
Abstract
Background:
There is no consensus regarding the management of posterior cruciate ligament (PCL) avulsion fractures and the expected outcomes after treatment.
Purpose:
To systematically review clinical outcomes and complications after management of tibial-sided avulsion fractures of the PCL.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A literature search of Scopus, PubMed, Medline, and the Cochrane Central Register for Controlled Trials was performed in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Included were studies with evidence levels 1 to 4 that reported clinical outcomes after treatment of PCL tibial-sided avulsion fractures in humans. The quality of the included studies was performed using the Methodological Index for Non-Randomized Studies (MINORS) criteria. A meta-analysis was performed for patient-reported outcome measures using random-effects modeling with 95% CIs.
Results:
A total of 58 studies published between 1999 and 2022 were identified. The mean MINORS score was 9.90 ± 4.12, indicating overall low-quality evidence with high risk of bias. The studies comprised 1440 patients (mean age, 32.59 ± 5.69 years; 75.2% males) with a mean follow-up of 26.9 ± 19.6 months (range, 5.3-126 months). Most patients were treated with open surgery (63.6%), followed by arthroscopic surgery (29.7%) and nonoperative treatment (6.7%). All patients reported significant posttreatment improvement in both subjective and objective outcomes (P < .05 for all). Arthroscopic surgery was associated with lower postoperative posterior tibial translation compared with open surgery (range, 0.6-3.2 vs 1.7-3.1 mm), greater preoperative to postoperative improvement in Lysholm score (54.6 vs 48.8; P < .0001), higher postoperative Tegner score (6.64 ± 1.03 vs 6.14 ± 2.29; P = .0448), and a higher rate of return to sport (100% vs 89.5%; P = .009). Nonoperative management was associated with a significantly lower fracture union rate (87% vs 99.1%; P < .0001) and greater postoperative side-to-side posterior translation (4.9 ± 4.3 mm) when compared with operative management.
Conclusion:
Although nonoperative and surgical management of PCL tibial avulsion fractures resulted in high rates of fracture union and improvement in functional outcome scores and a low incidence of complications, nonoperative treatment yielded a high side-to-side posterior displacement (>4 mm) with a lower rate of fracture union compared to surgical treatment.
The posterior cruciate ligament (PCL) is the strongest ligament of the knee, serving as the main stabilizer against posterior translation of the tibia, as well as rotational stability beyond 90° of knee flexion. 27,67 PCL injuries occur most commonly through posterior-directed forces applied to the tibia, such as motor vehicle dashboard injuries and sports-related mechanisms. 56 While the majority of PCL injuries are intrasubstance tears, a small subset of injuries involve avulsion fractures off the femoral or tibial attachment. 29
PCL avulsion fractures occur most commonly at the tibial origin via mechanisms comparable to those resulting in intrasubstance tears. 29 PCL avulsion fractures at the femoral attachment are much less common than tibial-sided avulsion fractures and have only been reported in a limited number of case reports. 20,41,45 While most avulsion fractures are isolated, Hooper et al found that 16.8% of PCL avulsion fractures involved concomitant meniscal injuries and 19.1% of patients sustained other concomitant ligamentous injuries. 21 If unrecognized or untreated, PCL avulsion fractures may lead to persistent instability and pain due to fracture malunion/nonunion. 29 Historically, open reduction and internal fixation (ORIF) has represented the gold-standard treatment due to unsatisfactory outcomes in patients undergoing nonoperative management. However, advancement in arthroscopic techniques and instrumentation have resulted in arthroscopic approaches becoming increasingly utilized, allowing for improved visualization of the avulsion fracture and treatment of concomitant injuries, despite possessing a steeper learning curve. 4,21 As such, the ideal treatment and surgical approach for PCL avulsion fractures remains controversial.
The purpose of this study was to systematically review and perform a meta-analysis evaluating outcomes and complications after management of tibial-sided PCL avulsion fractures. We hypothesized that PCL avulsion fractures treated with operative management would lead to higher rates of fracture union and improved patient outcomes when compared to patients treated nonoperatively, with no differences in outcomes between patients treated using an open versus arthroscopic approach.
Methods
Search Strategy
A systematic review was conducted in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines. 44 A literature search was conducted to identify studies reporting on patient outcomes and complications after nonoperative or surgical treatment for PCL tibial avulsion fractures by querying PubMed, Medline, Scopus, the Cochrane Database for Systematic Review, and the Cochrane Central Register for Controlled Trials databases from inception through December 15, 2022. The search included the following keywords combined with Boolean operators: “PCL”; “Posterior Cruciate Ligament”; “Avulsion”; “Fracture”; “Injury”; “Open”; “Arthroscopic”; “Screw”; “Suture”; “Fixation”; “Tibial; “Insertion”; “Outcomes”; “Approach”; “Reduction”; “Surgical”; “Operative”; “Nonoperative”; “Conservative”; and “Displaced.”
