mean (SD) age and follow-up of 72.6 (5.4) years and 35.1 (14.2) months, respectively).
Results:
Both groups had substantial improvements in pain and function. In G1, results were excellent in 80% and satisfactory in 20%, compared to 81% and 6% in G2, respectively (p = 0.2). The mean (SD) American Shoulder and Elbow Surgeons score was 91.2 (6.7) and 80.3 (14.3) in G1 and G2, respectively (p = 0.08). The mean Simple Shoulder Test score was 10.6 in G1 and 8.5 in G2 (p = 0.01). There were no reoperations in either group, but G1 had seven postoperative complications.
Conclusions:
The outcomes of TSA with PCP are comparable to RSA in patients with osteoarthritis and biconcave glenoids. However, TSA leads to more complications while RSA leads to lower functional outcomes.
Keywords
Introduction
Anatomic total shoulder arthroplasty (TSA) and reverse shoulder arthroplasty (RSA) have both been reported to provide successful outcomes in terms of pain relief and function in patients with osteoarthritis. 1 –7 However, shoulder arthroplasty in the presence of posterior subluxation of the humeral head and posterior glenoid bone loss warrants a separate consideration. 8 –11
Walch et al. developed a computed tomography (CT)-based classification system for primary osteoarthritis based on subluxation and glenoid bone loss. 12,13 In Walch B category, osteoarthritis is associated with static posterior subluxation; in the biconcave (B2) subcategory, there is posterior glenoid erosion. Posterior subluxation leads to elongation of the posterior soft tissues, which can compromise restoration of adequate soft tissue balancing at the time of shoulder arthroplasty. In addition, implantation of an anatomic glenoid component may be challenging in the B2 subcategory due to bone loss and increased retroversion.
When excessive posterior subluxation is noted intraoperatively at the time of TSA, options include posterior capsule plication (PCP) or intraoperative conversion to RSA. The outcomes of PCP in the setting of TSA in patients with type B osteoarthritis are largely unknown. Walch et al. reported acceptable results with TSA in patients with B2 glenoids, but the nine shoulders that underwent PCP ended up with worse motion. 11 Mizuno et al. first reported on the use of RSA in patients with primary osteoarthritis and severe posterior subluxation. 3 To date, no studies have compared the relative advantages and disadvantages of TSA with PCP versus RSA in patients with excessive intraoperative posterior subluxation.
The purpose of this study was to compare the clinical and radiographic outcomes, complications and reoperations of TSA with PCP and RSA for primary glenohumeral osteoarthritis with severe posterior subluxation and marked intraoperative soft tissue imbalance.
Methods
Following Institutional Review Board approval (Mayo Clinic Institutional Review Board: IRB# 15-006671), our Institutional Joint Registry database was queried to identify all patients who underwent primary anatomic TSA between January 2004 and December 2013 by three surgeons (RHC, JWS, and JSS). Inclusion criteria were age over 18 years, with primary osteoarthritis with severe posterior subluxation and bone loss (Walch B2 glenoid); PCP performed during primary anatomic TSA; minimum follow-up of 2 years or until failure; use of all-polyethylene glenoid components; and adequate radiographs and CT. 12,13 Patients were excluded if the indication for TSA was secondary osteoarthritis or if there was evidence of a full-thickness rotator cuff tear either in preoperative imaging studies or intraoperatively. Shoulders requiring structural glenoid bone graft were also excluded. These shoulders represented group 1 (G1).
Once shoulders in G1 had been identified, a matched group for comparison was extracted from all primary RSA performed by the same surgeons during the same time period (group 2, G2). The start date of the study for both implant styles (January 2004) was selected based on the date RSA was first implanted at the authors’ Institution. Inclusion criteria for shoulders in G2 included a diagnosis of primary osteoarthritis with severe posterior subluxation and bone loss (Walch B2 glenoid) and similar age and follow-up as those shoulders in G1. Patients were excluded from G2 in the presence of superior humeral head subluxation 14 or evidence of full-thickness rotator cuff tearing on preoperative imaging or intraoperatively.
A retrospective review of the medical charts was conducted to extract all relevant data for the present study. After data collection, a radiographic assessment session was conducted in which all preoperative, early follow-up, and last follow-up radiographs were evaluated in consensus by two senior surgeons (JWS and JSS) blinded to the clinical outcomes. In addition, relevant preoperative radiographic measurements were also obtained by a separate researcher. Glenoid retroversion measurements were performed on axial images from CT scans in all but two shoulders from G1 for whom only radiographs were available.
