
Abstract
Background:
Racial and ethnic disparities in the field of orthopaedic surgery have been reported extensively across many subspecialties. However, these data remain relatively sparse in orthopaedic sports medicine, especially with respect to commonly performed procedures including knee and hip arthroscopy.
Purpose:
To assess (1) differences in utilization of knee and hip arthroscopy between White, Black, Hispanic, and Asian or Pacific Islander patients in the United States (US) and (2) how these differences vary by geographical region.
Study Design:
Descriptive epidemiology study.
Methods:
The study sample was acquired from the 2019 National Ambulatory Surgery Sample database. Racial and ethnic differences in age-standardized utilization rates of hip and knee arthroscopy were calculated using survey weights and population estimates from US census data. Poisson regression was used to model age-standardized utilization rates for hip and knee arthroscopy while controlling for several demographic and clinical variables.
Results:
During the study period, rates of knee arthroscopy utilization among White patients were significantly higher than those of Black, Hispanic, and Asian or Pacific Islander patients (ie, per 100,000, White: 180.5, Black: 113.2, Hispanic: 122.2, and Asian: 58.6). Disparities were even more pronounced among patients undergoing hip arthroscopy, with White patients receiving the procedure at almost 4 to 5 times higher rates (ie, per 100,000, White: 12.6, Black: 3.2, Hispanic: 2.3, Asian or Pacific Islander: 1.8). Disparities in knee and hip arthroscopy utilization between White and non-White patients varied significantly by region, with gaps in knee arthroscopy being most pronounced in the Midwest (adjusted rate ratio, 2.0 [95% CI, 1.9-2.1]) and those in hip arthroscopy being greatest in the West (adjusted rate ratio, 5.3 [95% CI, 4.9-5.6]).
Conclusion:
Racial and ethnic disparities in the use of knee and hip arthroscopy were found across the US, with decreased rates among Black, Hispanic, and Asian or Pacific Islander patients compared with White patients. Disparities were most pronounced in the Midwest and South and greater for hip than knee arthroscopy, possibly demonstrating emerging inequality in a rapidly growing and evolving procedure across the country.
Racial and ethnic disparities in the field of orthopaedic surgery in the United States (US) have been reported extensively in many orthopaedic subspecialties. 17,31 –33,35 Minorities, including Black and Hispanic patients, have been shown to have significantly lower utilization of major orthopaedic interventions and worse perioperative outcomes after procedures such as total joint replacement and hip fracture surgery. 2,3,9,37 Several recent studies have reported that, despite several national efforts, these disparities have persisted and, in some cases, even worsened over time. 2,4,9,33,42
Unfortunately, however, data on racial and ethnic disparities in the field of arthroscopic sports medicine have remained relatively sparse. To date, there remains only single institutional and statewide data on arthroscopic surgery suggesting the existence of racial disparities on a regional scale, 7,11,14,19 with almost no nationally representative data available. Unlike other orthopaedic subspecialties, including spine, 16,28 shoulder, 5,15 and total joint arthroplasty, 2,4,33 which have leveraged large national registries and Medicare claims data, similar research in sports medicine has historically been limited by a lack of sizeable sports medicine databases until very recently. These data are especially important to determine whether restrictive patterns of access to common outpatient surgeries including hip and knee arthroscopy exist at the national level and to inform public policy and the efforts of the orthopaedic sports community to address these disparities in care.
The purposes of the current study were to assess (1) differences in the utilization of hip and knee arthroscopy between White, Black, Hispanic, and Asian or Pacific Islander patients in the US and (2) how these racial differences in utilization vary by geographical region. We hypothesized that Black and Hispanic patients would have lower utilization rates when compared with White patients, without any differences in the size of these disparities by geographical region.
Methods
Patient Population
The study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines for cross-sectional studies. This study was exempt by our institutional review board given its use of publicly available deidentified data.