Eligibility Criteria
Inclusion criteria consisted of studies with evidence levels from 1 to 4 that were available in English and that reported patient outcomes and complications after either nonoperative or surgical treatment for PCL tibial avulsion fractures. Exclusion criteria consisted of non–English language studies, review articles, editorial commentaries, case reports, biomechanical studies, epidemiological and database studies, studies reporting on patients with PCL avulsion fractures at the femoral insertion, studies with overlapping patient datasets (study with most recent mean follow-up was retained), and studies not reporting on outcomes after management of PCL avulsion fractures.
Two authors (V.G. and F.J.C.) independently conducted an initial title and abstract screening followed by a full-text screening to determine whether studies satisfied inclusion or exclusion criteria. A third independent author (E.S.M.) was consulted to discuss and resolve any disagreements, during which time no disagreements were encountered. Reference lists from the included studies were examined to ensure that all relevant articles meeting inclusion criteria were included in this systematic review.
Data Extraction
Data were extracted from the included studies and entered into a Microsoft Excel spreadsheet (Version 2207; Microsoft). Study characteristics from each article were extracted, including level of evidence, number of patients, patient demographics (age, sex), mechanism of injury, mean follow-up, and time from injury to treatment. Intraoperative data were gathered and included surgical approach (open vs arthroscopic), fixation method, mean operative time, and mean blood loss. Preoperative and final follow-up outcome measures including Lysholm scores, subjective and objective International Knee Documentation Committee (IKDC) scores, Tegner scores, posterior drawer testing, posterior translation distance and range of motion (ROM) were recorded, as well as fracture union (confirmed by radiographs), time to union, and complications.
Data and Statistical Analysis
Weighted means of intraoperative characteristics and clinical outcomes at final follow-up were calculated for the combined population of all included patients as well as subgroup analyses based on treatment approach (open surgery vs arthroscopic surgery vs nonoperative treatment). Mean improvement calculations from preoperative to postoperative levels of the gathered clinical outcomes were inputted into random-effects models, and forest plots were produced using Open Meta-Analyst (Version 12.11.14; Tufts University). 66 When 2 or more studies included mean improvement data, subgroup analyses were performed comparing outcomes between open and arthroscopic treatment approaches. Random-effects models produced weighted means for continuous variables and weighted proportions for discrete variables. All forest plots included 95% CIs and I2 values for heterogeneity. A two-tailed Z test of proportions or t test of means was used to determine if there was any significant difference between treatment approaches. Statistical significance was set to P < .05.
Risk-of-Bias Assessment
To minimize bias, a methodological quality assessment was performed on all included studies by 2 authors (V.G. and F.J.C.) independently using the Methodological Index for Non-Randomized Studies (MINORS) criteria. Any disagreements were resolved by a third investigator (E.S.M.).
Results
The initial literature search identified 3417 articles (Figure 1). After duplicates were removed, 1036 articles remained and underwent full title and abstract screening. A total of 86 articles were then selected for full-text review. After full-text review, 58 stu meeting the eligibility criteria were identified and included in this review (Appendix Table A1).

Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) diagram. PCL, posterior cruciate ligament.
Patient Characteristics
A total of 1440 patients, 75% (1083/1440) of whom were men, were included in this systematic review and meta-analysis (Table 1). The mean patient age was 32.6 ± 5.7 years (range, 22-50.5 years). Mean patient follow-up was 26.9 ± 19.6 months (55 studies, 1406 patients; range, 5.3-126 months). Mechanisms of injury were reported in 50 studies (1186 patients), with the most common mechanisms being motor-vehicle accidents (65.1%, 773/1186 patients) followed by sports injuries (17.7%, 210/1186 patients) and falls (9.6%, 114/1186 patients). When evaluating treatment, 93% (1344/1440) of patients underwent operative management, with 63.6% (916/1440) undergoing open surgery, while 29.7% (428/1440) underwent arthroscopic surgery. Nonoperative management was performed in 6.7% (96/1440) of patients. Patients undergoing open surgery were most commonly treated using screw and washer fixation (48.2%, 405/841 patients), whereas patients who underwent arthroscopic surgery were treated most commonly using transtibial pull-out fixation (94.3%, 402/426 patients) (Table 1). All patients treated nonoperatively 3,40,64,71 underwent a period of immobilization via casting ranging from 4 weeks 64 to 8 weeks, 40 often followed by a hinged brace 3,71 and ROM exercises 64,71 until patients achieved full flexion and full weightbearing.