Patients
A total of 880 primary anatomic TSA cases were performed during the study period. Fifteen shoulders of 15 patients met the inclusion criteria (G1, TSA with PCP). A total of 937 primary RSA cases were identified in the same study period, from which primary osteoarthritis was the underlying diagnosis in 106 cases. Of these, 32 (30%) had B2 glenoids, and 16 of them had a minimum follow-up of 2 years. Table 1 compares the demographic and follow-up characteristics between the two groups. The median (range) length of radiographic follow-up was 27 (1.5–71) months. There were 14 men and 1 woman in G1 and 11 men and 5 women in G2 (p = 0.08). The shoulder arthroplasty was done on the dominant side of 10 shoulders in G1, and 4 shoulders in G2 (p = 0.06). Most recent follow-up was through a physical exam in 14 (45%) cases (8 in G1 and 6 in G2) and through a validated questionnaire follow-up in 17 (55%) cases (7 in G1 and 10 in G2). 15,16
Comparison of demographic and follow-up characteristics between both groups.
BMI: body mass index; TSA: total shoulder arthroplasty; RSA: reverse shoulder arthroplasty.
The paleoglenoid, intermediate, neoglenoid retroversion angles, and the percentage of posterior subluxation of the humeral head in each group are summarized in Table 2. The measurements were performed following the methods described by Walch et al. 11,17 . The mean (SD) of paleoglenoid, intermediate, and neoglenoid retroversion angle in both groups was 16.2° (9.1°), 20.8° (8.7°), and 22.4° (11.1°), respectively. The mean (SD) posterior subluxation in both groups was 72.7% (10%). The degree of preoperative radiographic superior subluxation of the humeral head was none in 23 cases (7 in G1 and 16 in G2), mild (<25%) in 6 cases (all G1), and moderate (25–50%) in 2 cases (all in G2).
Preoperative radiographic measurements in both groups.

RSA: reverse shoulder arthroplasty; TSA: total shoulder arthroplasty.
Surgical procedures
All surgical procedures were performed through a deltopectoral approach. For G1, 12 Comprehensive Total Shoulder System ® (Biomet, Warsaw, Indiana, USA), 2 ReUnion Total Shoulder System ® (Stryker, Mahwah, New Jersey, USA), and 1 Cofield Total Shoulder System ® (Smith and Nephew, Memphis, Tennessee, USA) implants were used. The glenoid component for the BIOMET ® implants was hybrid pegged all-polyethylene base (one small, seven medium, and four large size). The other glenoid components were the Cofield ® glenoid peg base (large) and the ReUnion ® self-pressuring glenoid (sizes 44 and 48 mm). Cement was used for all glenoid components but not for any humeral stem. No bone graft was used for any of the patients in G1. The need to perform a PCP was decided intraoperatively at the time of TSA when there was more than 50% posterior translation of the trial humeral head, despite increasing the lateral offset of the glenohumeral joint as much as possible while still allowing subscapularis closure. The technique of PCP involved using a bone hook in the trunnion of the broach to translate the humerus laterally and gain access to the posterior capsule from the front, placing multiple sutures to imbricate the posterior capsule and cuff, and tying all the sutures after removal of the bone hook (Figure 1). After surgery, shoulders in G1 were immobilized in external rotation for 6 weeks to facilitate healing of the PCP. For G2, all implants were Comprehensive Total Shoulder System prostheses. All baseplates used were mini size 25 mm with porous coat. There were eight patients with 36-mm-sized glenosphere (three of them with 3-mm offset) and eight with 41-mm-sized glenospheres (two of them with 3-mm offset). There were seven mini and nine micro humeral stems (all porous coated). Cement was not used for any of the patients in G2. In all cases, eccentric glenoid reaming was performed. In cases with more severe bone loss that would compromise baseplate fixation and stability, bone autograft from the humeral head was used for the glenoid component (this was needed for four patients). The mean (SD) operative time was 94 (14) min for G1 and 87 (14) min for G2.

Illustrations of the PCP technique. (a) Placement of sutures after retracting the humerus laterally to expose the posterior capsule. “Used with permission of Mayo Foundation for Medical Education and Research. All rights reserved.” (b) Final appearance of the PCP before implantation of the humeral head. “Used with permission of Mayo Foundation for Medical Education and Research. All rights reserved.” PCP: posterior capsular plication.
