
Abstract
Introduction:
To describe the clinical outcomes of arthroscopic fixation of displaced posterior cruciate ligament (PCL) avulsion fractures with/without associated tibia plateau fractures using an adjustable loop suspensory fixation device.
Methods:
Four male patients who have sustained PCL tibia avulsion fractures with/without associated tibia plateau fractures were operated on in a single centre using an arthroscopic adjustable loop suspensory device technique. After arthroscopic evaluation and reduction of the fracture using a probe and PCL drill guide, a proximal medial tibial mini incision was used to drill a bone tunnel through the fracture fragment. An adjustable loop suspensory device was relayed through the bone tunnel via a transtibial manner, and the button device was flipped onto the bony fragment for fixation. The associated tibial plateau fractures were then fixed if present. Knee function at the last follow-up was evaluated by International Knee Documentation Committee (IKDC), Knee Injury And Osteoarthritis Outcome Score (KOOS), Lysholm scores. Range of motion and knee stability were assessed, and fracture union was evaluated by plain radiographs.
Results:
All patients underwent the operation successfully with no major complications encountered. All were followed up for a minimum of 6 months. There was no instability reported by the patients or found during objective evaluation using posterior drawer test and reverse pivot shift test. All fractures achieved union. Mean post-operative Lysholm score was 91.5 (range 85–95), IKDC score was 85.1 (range 74.7–89.7) and KOOS was 89.3 (range 81.5–94.6). All patients returned to their pre-injury activities of daily living and work. Radiographic evaluation showed union at the fracture site in all four patients at the last follow-up.
Conclusion:
This arthroscopic procedure is a viable minimally invasive technique that is appropriate in minimally displaced avulsion fractures of the PCL with associated tibia plateau fractures.
Level of Evidence:
Case Series, IV
Introduction
Despite controversies in the treatment of posterior cruciate ligament (PCL) avulsion injuries, it is recommended that early surgical treatment of displaced bony avulsions of the PCL is necessary to restore knee stability, biomechanics 1 –4 and also to prevent the early onset of osteoarthritis. 3,4 Although conventional open surgical fixation of PCL avulsion injuries has been described with satisfactory clinical outcomes, 5,6 they carry significant surgical risk due to the proximity to complex popliteal neurovascular anatomical structures and are known to be associated with complications. 7 Minimally invasive and arthroscopic approaches have since been developed to mitigate the risks associated with open surgical approaches. 1,8 –22
Arthroscopic surgical fixation of isolated PCL avulsion fractures has been described 8,9 with limited clinical data. The technique of suspensory fixation devices has also been described to simplify the procedure. 8,10 However, to date, there has not been any clinical outcomes elaboration and validation in the use of adjustable loop suspensory fixation devices.
The syndesmotic TightRope device (Arthrex, Naples, Florida, USA) is an adjustable suspensory device that has been utilized in the treatment of ankle syndesmostic injuries, acromioclavicular joint injuries and even in patella fractures. 23 We aim to describe the clinical outcomes of this arthroscopic technique of surgical fixation using the TightRope device, as described in the study by Gwinner et al., 10 in isolated PCL avulsion fractures as well as in PCL avulsion fractures with associated tibial plateau fractures.
Materials and methods
Four consecutive patients were operated on in a single centre. The fracture patterns were confirmed by clinical evaluation as well as X-ray and CT radiological studies. Their injuries are summarized in Table 1. None of the patients had any neurological or vascular deficit at the time of initial assessment. All were closed fractures.
Patient demographics.

Surgical technique
All cases were performed under general anaesthesia, with perioperative antibiotics. Preoperative CT scans and intraoperative knee arthroscopy confirmed the existence and patterns of the intra-articular fractures.
For all cases, surgical fixation was performed under general anaesthesia with the patient supine and the affected limb hanging off the end of the table at 90°. Arthroscopic fluid delivery was via gravity-fed system. In addition to the standard anteromedial and anterolateral portals, a posteromedial portal was established as an accessory working and viewing portal. No additional posterolateral portal was required. Routine diagnostic arthroscopy using a 30° 4.0-mm arthroscope was performed to evaluate concomitant meniscal, anterior cruciate ligament (ACL) or chondral injuries. The arthroscope was advanced posteriorly between the medial femoral condyle and PCL to gain access to the fracture site and posterior compartment of the knee. The fracture was exposed by releasing some of the soft tissue remnants, fracture debris and blood clots using an arthroscopic radio frequency wand.