Patient Characteristics (N = 1440 Patients) a
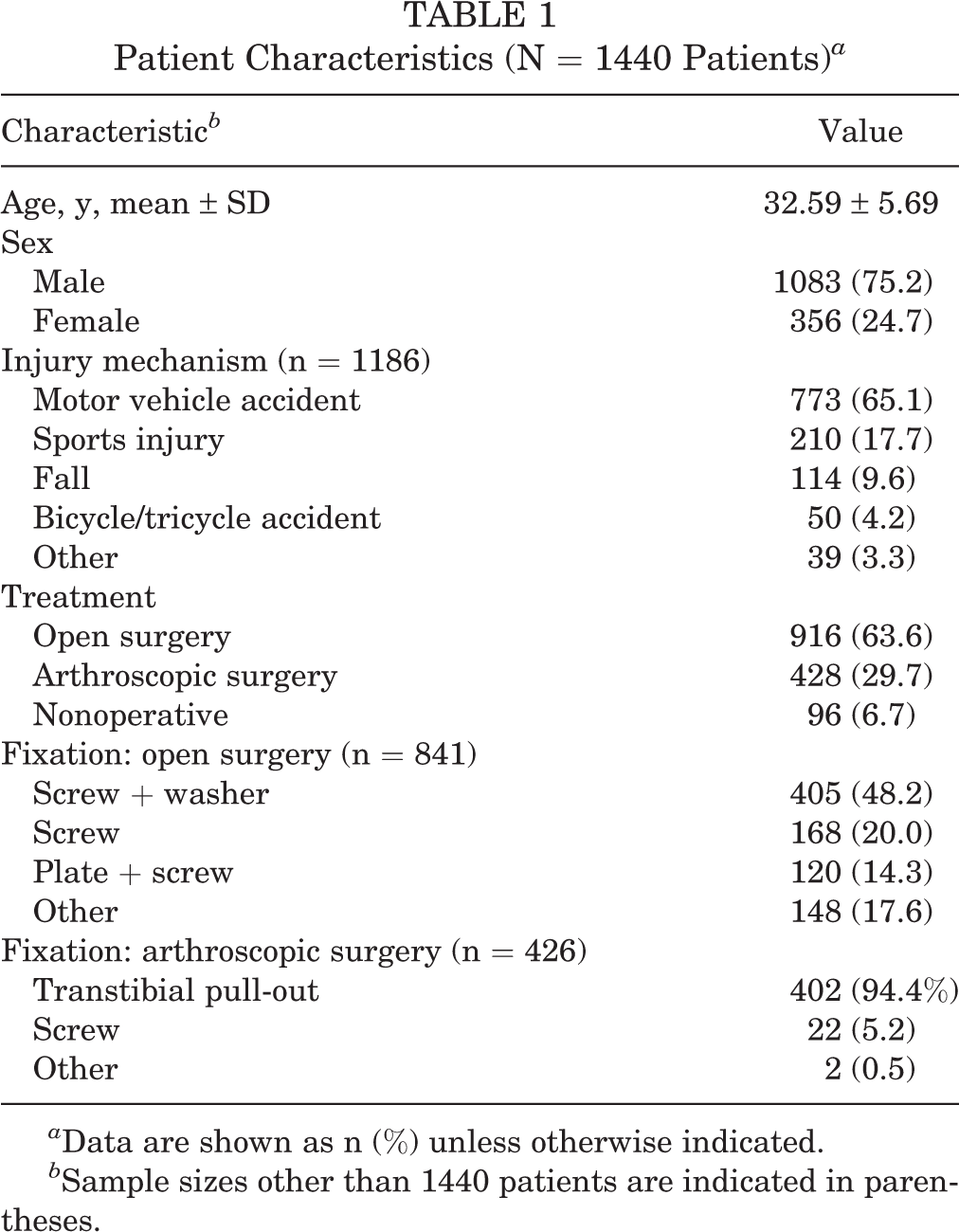
a Data are shown as n (%) unless otherwise indicated.
b Sample sizes other than 1440 patients are indicated in parentheses.
Surgery Characteristics
Operative time was reported in 27 studies, with an overall mean time of 50.1 ± 16.9 minutes (range, 22-96.8 minutes). When reported, patients undergoing an open approach (18 studies, n = 440 patients) reported a significantly lower mean operative time (46.2 ± 17.5 minutes; range, 22-96.8 minutes) when compared with patients who underwent an arthroscopic approach (9 studies, n = 180 patients; 59.7 ± 11.9 minutes; range, 35-70.5 minutes; P < .0001).