Outcome assessment
The following outcomes were collected: (1) preoperative pain (1 no pain, 2 mild pain, 3 pain after usual activities, 4 moderate pain, and 5 severe pain), active range of motion (ROM) for forward flexion, external rotation and internal rotation, and strength for shoulder elevation, abduction, external rotation, and internal rotation (0 = no movement is observed; 1 = visible contraction, no segment movement; 2 = active movement upon resistance with gravity removed; 3 = active movement against gravity; 4 = active 122 movement against gravity and examiners’ resistance; and 5 = normal strength); (2) preoperative radiograph characteristics; (3) postoperative pain, ROM, and strength; (4) postoperative radiograph characteristics in the early (within 6 weeks after surgery) and final follow-up; (5) complications and reoperations; (6) functional outcomes (Neer rating scale, Simple Shoulder Test (SST), and American Shoulder and Elbow Surgeons (ASES) score); and (7) patient satisfaction on a 1–5 scale (where 1 is not satisfied, 2 is fair satisfaction, 3 is good satisfaction, 4 is very good satisfaction, and 5 is excellent satisfaction).
Information on the subjective feeling of stability was also collected from the charts. The Neer rating system used in this study was first described by Neer et al. 4 , and later modified by Cofield 1 . The result was considered excellent if the patient had no or slight pain, active abduction to 140°, and external rotation to 45° and was satisfied with the procedure. A satisfactory result consisted of no, slight, or moderate pain only with vigorous activity, active abduction to 90°, external rotation to 20°, and the patient being satisfied with the procedure. A result was graded as unsatisfactory if any of the above criteria were not met or if the patient needed a revision procedure. A clinical failure was defined as the need for revision surgery to increase stability regardless of the failure etiology.
Radiographic data collected included the degree of superior subluxation of the humeral head or implant in all three time periods, glenoid and humeral lucent lines, the presence of glenoid loosening, and shifting in position of the glenoid or humeral components. The degree of subluxation was categorized as none, mild (<25%), moderate (25–50%), and severe (>50%).
Glenoid radiolucent lines were classified as 0 (none), 1 (faceplate only), 2 (1 mm incomplete), 3 (1 mm complete), 4 (1.5 mm incomplete), 5 (1.5 mm complete), and 6 (2 mm complete). Humeral radiolucent lines were classified as 0 (none), 1 (1 mm incomplete), 2 (1 mm complete), 3 (1.5 mm incomplete), 4 (1.5 mm complete), 5 (2 145 mm in 1–2 zones), 6 (2 mm in 3–4 zones), and 7 (2 mm complete). The presence of glenoid loosening was determined in consensus between the two senior surgeons involved in radiograph analysis. Radiographic success of the PCP was considered as absence of posterior subluxation in the most recent radiograph (Figure 2). Scapular notching according to Sirveaux et al. 18 was also recorded.
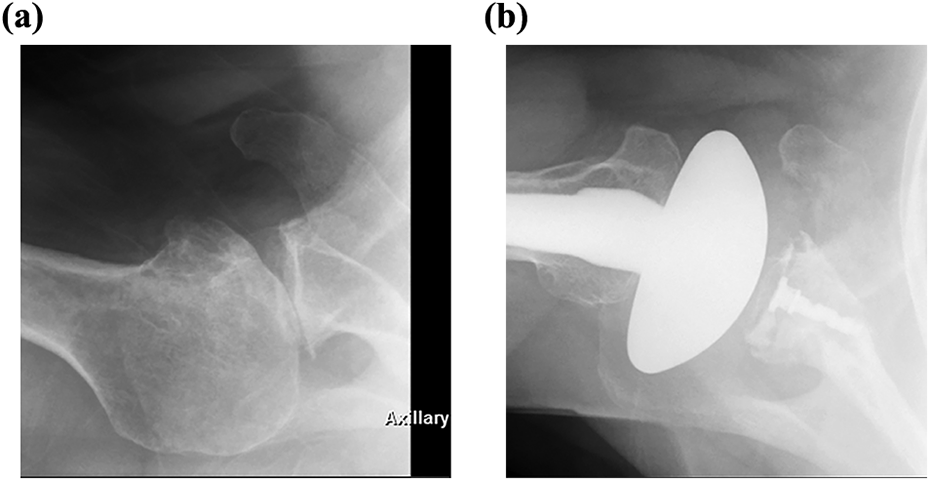
Example of a radiographically successful PCP. (a) Preoperative axillary view radiograph demonstrating posterior subluxation of the humeral head in a patient with a B2 glenoid. (b) Postoperative axillary view radiograph at 2.5 years demonstrates the humeral head being well-centered on the glenoid. PCP: posterior capsular plication; B2: biconcave.