We conducted a retrospective cross-sectional study using the National Ambulatory Surgery Sample (NASS) of the 2019 Healthcare Cost and Utilization Project (HCUP). 40 The NASS is a newly created (2016-2020) nationally representative sample of ambulatory surgery encounters that draws from the HCUP State Ambulatory Surgery and Services Database and State Emergency Department Database. Briefly, encounters are identified according to Current Procedural Terminology (CPT)-coded procedures requiring use of an operating room, penetration of skin, use of anesthesia, and use of sedation for pain control, accounting for over 15.7 million ambulatory surgery procedures annually. 40,41 Not only is it the largest registry of outpatient surgical procedures in the US, but, to our knowledge, it is currently the only publicly available nationally representative database of outpatient procedures from hospital-affiliated ambulatory surgery centers to include information concerning patient race and ethnicity. Missing race and ethnicity data constituted less than 1% of observations in the NASS data, and these patients were excluded from the study.
Measurements
The primary predictor variables of this study were (1) patient-reported race (White, Black, or Asian or Pacific Islander) and ethnicity (non-Hispanic vs Hispanic) as documented in the NASS dataset and (2) the US census region of the surgical center where the index procedure was performed (Northeast, Midwest, South, West). The primary outcome of the study was utilization of knee or hip arthroscopy, defined using CPT codes. Consistent with previous studies, knee arthroscopy encounters were identified using CPT codes 29866-29889 and hip arthroscopy encounters identified using CPT codes 29860-29863 and 29914-29916. 10,36
Additional patient demographics were also collected including age, sex, urban-rural classification of residence (using National Center for Health Statistics designation schema), 22 median household income quartile (based on the ZIP code of the patient’s address), insurance status, and medical comorbidities used to calculate an Elixhauser Comorbidity Index. 29 Facility characteristics including type of surgery center (ambulatory surgery center vs hospital-based), bed size (small, medium, large), ownership (public, not-for profit, for-profit), and teaching status were also collected.
Statistical Analysis
Survey weights were used to calculate nationally representative estimates of total procedure volumes by race and ethnicity. Racial and ethnic differences in age-standardized utilization rates of knee and hip arthroscopy were calculated by dividing estimates obtained from the NASS data by population estimates from US census data for each racial and ethnic group. Differences in baseline characteristics were compared using the chi-square test for categorical data. The Student t test was used for comparisons of continuous variables between 2 groups, while analysis of variance tests were used for comparing continuous variables across more than 2 groups.
Poisson regression was used to model age-standardized utilization rates for knee and hip arthroscopy with sex, race and ethnicity, census region, and Elixhauser comorbidity score as covariates. Population estimates for each subgroup were included as offset values in the regression models. Finally, an additional subanalysis was performed to evaluate temporal trends in disparities during the study period by discharge quarter (Q1-Q4) given that no additional years of data for the NASS were available. Analysis was conducted using Stata MP Version 17. Statistical significance was defined as P < .05.
Results
Patient Characteristics
The demographic characteristics of arthroscopy patients varied by race and ethnicity (Table 1). Black, Hispanic, and Asian or Pacific Islander patients were more likely than White patients to have Medicaid (21.9%, 20.7%, and 12.8%, respectively, vs 9.2% for White patients; P < .001); Black and Hispanic patients were also more likely to reside in more socioeconomically disadvantaged regions (39.5% and 28.3% residing in lowest income quartile, respectively vs 19.0% for White patients; P < .001). Geographical regions also varied by race and ethnicity, as there was a relatively high proportion of Black and Hispanic patients in the South (52.1% and 36.1%, respectively vs 33.2% White patients; P < .001), in addition to high proportions of Asian or Pacific Islander and Hispanic patients undergoing arthroscopy in the West (55.7% and 41.1%, respectively vs 18.7% White patients and 9.4% Black patients; P < .001). White patients were also more likely to be treated in smaller (30.7% vs 18.6% White vs non-White; P < .001), nonteaching facilities (38.5% vs 26.4% White vs non-White; P < .001).
Baseline Demographic Characteristics of Arthroscopy Patients by Race and Ethnicity a

a Data are represented as No. (%) unless otherwise specified. All estimates are weighted and thus represent nationally representative estimates. NCHS, National Center for Health Statistics; US, United States.
b Based on the median income of the ZIP code of the patient’s address (in 2019 US dollars): 1, <$48,000; 2, ≥$48,000 and <$61,000; 3, ≥$61,000 and <$82,000; 4, ≥$82,000.
c Based on the 2006 NCHS urban-rural classification scheme 15 : 1, large central metro; 2, large fringe metro; 3, medium metro; 4, small metro; 5, metropolitan; 6, noncore.