An arthroscopic PCL tibial drill guide (Arthrex) was passed through the anteromedial portal and used to reduce the fracture (Figure 1(a)). The reduced fracture fragment was then pinned in position using the accompanying 2.4-mm guide pin under direct arthroscopic visualization via the posteromedial portal. This was then over-reamed with a 4.5-mm reamer (Figure 1(b)). The reamer was then left in situ and the guide pin was removed (Figure 1(c)). A wire loop was then introduced through the reamer into the posterior compartment and retrieved from the anteromedial portal (Figure 1(d)). A no. 5 Ethibond suture was then shuttled through the anteromedial portal to the posterior compartment and subsequently out through the tibial drill tunnel. A syndesmotic TightRope was then modified by removing the attached needle and passing a shuttle suture through the oblong button. The Arthrex TightRope suspensory device was then relayed through the tibia tunnel utilizing the no. 5 Ethibond suture shuttle. The oblong button was then flipped onto the bony fragment under direct arthroscopic visualization (Figure 2). The TightRope button on the anteromedial tibia was then tensioned by sequentially pulling on both limbs of the TightRope device to fix the fracture in its reduced position (Figure 3(a) and (b)). The tensioning sutures were then tied with multiple half hitches to secure the TightRope fixation. In patient C, the same procedure was repeated to arthroscopically fix the posteromedial tibial plateau fragment, with the use of an arthroscopic ACL tibial drill guide. The concomitant injuries were then fixed or repaired in patients C and D. Medial collateral ligament (MCL) repair was performed in patient C, and open reduction internal fixation of lateral tibia plateau fracture was performed with a 3.5-mm proximal lateral tibia locking compression plate in patient D (Figure 4(a) to €).

Intraoperative arthroscopic image showing the (a) PCL tibial drill guide (Arthrex) used to reduce the fracture, (b) reaming of the tunnel via the drill guide pin, (c) reamer left in situ after reaming and (d)wire loop being introduced through the reamer into the posterior compartment and retrieved from the anteromedial portal. PCL: posterior cruciate ligament.
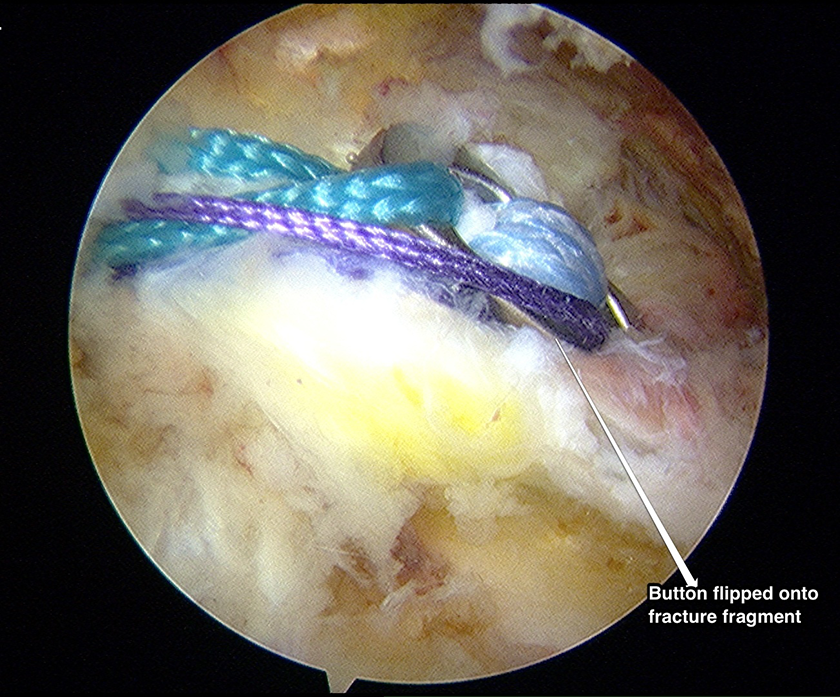
Intraoperative arthroscopic image showing the flipped oblong button onto the bony fragment.