Statistical analysis
Descriptive statistics were used to summarize the outcomes. Data were reported as number of cases (n), percentage, mean, median, SD, and range. Nonparametric tests were used due to the limited sample size. For the comparison between preoperative and postoperative outcomes, a Wilcoxon’s or Fisher’s exact test was applied as indicated. A Fisher’s exact test was also used for the comparison between non-paired qualitative variables, and a Mann–Whitney U test was used to compare non-paired quantitative variables between dichotomous variables. The α level was set at 0.05. All the statistical analysis was conducted using the SPSS v.21 (SPSS Inc., Chicago, Illinois, USA).
Results
Shoulder arthroplasty resulted in substantial improvements in pain, motion, and function in both groups (Table 3). At the most recent follow-up in G1, results were considered excellent in 12 shoulders (80%) and satisfactory in 3 shoulders (20%). In G2, results were excellent in 13 (81%), satisfactory in 1 (6%), and unsatisfactory in 2 (13%; p = 0.2). The reason for the unsatisfactory results in two shoulders was related to the lack of active external rotation. These two patients had preoperative rotator cuff deficiency with 3+/5 and 4−/5 active external rotation. The mean (SD) ASES score was 91.2 (6.7) and 80.3 (14.3) in G1 and G2, respectively (p = 0.08). The simple shoulder test score was significantly better in G1 compared to G2 (mean 10.6 and 8.5, respectively; p = 0.01). None of the patients had a subjective feeling of instability and there were no cases of scapular notching.
Comparison of preoperative and postoperative pain, range of motion, and strength between both groups.

ABD: abduction; ER: external rotation; FF: forward flexion; IR: internal rotation; ROM: range of motion; RSA: reverse shoulder arthroplasty; TSA: total shoulder arthroplasty. ** Statistically significant.
There were no reoperations in either group. However, four shoulders (26%) in G1 were considered a radiographic failure: two (13%) cases of glenoid component loosening and three (20%) cases (one patient had both) of radiographic failure of the PCP (Figure 3). Two additional shoulders (13%) in G1 developed progressive late cuff insufficiency with superior migration of the humeral component in G1. In G1, there were 10 (66%) cases without superior migration of the humeral component, 3 (20%) with mild superior migration, and 2 (14%) with severe superior migration of the humeral component. There were 11 (73%) cases without posterior subluxation of the humeral head prosthesis, 1 (7%) with mild posterior subluxation, and 3 (20%) with moderate posterior subluxation. In G1, glenoid radiolucent lines were as follows: none in six (40%) cases, type 1 in five (34%) cases, type 2 in two (13%) cases, and type 6 in two (13%) cases. There were no cases of glenoid radiolucent lines in G2 and no cases of humeral component radiolucent lines in either group.

Example of a radiographic failure of the PCP. (a) Preoperative axillary view radiograph demonstrating end-stage osteoarthritis with humeral head subluxation and posterior glenoid bone loss. (b) Postoperative axillary view radiograph at 30 months demonstrating moderate posterior subluxation of the humeral head implant. PCP: posterior capsular plication.
Discussion
When anatomic TSA is performed for primary glenohumeral osteoarthritis in patients with preoperative posterior subluxation and bone loss (Walch B2 category), adequate soft tissue balancing and tracking may not be possible in a number of shoulders despite adequate component version, soft tissue releases, and use of a thicker humeral head to tension the posterior capsule and cuff. In these circumstances, the surgeon is faced with two alternatives: plication of the posterior capsule or intraoperative conversion to a RSA.
The results of our study seem to indicate that TSA with PCP and RSA provide similar outcomes in terms of pain, motion, and strength. As a group, RSA seems to provide slightly worse functional outcomes (as measured using the SST and ASES scores); however, use of TSA with PCP comes with the cost of some risk of glenoid component loosening and/or soft-tissue failure (cuff deficiency or recurrence of posterior subluxation).