Fracture Healing Outcomes
Fracture healing assessed by radiographs was reported in 49 studies (1198 patients). The overall healing rate was 98.7% of patients (1182/1198; range, 33.3%-100%). Surgically treated PCL avulsion fractures were found to have a significantly higher fracture union rate (99.1%, 1142/1152) compared with those treated conservatively (87.0%, 40/46; P < .00001). There was no significant difference in fracture union rate in patients treated with an open approach (99.0%, 723/730) versus arthroscopic approach (99.3%, 419/422; P = .603). The mean time to achieve fracture union was 11.5 ± 4.6 weeks, reported in 20 studies (n = 450 patients). No significant difference in time to achieve fracture union was found between open (11.53 ± 5.19 weeks, 344 patients) and arthroscopic management (11.30 ± 2.87 weeks, 106 patients; P = .663).
Lysholm Score
The postoperative Lysholm score was reported in 37 studies (989 patients), with a mean score at final follow-up of 92.4 ± 5.2 (range, 81.5-97.4). Patients treated with open surgery (n = 523) reported a mean postoperative Lysholm score of 91.6 ± 4.2 (range, 81.5-95.63), whereas patients treated with arthroscopic surgery (n = 396) reported a mean score of 93.6 ± 6.6 (range, 82-97.4). Seventy patients treated nonoperatively reported a mean Lysholm score of 91.3 ± 1.63 (range, 90-92.3). Random-effects models demonstrated a 48.8-point improvement [95% CI, 37.4-60.3] from preoperative to postoperative Lysholm scores in patients undergoing open surgery (P = .724), which was significantly lower than the 54.6-point improvement (95% CI, 43.38-65.91) in patients undergoing arthroscopic surgery (P < .0001) (Figure 2).

Forest plot showing mean improvement in Lysholm scores from preoperative to postoperative levels in patients treated for posterior cruciate ligament avulsion fractures.
IKDC Score
Subjective IKDC scores were reported in 13 studies (269 patients), with a mean score at final follow-up of 87.3 ± 5.7 (range, 58.1-97.1). The mean postoperative subjective IKDC score was 86.9 ± 2.9 (range, 78.1-90.2) for patients treated with open surgery (79 patients) and 89.2 ± 4.3 (range, 58.1-97.1) for patients undergoing arthroscopic surgery (160 patients), 30 patients were treated nonoperatively. Random-effects models demonstrated a 43.7-point improvement in subjective IKDC scores from preoperative to postoperative levels, with no significant difference in patients undergoing arthroscopic surgery and open surgery (P = .774) (Figure 3). Regarding the objective IKDC of patients who underwent surgical treatment (88 patients, 3 studies), a random-effects model demonstrated that surgical treatment resulted in significantly increased odds of achieving “normal” or “near-normal” IKDC grades (defined as grades A and B, respectively) (Figure 4).
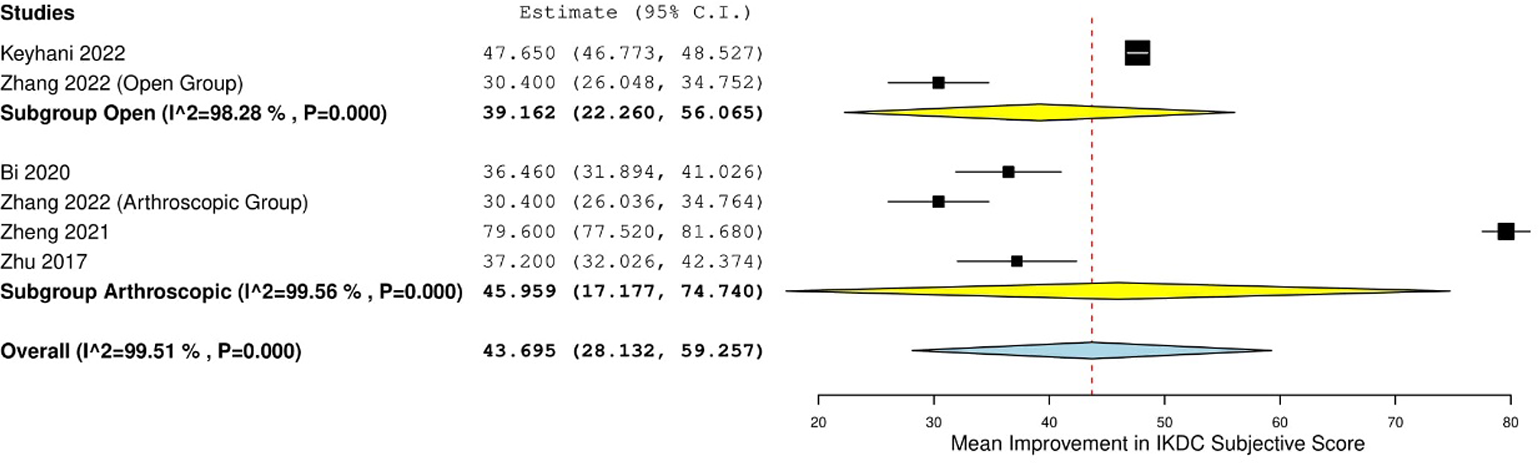
Forest plot showing mean improvement in IKDC subjective scores from preoperative to postoperative levels in patients treated for posterior cruciate ligament avulsion fractures. IKDC, International Knee Documentation Committee.