Utilization Rates
At the national level, utilization rates of knee arthroscopy among White patients were significantly higher than those of Black, Hispanic, and Asian or Pacific Islander patients (White: 180.5 per 100,000, Black: 113.2 per 100,000, Hispanic: 122.2 per 100,000, and Asian: 58.6 per 100,000; adjusted rate ratio [aRR] for White vs non-White across study period, 1.8 [95% CI, 1.8-1.9]; P < .001) (Figure 1A). Disparities were even more pronounced among patients undergoing hip arthroscopy, with White patients receiving the procedure at almost 4- to 5-fold higher rates (White: 12.6 per 100,000, Black: 3.2 per 100,000, Hispanic: 2.3 per 100,000, Asian or Pacific Islander: 1.8 per 100,000; aRR for White vs non-White across study period, 4.0 [95% CI, 3.8-4.3]; P < .001) (Figure 1B).

Age-standardized (A) knee arthroscopy and (B) hip arthroscopy utilization rates, by race, ethnicity, and US census region. Asian, Asian or Pacific Islander.
Significant geographical variations in utilization existed, with racial and ethnic disparities for overall arthroscopy utilization being most pronounced in the Midwest (White vs non-White aRR, 2.0 [95% CI, 1.9-2.1]; P < .001) and South (White vs non-White aRR, 1.9 [95% CI, 1.9-2.0]; P < .001). These trends differed for knee and hip arthroscopy; while disparities for knee arthroscopy were greatest in the Midwest and South (Table 2), disparities for hip arthroscopy were greatest in the West (White vs non-White aRR, 5.3 [95% CI, 4.9-5.6]; P < .001), followed by the South (White vs non-White aRR, 4.5 [95% CI, 4.2-4.8]; P < .001).
aRRs for Knee and Hip Arthroscopy Utilization Rates by Census Region a
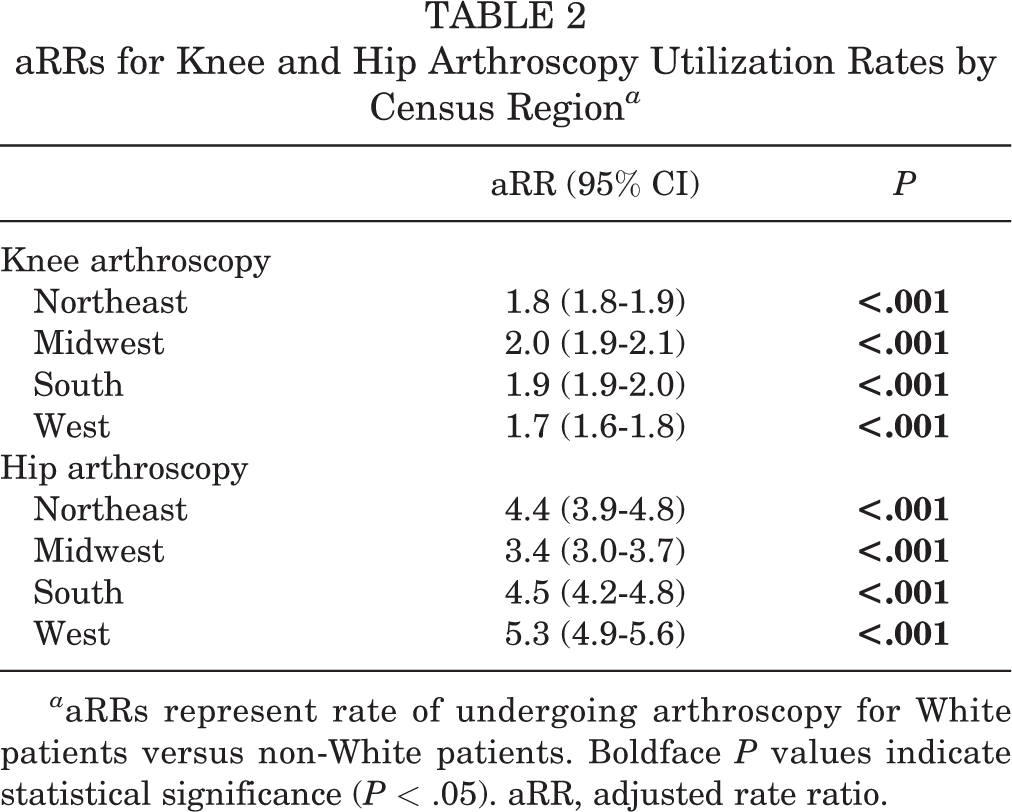
a aRRs represent rate of undergoing arthroscopy for White patients versus non-White patients. Boldface P values indicate statistical significance (P < .05). aRR, adjusted rate ratio.