Posterior glenoid erosion with posterior subluxation of the humeral head is not uncommon in primary osteoarthritis 12 and has a negative effect on the outcomes of shoulder arthroplasty. 8,9,11 The surgical treatment of shoulder osteoarthritis in this scenario includes hemiarthroplasty (HA) with or without asymmetric reaming (anterior reaming), TSA with asymmetric reaming, TSA with glenoid bone graft, TSA with augmented glenoid component, or RSA. 19,20 HA provides poor results in the context of eccentric posterior glenoid wear. 9,10 In addition, the outcomes of HA are worse compared to TSA in the presence of posterior glenoid bone loss. 8 Although some authors have advocated HA with eccentric anterior reaming, 21 –23 there are concerns on joint line medialization that could worsen posterior shoulder instability. 19,20 Even in the setting of TSA, eccentric reaming alone is not recommended if glenoid retroversion is greater than 15° or the posterior bone loss is greater than 8 mm. 24 –26 Correction of the glenoid retroversion with eccentric anterior reaming leads to joint line medialization, use of a smaller glenoid component, medial cortex perforation, and medial subsidence. 27 Bone graft for the posterior glenoid bone during TSA has provided high rates of glenoid loosening (11% at 5 years), graft failure (29%), and unsatisfactory results (between 47% and 71%). 11,16,28 The use of augmented glenoid components is appealing. 20 However, the outcomes of this technique have been discouraging, 29 and clinical data are only available with short-term follow-up. 30 Given the suboptimal or poor outcomes of these management strategies in the complex scenario of B2 glenoids, the use of RSA has been recommended. 3 Successful management of primary osteoarthritis in B2 glenoids with TSA involves taking into consideration the dual problem of posterior subluxation and bone loss. Posterior humeral head subluxation has been found to be independent from humeral and glenoid retroversion 31,32 and can recur even when the retroversion has been corrected. 8,32 –35 The use of an increased humeral head implant thickness alone to increase soft tissue tension is unlikely to correct posterior subluxation. 11 Therefore, the addition of soft tissue procedures at the time of TSA will be necessary in some shoulders. The outcomes of TSA in patients with B2 glenoids have been reported by several authors. 11,32,33,36,37 Nonetheless, the number of patients with B2 is small and none of these had a concomitant PCP at the time of TSA. 32,33,36,37
Walch et al. reported the outcomes of TSA in 75 patients (92 shoulders) with B2 glenoids at a mean follow-up of 77 months. 11 Nine shoulders (9.8%) additionally underwent PCP for intraoperative instability in neutral rotation (static posterior instability of the humeral head >50% of the humeral head diameter). Patients with PCP had worse forward flexion compared to those without PCP. Our study did not find significantly lower forward flexion with TSA and PCP compared to RSA. In the study by Walch et al., rates of glenoid loosening and revision were 20.6% and 16.3% at 6 years. 11 In our study, rates of glenoid loosening and recurrent posterior subluxation were 13% and 20%, respectively.
Mizuno et al. reported the outcomes of RSA in 27 patients with shoulder osteoarthritis and biconcave glenoids. 3 At a mean follow-up of 54 months, there were significant improvements in constant score, pain, activities of daily living, strength, and motion. They were no cases of recurrent posterior instability, but other complications included three cases of nerve injury (1 permanent) and one case of early glenoid loosening. The outcomes of our study are comparable to those reported by Mizuno et al. 3 (Table 4). Mizuno et al. obtained less external rotation but greater internal rotation compared to our study, which may be explained by differences in humeral component version. Differences in active motion may also be explained by the status of the rotator cuff. Despite no obvious full-thickness rotator cuff tear is present at the time of shoulder replacement, poor tendon tissue quality may imply progression toward tendon tear in the postoperative period. This could lead to poor active motion, so some authors advocate for the association of tendon transfers, particularly for external rotation. 38
Comparison of outcomes between our study and those reported in the literature.