Forest plot showing risk difference in achieving “normal” (grade A) or “near-normal” (grade B) IKDC objective scores in preoperative versus postoperative levels in patients treated for posterior cruciate ligament avulsion fractures. IKDC, International Knee Documentation Committee.
Posterior Tibial Translation
Side-to-side differences in postoperative posterior tibial translation (PTT) were reported in 13 studies (296 patients). PTT was measured with a KT-1000 in 6 studies, 5,7,11,18,73,76 KT-2000 in 4 studies, 23,33,53,70 “KT-3000” in 1 study, 78 or Telos stress device in 2 studies. 52,71 For patients undergoing arthroscopic surgery (185 patients), postoperative PTT ranged from 0.6 to 3.2 mm. For patients undergoing open surgery (81 patients), postoperative PTT ranged from 1.7 to 3.1 mm. One study reported on postoperative PTT after nonoperative treatment (30 patients), with a PTT of 4.9 ± 4.3 mm. 71
Posterior Drawer
Postoperative posterior drawer examination results were reported in 34 studies comprising 804 patients. A negative or grade 1 posterior drawer was reported in 91.8% of patients (738/804) at final follow-up. Of the patients undergoing open surgery, 90.3% (438/485) reported a negative or grade 1 postoperative posterior drawer test compared with 94.0% (300/319) of patients undergoing arthroscopic surgery (P = .061). Random-effects models found a 0.887 risk difference in favor of achieving a negative or grade 1 posterior drawer test postoperatively in patients who underwent surgical treatment, with no significant difference between open and arthroscopic surgery (P = .803) (Figure 5).
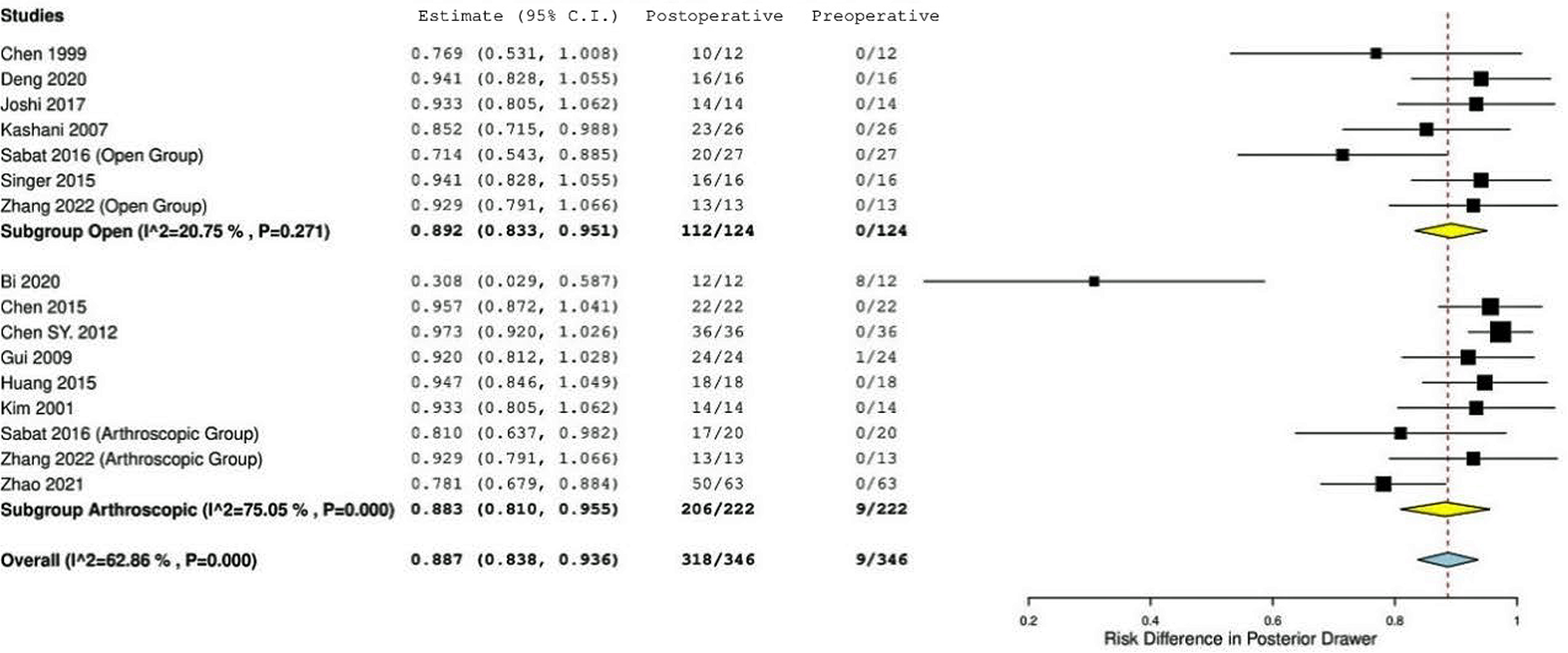
Forest plot showing risk difference in posterior drawer grades in preoperative versus postoperative levels in patients treated for posterior cruciate ligament avulsion fractures.