(a and b). Intraoperative arthroscopic image showing the concomitant intra-articular tibia plateau fracture being reduced.
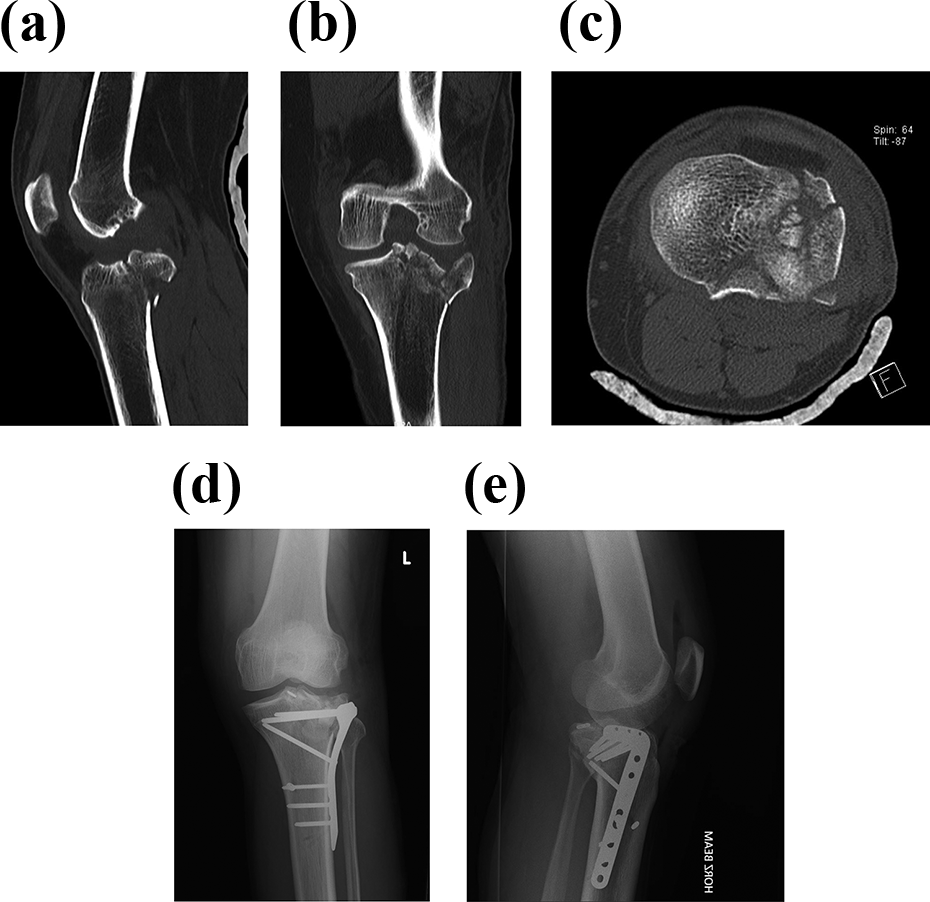
(a and e). Preoperative CT scan and post-operative radiographs after fixation of PCL avulsion and lateral tibia plateau fracture. CT: computed tomography; PCL: posterior cruciate ligament.
Post-operative rehabilitation
Protected weight bearing with a knee extension brace was started immediately post-surgery for the first 6 weeks. Isometric and subsequently closed chain knee exercises were commenced for the first 6 weeks. This was progressed to open chain knee exercises, strengthening and subsequent gradual return to activities over the next 6–9 months of rehabilitation.
Clinical evaluation
All patients were evaluated clinically at 6 weeks, 3 months, 6 months and 1 year post-operatively. An independent author who was not involved in the initial surgical management carried out the final post-operative clinical evaluation using the posterior drawer test and reverse pivot shift examination. Additionally, measurements of the knee range of motion were performed using a goniometer. The clinical assessments consisted of Lysholm, KOOS and IKDC scores.