Subanalysis demonstrated that, over the course of 2019, utilization of knee arthroscopy increased among all racial and ethnic subgroups (Table 3). aRRs were constant over time for knee arthroscopy, indicating a persistent disparity (aRR for White vs non-White in Q1, 2.1 [95% CI, 2.0-2.1]; aRR in Q4, 2.1 [95% CI, 2.0-2.1]; P = .9). Utilization of hip arthroscopy increased among White patients but was constant among non-White patients (Table 3). In fact, there was a widening disparity between White and Black patients in hip arthroscopy utilization over the course of 2019 (aRR for White vs Black in Q1, 3.4 [95% CI, 3.3-3.6]; aRR in Q4, 4.1 [95% CI, 3.9-4.2]; P = .032).
Temporal Trend in Knee and Hip Arthroscopy Utilization Rates by Race and Ethnicity a

a Rates are reported per 100,000 person-years. Boldface P values indicate statistical significance (P < .05). aRR, adjusted rate ratio.
Discussion
Racial and ethnic disparities in utilization and perioperative outcomes after orthopaedic surgical procedures have been well-documented; however, few studies to date have sought to characterize such differences in the sports medicine subspecialty. 7,11,14,19 In this nationwide database study evaluating differences in utilization of knee and hip arthroscopy, 2 of the most commonly performed procedures in sports medicine, 13,28 significant racial and ethnic disparities were evident. Specifically, as hypothesized, White patients were found to be 1.6 times as likely as Black patients, 1.5 times as likely as Hispanic patients, and 3.1 times as likely as Asian or Pacific Islander patients to undergo knee arthroscopy after adjusting for patient age. Differences in utilization of hip arthroscopy were even greater, with White patients undergoing surgery at rates 3.9 times higher, 5.5 times higher, and 7.0 times higher than Black, Hispanic, and Asian patients, respectively. While differences were demonstrated across the US, inequality was most marked in the Midwest and South, suggesting geographic variation in utilization patterns. As arthroscopic techniques continue to grow in popularity, early interventions by orthopaedic surgeons and policymakers alike are needed to identify and address these emerging disparities and ensure optimal and equitable care for all patients.
To our knowledge, this study is the first to assess racial and ethnic disparities in the utilization of knee and hip arthroscopy across the US. Several studies have investigated racial disparities in other orthopaedic subspecialties including spine, 16 shoulder, 5,15 and total joint arthroplasty, 2,4,33 by leveraging large national registries and Medicare claims data; however similar research in sports medicine has historically been limited by a lack of sizeable sports medicine databases. Nevertheless, studies utilizing institutional data repositories have demonstrated similar racial inequalities. 6,7,11 For example, among patients presenting to a single institution with anterior cruciate ligament (ACL) injury, Collins and colleagues found non-White patients to be significantly less likely than their White counterparts to undergo ACL reconstruction, as were those of lower versus higher socioeconomic status. 11 Black and Hispanic children have also been shown to experience greater delays to surgery after ACL rupture. 6 More recent studies examining data from statewide databases have revealed similarly decreased rates of surgical intervention for anterior glenohumeral instability and rotator cuff tear among Black and Hispanic compared with White patients. 19,39 A paucity of literature pertaining to sports medicine-related hip disabilities currently exists. Brown et al 7 determined Black patients to comprise a significantly lower proportion of patients to be evaluated by a specialist, obtain a magnetic resonance imaging scan, and ultimately be recommended for surgery. However, odds of recommendation for surgery were associated with the presence of labral tears and cam deformities, which were more common among White patients in that cohort. Results of the current study are consistent with these previous investigations of racial and ethnic disparities in sports medicine as they demonstrate decreased utilization of knee and hip arthroscopy among Black, Hispanic, and Asian or Pacific Islander patient populations. Still, future studies are needed to better characterize any underlying differences in the prevalence of knee and hip pathologies that may at least partially explain these findings.