Range of Motion
Full knee ROM was achieved in 95.5% (557/583 patients; range, 82.6%-100%; n = 26 studies) of patients at final follow-up. There was no significant difference in the percentage of patients achieving full ROM between open surgery (96.6%, 365/378 patients; range, 82.6%-100%) and arthroscopic surgery (93.7%, 192/205 patients; range, 84.6%-100%; P = .103). Random-effects models demonstrated a mean improvement of 67.57° in ROM from preoperative to postoperative measurements, with no difference in open versus arthroscopic surgery (P = .341) (Figure 6).
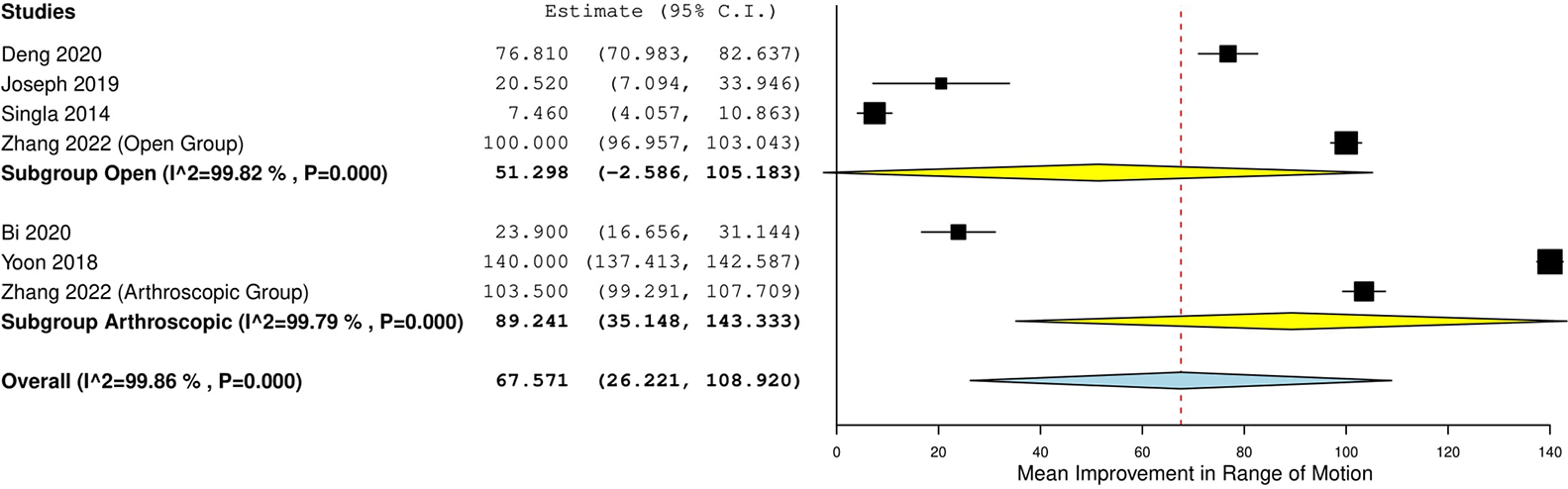
Forest plot showing mean improvement in range of motion from preoperative to postoperative in patients treated for posterior cruciate ligament avulsion fractures.