This study was approved by the National Disease Specific Review Board.
Results
The demographics of our patient cohort are summarized in Table 1. The injury pattern and operative data are summarized in Table 2. The mean age at the time of surgery was 33.5 (range 23–42) years. The mean operative time for isolated PCL avulsion injuries was 68.5 (range 68–69) minutes. The final evaluation was performed at an average of 7.5 months (range 6–12 months) post-operatively.
Injury pattern and operative data.

PCL: posterior cruciate ligament; MCL: medial collateral ligament.
The results of the objective clinical assessments at follow-up are summarized in Table 3. At the final clinical follow-up, all patients had returned to their pre-injury activities of daily living and work. All patients achieved an operated knee range of motion similar to the contralateral knee. The mean range of motion was 132.5° (range 130–140°).
Post-operative knee ROM and stability.
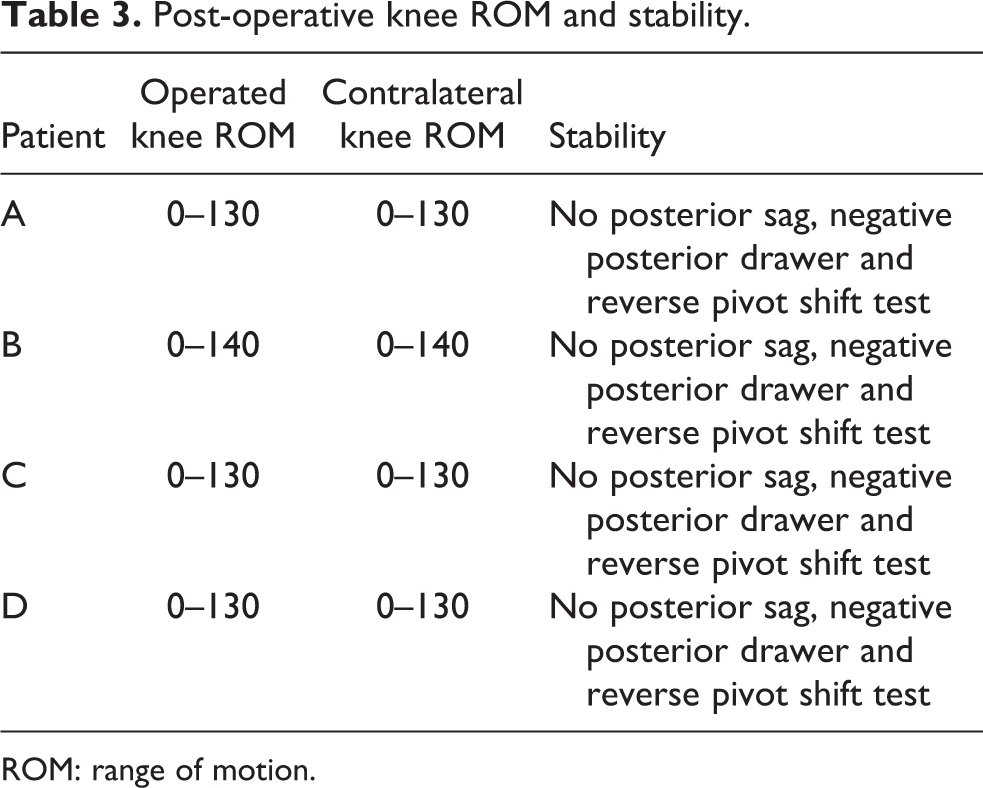
ROM: range of motion.
Posterior drawer tests and reverse pivot shift tests were negative in all patients. No posterior tibia sag was noted. None of the cases required revision surgery or encountered post-operative complications such as arthrofibrosis, loss of fixation or infection. There was no malunion or non-union in all cases.