The current study also expands on previous sports medicine literature by accessing data from the NASS, the largest all-payer ambulatory surgery database in the US, to explore racial and ethnic disparities in knee and hip arthroscopy care on the national level. 41 Notable gaps in knee and hip arthroscopy utilization were observed between White and racial and ethnic minority patients across the country, with disparities between White and non-White patients being most prominent in the Midwest and South. White patients in the Midwest underwent knee arthroscopy at higher rates than any other region, while rates of hip arthroscopy were lowest among non-White patients in the South.
Similar geographic variation in surgical utilization has been reported for a number of other orthopaedic subspecialties including spine, 43 foot and ankle, 26 and arthroplasty. 30,44 Causes of regional variability are likely multifactorial, influenced by geographic differences in access to care, 1,24 inherent physician bias, 8,18 specialty care referral patterns, sociocultural patient preferences, 20,21 insurance coverage, 6,24 and reimbursement arrangements. 38 Interestingly, Li et al 27 recently reported patients of minority race and lower socioeconomic status were more likely to undergo arthroscopic surgery at low-volume hospitals where costs of care and complication rates were relatively higher than at high-volume facilities. Although rates of utilization were not reflective of orthopaedic surgeon density, 23 they may correlate with density of orthopaedic surgeons performing arthroscopy, and regional limitations in access to high-volume facilities and surgeons with larger caseloads may contribute to differential racial and ethnic arthroscopy rates.
Numerous initiatives have been developed in response to documented disparities in orthopaedic surgery utilization and outcomes, including dedicated programs established by the National Institute of Arthritis and Musculoskeletal Skin Diseases and American Academy of Orthopaedic Surgeons. Despite increasing emphasis on cultural competency, patient education, and expanded access to care, however, recent studies have shown only modest progress in addressing racial and ethnic disparities. 2,3,37 As racial and ethnic minorities now comprise more than one-third of the US population, 25 and considering the expanding indications for and prevalence of knee and hip arthroscopy, these findings highlight the need for further focused efforts to improve access to necessary arthroscopic procedures and provide equitable sports medicine care to all patients.
Limitations
There are several important limitations to this study. First, as with any retrospective large database study, there is the possibility for selection bias, incorrect reporting of procedure codes, and poor medical record quality. Second, the NASS includes data obtained only from hospital-affiliated ambulatory surgery centers, thus facilities not affiliated with a hospital were not included in these analyses. However, as a nationwide database, findings of the current study are highly generalizable relative to smaller studies conducted at the institutional, state, and regional levels. 7,12,28,34 Third, we did not have access to data beyond 2019, which is the most recent and only year of available NASS data and thus most closely resembles current practice patterns. In addition, 2019 is the only year to include patient race and ethnicity data elements, precluding any analysis of trends in utilization beyond the calendar year. Finally, the temporal analysis of trends in hip and knee arthroscopy utilization was conducted by quarter, which may naturally fluctuate according to patient personal schedules and insurance plans. Whether such fluctuations are shared evenly by patients of different races cannot be inferred. Future studies are necessary to quantify the extent of such fluctuations and determine whether these are shared proportionally among patients of different races and ethnicities.
Conclusion
The study findings demonstrated racial and ethnic disparities in utilization of knee and hip arthroscopy are evident across the US, with decreased rates among Black, Hispanic, and Asian or Pacific Islander patients compared with White patients. Disparities in hip arthroscopy utilization were found to be more pronounced than those for knee arthroscopy, possibly demonstrating emerging inequality in a rapidly growing and evolving procedure across the country. Gaps in arthroscopy rates were greatest in the Midwest and South, indicating utilization also varies by region. Future efforts are needed to characterize the effects of these disparities on long-term outcomes as well as to identify their root causes to inform effective strategies for reducing inequality in knee and hip arthroscopy care.
Footnotes
Final revision submitted March 2, 2023; accepted April 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.N. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; consulting fees from Stryker; and hospitality payments from Medical Device Business Services, Wright Medical, and Zimmer Biomet. G.O. has received grant support from Stryker; education payments from Arthrex, Peerless Surgical, and Smith & Nephew; and hospitality payments from Exactech. R.W. has received consulting and nonconsulting fees from Arthrex, royalties from Arthrex, and hospitality payments from JRF Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.