Tegner Score
Tegner scores were reported in 9 studies. At final follow-up, the mean postoperative Tegner score was 6.40 ± 1.31 (9 studies, 228 patients). The mean postoperative Tegner score was 6.14 ± 2.29 for patients undergoing open surgery (n = 34) which was significantly lower than for patients undergoing arthroscopic surgery (6.64 ± 1.03, n = 164; P = .0448). Random-effects models demonstrated a 3.93-point improvement in Tegner score from preoperative to postoperative levels (Figure 7).

Forest plot showing mean improvement in Tegner scores from preoperative to postoperative levels in patients treated for posterior cruciate ligament avulsion fractures.
Return to Preinjury Level
Return to preinjury level of activity, including daily living, work, and sport, was reported in 10 studies consisting of 256 patients undergoing surgical treatment. Moreover, 94.9% of patients (243/256) were able to return to preinjury levels. The overall return to sport (RTS) rate was 96.0% (97/101; range, 88-100%). The RTS rate for patients treated with arthroscopic surgery (100%, 63/63) was significantly higher than for patients treated with open surgery (89.5%, 34/38; range, 88.5%-91.6%; P = .009) (Figure 8). The return to work rate for patients who underwent open surgery was 87.5% (28/32; range, 81.3%-100%). There were no return to work data on patients who underwent arthroscopic surgery.

Forest plot showing return-to-sport rate in open versus arthroscopic surgical treatment for posterior cruciate ligament avulsion fractures. Ev, number of patients returning to sport; NA, not applicable; trt, total patients.
Postoperative Complications
The overall complication rate in the pooled sample was 7.3%, as reported in 50 studies (90/1225 patients; range, 0%-31.0%). There was no significant difference in complication rates for patients undergoing surgical treatment (7.2%, 83/1150 patients; range, 0%-31.0%) versus conservative treatment (7.8%, 7/90 patients; range, 5.0%-16.7%; P = .834). In addition, no significant difference was found in complication rate between open (6.8%; 49/722 patients; range, 0%-31.0%) and arthroscopic surgery (8.2%; 34/413 patients; range 0%-30.4%; P = .384). The most reported complication was motion deficit/arthrofibrosis (2.7%, 33 patients), pain and/or swelling (1.2%, 15 patients), failure (defined as incomplete reduction or significant postoperative instability [1.1%, 14 patients]), and infection (0.9%, 11 patients).
Risk-of-Bias Assessment
The mean MINORS score was 9.90 ± 4.12 (range, 6-24) (Appendix Table A2). For noncomparative studies (n = 53), the mean score was 8.39 ± 1.79 (range, 6-14), while the mean score for comparative studies (n = 9) was 18.11 ± 3.44 (range, 15-24).
Discussion
The most important finding from this study was that surgical treatment of PCL avulsion fractures achieves a high rate of fracture union with excellent restoration of posterior tibial translation. In addition, fracture union rates and side-to-side differences in PTT were improved in operative versus nonoperative management. This study suggests that displaced PCL avulsion fractures treated with open or arthroscopic surgery will lead to the best outcomes and patient satisfaction.
The high union rate of conservative treatment may be inflated due to variability in indications for surgical and conservative treatment, with numerous studies requiring at least 3 to 5 mm of displacement for surgery, 18,38,52 while conservative treatment may be suitable for nondisplaced and minimally displaced fractures. 37 Despite operative management being indicated for greater displacement, we found a significantly higher rate of fracture union for PCL avulsion fractures treated surgically (99.1%) compared with those treated conservatively (87.0%). Given that complete PCL insufficiency is defined as PTT exceeding 8 mm 57 and PCL graft failure is PTT greater than 3.6 mm, 15 operative management for PCL avulsion fractures was shown to be quite effective at reducing PTT, while similar results were not observed with conservative treatment.
Patients treated with open surgery most commonly underwent screw and washer fixation, while patients treated arthroscopically typically had a transtibial suture pull-out fixation. Several newly introduced arthroscopic fixation techniques have been introduced including a cortical button fixation with a single tibial tunnel, 63 suture bridge with double tibial tunnels, 70 and cross-linked pull-out sutures with triple tibial tunnels. 52 Further research is needed to identify the optimal fixation method from a biomechanical and clinical perspective. In addition, we found a significantly longer mean operative time for arthroscopic surgery compared with open surgery. The one randomized control trial conducted from 2015 to 2017 included in this review compared arthroscopic reduction and internal fixation (ARIF) with ORIF. 62 No differences in clinical outcomes were observed, but the ORIF group had a significantly lower cost of surgery (ORIF, US $688 ± $75.1; ARIF, US $917.7 ± $162.7) and a significantly shorter duration of surgery (ORIF, 33.4 ± 10.1 minutes; ARIF, 47.8 ± 17.9 minutes). A significant advantage of arthroscopic surgery is smaller incisions leading to faster recovery, less pain, and lower infection risk. 13,39 Recovery time was not a variable investigated given the nature of the follow-up of included studies. However, we found no difference in fracture union or complications between surgical approaches. Biomechanical studies have shown equivalent outcomes in arthroscopic suture fixation and open screw fixation for PCL avulsion fractures. 16,55 We hypothesized that although differences in posterior translation, Tegner score, and Lysholm score were noted, the marginal differences found in the meta-analysis were likely not clinically significant.