Outcome scores
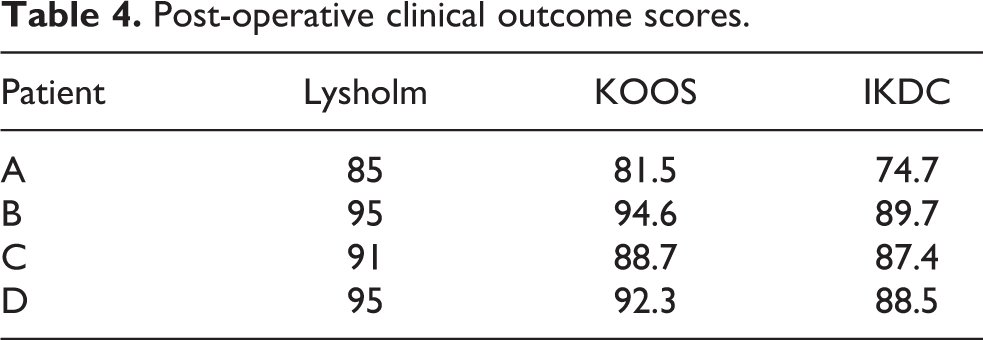
The clinical outcome scores are summarized in Table 4. Mean post-operative Lysholm score was 91.5 (range 85–95), IKDC score was 85.1 (range 74.7–89.7) and KOOS was 89.3(range 81.5–94.6).
Post-operative clinical outcome scores.
Radiological evaluation
Plain radiographs of the knee were done immediately after surgery, at 6 weeks and 6 months to verify the button position and healing progress of the fracture fragments (Figure 5(a) and (b)). All cases progressed to radiological union of the fractures. A post-operative magnetic resonance imaging (MRI) scan was performed for patient C at 6 months post-operatively because of medial-sided knee pain. The MRI scan showed synovitis under the repaired medial collateral ligament. It also showed complete fracture union as well as an intact PCL and MCL ligament repair (Figure 6(a) to (c)). The symptoms resolved at 8 months post-operatively after non-surgical management.

(a and b). Post-operative radiographs done at 6 months post-surgery.

(a and c). Post-operative MRI showing fracture union and intact PCL and MCL after PCL avulsion fracture fixation and MCL ligament repair. PCL: posterior cruciate ligament; MRI: magnetic resonance imaging; MCL: medial collateral ligament.
Discussion
There is no consensus on the optimal fixation technique for PCL avulsion fractures, with comparable results found in clinical 11 and biomechanical studies 12 comparing open screw fixation against arthroscopic suture fixation. There are no well-designed randomized comparative clinical studies to date, but satisfactory clinical outcomes have been described with both open and arthroscopic procedures. A recent systematic review involving 637 patients has however demonstrated better objective and subjective knee outcome scores in patients undergoing arthroscopic compared to open procedures. 24
Open surgical techniques require dissection through the popliteal fossa in close proximity to the neurovascular structures. Open approaches are also more invasive and require more soft tissue, muscle and posterior capsular dissection as compared to arthroscopic techniques. More aggressive soft tissue dissection in open procedures could also contribute to more scar tissue formation and arthrofibrosis, leading to decreased post-operative range of motion and function. Inadvertent division of the medial head of the gastrocnemius to improve exposure can also lead to post-operative weakness of this muscle. 6
Arthroscopic surgical techniques can also address concomitant intra-articular injuries such as meniscal tears, ACL injuries and osteochondral injuries which are frequently associated with these avulsion fractures. 13,24,25 In addition, it obviates the need for prone positioning which may be difficult in polytrauma patients.
We have shown that arthroscopic TightRope fixation is safe and reproducible with minimal morbidity. This technique allows accurate rigid anatomical fixation of the avulsed bone onto its footprint. It does not require any open approaches. TightRope can be used for fixation of medium- and large-sized PCL fragments. We would recommend caution in fixing smaller fragments with this technique as the 4.5-mm reamer may further fragment these small bony fragments, and the button may not be able to achieve adequate hold on the avulsed fragments. An alternative arthroscopic fixation utilizing sutures tied around the bone–ligament junction and passed through drillholes from the tibial footprint to the anteromedial tibia may be more appropriate in these cases. 18 Our study has shown that TightRope can also be used for rigid and secure fixation of larger tibial plateau fragments. It has also been suggested that TightRope can be used for small fragments as uniform compression can be achieved through the broad PCL tibia insertion. 8
We were able to successfully perform this procedure as early as 4 days from the time of injury. However, it should be noted that this was based on the senior author’s clinical evaluation that there was minimal capsular disruption which may prevent the adequate distension of the posterior compartment for visualization. Caution should be exercised in patients with significant soft tissue injuries as the prolonged leakage of arthroscopy fluid from the joint in a knee with significant capsular disruption may predispose to compartment syndrome in the leg.