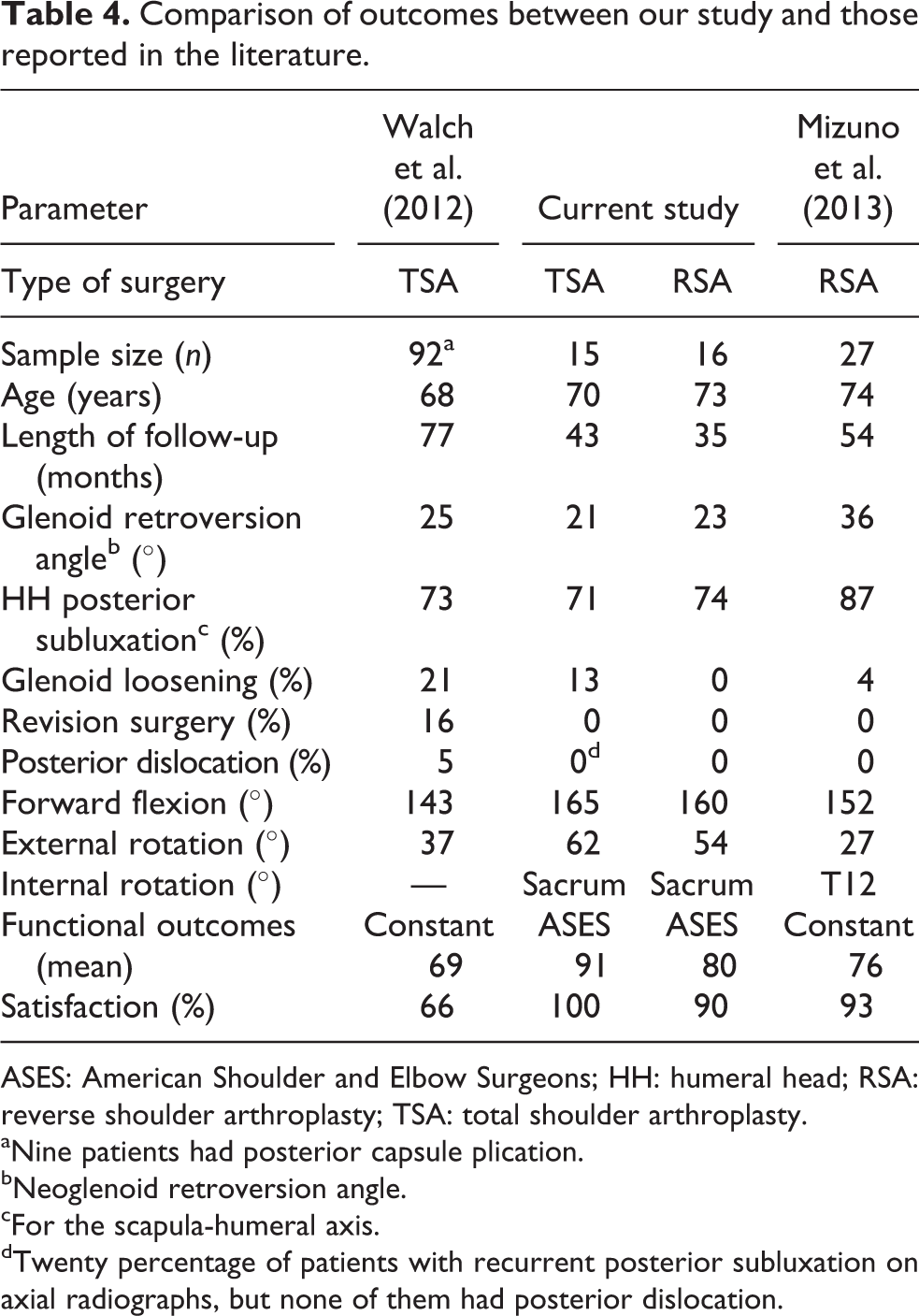
ASES: American Shoulder and Elbow Surgeons; HH: humeral head; RSA: reverse shoulder arthroplasty; TSA: total shoulder arthroplasty.
aNine patients had posterior capsule plication.
bNeoglenoid retroversion angle.
cFor the scapula-humeral axis.
dTwenty percentage of patients with recurrent posterior subluxation on axial radiographs, but none of them had posterior dislocation.
The present study has some limitations. First, the status of the rotator cuff may be different between groups. Despite attempts to limit the influence of cuff disease, it is possible that differences in the status of the rotator cuff (as evidenced by lower preoperative ER and IR strength—Table 3) explain differences in the outcomes (lower functional outcomes in G2 compared to G1). Second, an exact pair-matched (for age, length of follow-up, gender, and anthropometric characteristics) comparison group could not be established. Despite this limitation, the 2 groups were comparable for age, gender, anthropometric characteristics, and length of follow-up (Table 1). Third, it might be possible that G1 had a worse prognosis for instability compared to G2 because all patients undergoing TSA with PCP had intraoperative instability, whereas not all patients in the RSA had intraoperative instability. Finally, the present study had a small sample size for the two groups, with a relatively short follow-up.
Conclusions
The clinical outcomes of TSA with PCP are comparable to RSA in patients with osteoarthritis and preoperative posterior subluxation (Walch B). However, TSA is associated to late cuff insufficiency, recurrent posterior subluxation, and glenoid loosening in some shoulders, while RSA leads to somewhat lower functional outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Cofield has royalties from Smith/Nephew, DJO. Dr Sperling receives royalties from Biomet, and Dr Sanchez-Sotelo receives royalties from Stryker. No other authors have anything to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.