Significant improvements in Lysholm, IKDC subjective, IKDC objective, Tegner, posterior translation side-to-side difference, posterior drawer, and ROM were observed when comparing preoperative to postoperative measurements. The mean improvements exceeded the thresholds for the minimal clinically important difference for IKDC subjective score (16.7) and Lysholm score (8.9) for knee ligament injuries. 19 In addition, the mean improvement in Tegner score exceeded the minimal detectable change of 1. 19 The mean postoperative IKDC subjective score was 87.3 ± 5.7, exceeding the Patient Acceptable Symptom State of 75.9. 19
A systematic review conducted in 2017 by Hooper et al evaluated outcomes of PCL avulsion fractures from 28 articles comprising 637 patients. 21 The most significant findings were higher subjective and objective knee outcome scores, a higher return to preinjury level of activity, and slightly higher rate of arthrofibrosis in patients treated with arthroscopic surgery compared with open surgery. The present systematic review and meta-analysis (58 studies, 1440 patients) found statistically significant differences in mean improvement in Lysholm score and postoperative Tegner scores between arthroscopic and open surgery treatment groups, although likely not clinically significant. Similar to Hooper et al, we found a significantly higher return to preinjury level of activity, work, and sport in the arthroscopic group (100%) compared with the open group (89.5%). Hooper et al hypothesized this difference in return to preinjury level of activity may be due to scar formation from open surgery causing pain and impacting function in athletes. 21 Furthermore, damage to the posterior capsule after open surgery may contribute to the greater PTT compared with arthroscopic surgery. 46 Although Hooper et al reported a slightly higher rate of arthrofibrosis in patients undergoing arthroscopic surgery, we found no significant difference in complication rates between arthroscopic surgery, open surgery, or conservative treatment.
Limitations
This investigation is not without limitations. The vast majority of included studies were of level 3 and 4 evidence. Only 3 studies of level 2 evidence and 1 study of level 1 evidence were included in this review. The risk of bias assessment produced a mean MINORS score of 9.90 ± 4.12 of a possible 24 points, indicating poor quality evidence with high risk of bias. The high risk of bias limits the results of this meta-analysis given the low level of confidence that the findings of the included studies represent true treatment effects. 65 There was high heterogeneity in the number of patients, mean follow-up, time from injury to surgery, and the types of patient-reported outcome measures used. Although this investigation found no significant overall difference across most outcome measures between open and arthroscopic approaches, higher level prospective studies are needed to clarify the costs and benefits of each approach. The variable reporting of included studies makes it difficult to investigate the possible advantages of an arthroscopic approach when applied to treating PCL avulsion fractures, such as recovery time and overall patient satisfaction. Moreover, the variable reporting of concomitant injuries could greatly bias the outcome measures when comparing open and arthroscopic approaches. Given the high heterogeneity in studies and low level of evidence, it is not possible to make a clinical recommendation regarding the optimal surgical approach and fixation method.
Conclusion
Although nonoperative and surgical management of PCL tibial avulsion fractures resulted in high rates of fracture union and improvement in functional outcome scores and a low incidence of complications, nonoperative treatment yielded a high side-to-side posterior displacement (>4 mm) with a lower rate of fracture union compared to surgical treatment.
Footnotes
Final revision submitted May 5, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.R.M. has received education payments from Medwest Associates. R.H.B. has received education payments from Elite Orthopaedics. D.M.K. has received grant support from Arthrex; education payments from Smith & Nephew, Elite Orthopedics, and Medwest Associates; and hospitality payments from Stryker. R.F.L. has received consulting fees from Arthrex and Smith & Nephew, nonconsulting fees from Linvatec and Smith & Nephew, and royalties from Arthrex and Smith & Nephew. J.C. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; consulting fees from Arthrex, ConMed Linvatec, DePuy Synthes, Ossur, Smith & Nephew, Stryker, and Vericel; and speaking fees from Arthrex, Linvatec, and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.