The biomechanical properties of TightRope have been tested, and this has shown high ultimate strength, high stiffness for initial fixation and low cyclic displacement. 26 This offers advantages in the fixation of PCL avulsion fractures. The TightRope has also been shown to be biomechanically stronger than screws and sutures in the treatment of ACL avulsion fractures. 27
In addition to the current literature, we have also described the utilization of this arthroscopic technique in the fixation of a variety of tibial plateau fracture patterns. All our patients have achieved satisfactory post-operative clinical outcomes and knee stability, with the restoration of range of motion equal to the contralateral knee. All patients were able to return to their pre-injury activities of daily living and work noted at the 6-month clinical review. Despite having only a minimum of 6 months for recovery, the clinical outcome scores in our patients are comparable to other open or arthroscopic methods of fixation of these fractures. 11,14 –17,24 The commonly reported complications of arthrofibrosis and hardware irritation 1,16,17,24 were not observed in our arthroscopic study. The slightly inferior clinical outcome scores in two patients could be related to their workplace injury compensation claims.
Other arthroscopic techniques have also been described using the suture bridge method, 18 ,19 percutaneous screws, 20,21 suture anchors 22 or suture fixations. 1,14 –16 The suture bridge technique has been studied to have good clinical outcomes but has a possible steeper learning curve than the TightRope technique described in this article. In addition, as compared to just an additional posteromedial portal in our technique, the described suture bridge technique requires two additional portals (posteromedial and posterolateral), with the added risk of common peroneal nerve injury. Percutaneous screw fixation under arthroscopic control does not eliminate the risk of neurovascular injury. 20,21 Moreover, there is a high risk of bony fragment fragmentation, screw cut-out and joint penetration by the screw. 20,21
Limitations
The limitations of this study are the small number of patients and short-term follow-up. This limits the validity of the conclusions that we could make. We were also not able to perform objective side-to-side knee laxity testing as our institution does not own such an assessment device. There is likely to be some measureable objective laxity when compared to the uninjured contralateral knee as the PCL is likely to have strained or partially torn prior to avulsion of the tibial attachment. However, we were not able to note any discernible difference on clinical evaluation for PCL laxity and insufficiency. The patients in our study group were also of a younger age group, and therefore, its utility in elderly osteoporotic bone is also not known.
This small study shows that this is a simple and feasible procedure for these injuries and may form the basis of further larger studies evaluating the safety and efficacy of this procedure over other methods of fixation for minimally displaced PCL avulsion fractures. While this technique is less technically demanding and easier to perform than the other previously described arthroscopic techniques, it should still be noted that the performing surgeon should be familiar with establishing arthroscopic access to the posteromedial knee. This procedure should thus only be undertaken by surgeons who regularly scope the back of the knee and who are familiar with the instruments used for arthroscopic PCL reconstruction.
Conclusion
In the light of the findings in our study and the current literature, we believe that arthroscopic TightRope fixation is simple and feasible and should be the standard of care for management of minimally displaced avulsion fractures of the PCL, even in the presence of other pathology in the knee.
Footnotes
Authors’ note
The authors, their immediate family, and any research foundations with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. There were no prior or duplicate submission or publication elsewhere of any part of the work. The manuscript has been read and approved by all authors. Each author believes that the manuscript represents honest work. This study was approved by the National Disease Specific Review Board.
Declaration of conflicting interests
CJ Pearce is a speaker for Smith & Nephew and Depuy Synthes and is on the editorial board for KSSTA(Knee Surgery, Sports Traumatology, Arthroscopy), but speaker presentations and topics are not related/not relevant to the subject of this article. BCS Lee is a speaker for Arthrex, but speaker presentations and topics are not related/not relevant to the subject of this article. The authors declared no other potential conflicts of interest related to the subject of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.