
Abstract
Background:
Although several studies have noted that patients are routinely overprescribed opioids, few have reported usage after arthroscopic surgery.
Purpose:
To determine opioid consumption and allocation for unused opioids after common arthroscopic surgeries.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients between the ages of 15 and 40 years who were scheduled to undergo anterior cruciate ligament reconstruction (ACLR), labral repair of the hip or shoulder, meniscectomy, or meniscal repair were prospectively enrolled. Patients were prescribed either 5 mg hydrocodone-325 mg acetaminophen or 5 mg oxycodone-325 mg acetaminophen based on surgeon preference. Patients completed a daily opioid usage survey during the 2-week postoperative period. In addition, patients completed a survey on postoperative day 21 inquiring about continued opioid use and medication disposal, if applicable. Opioid medication consumption was converted to morphine milligram equivalents (MMEs).
Results:
Of the 200 patients who were enrolled in the study, 176 patients had sufficient follow-up after undergoing 85 (48%) ACLR, 26 (14.8%) hip labral repair, 34 (19.3%) shoulder labral repair, 18 (10.2%) meniscectomy, and 13 (7.4%) meniscal repair procedures. Mean age was 26.1 years (SD, 7.38); surgeons prescribed a mean of 26.6 pills whereas patients reported consuming a mean of 15.5 pills. The mean MME consumption in the 14 days after each procedure was calculated: ACLR (95.7; 44% of prescription), hip labral repair (84.8; 37%), shoulder labral repair (57.2; 35%), meniscectomy (18.4; 27%), and meniscal repair (32.1; 42%). This corresponded to approximately 39% of the total opioid prescription being utilized across all procedures. Mean MME consumption was greatest on postoperative day 1 in hip, shoulder, and meniscal procedures and on postoperative day 2 in ACLR. Only 7.04% of patients reported continued opioid use in the third postoperative week. Patients had a mean of 11 unused pills or 77.7 MMEs remaining. Of the patients with remaining medication, 24.7% intended to keep their medication for future use.
Conclusion:
The results of our study indicate that patients who undergo the aforementioned arthroscopic procedures consume <75 MMEs in the 2-week postoperative period, translating into a mean of 10 to 15 pills consumed. Approximately 60% of total opioids prescribed went unused, and one-fourth of patients intended to keep their remaining medication for future usage. We have provided general prescribing guidelines and recommend that surgeons carefully consider customizing their opioid prescriptions on the basis of procedure site to balance optimal postoperative analgesia with avoidance of dissemination of excess opioids.
Orthopaedic surgeons provide nearly 8% of all narcotic prescriptions in the United States - third among all medical specialties. 42 Over 10 million people used prescription pain medication for nonmedical purposes in 2019, 37 and opioid-based pain medications are the third-highest abused drug by Americans behind alcohol and marijuana.12,21 This causes more deaths annually than cocaine and heroin combined 18 and is also contributing to an increase in fentanyl and heroin use, which is 19 times higher among persons who have abused prescription opioids than among those who have not. 22 According to a 2012 survey, 79.5% of persons who began using heroin within the preceding year had previously abused prescription opioids. 22
Prescription opioid use is particularly concerning among teenagers and young adults, who are especially vulnerable to substance abuse and subsequent substance use disorders in adulthood.22,43 A total of 12.9% of high school seniors reported a history of nonmedical opioid use, 6 and adolescent males who participated in high-injury sports (wrestling and football) had 50% higher odds of nonmedical use of prescription opioids than adolescents who did not participate in those sports. 40 Furthermore, adolescent overdose deaths have risen exponentially since the COVID-19 pandemic, 13 and a National Surveys on Drug Use and Health study demonstrated a heroin initiation hazard 13 times higher for patients under 21 years of age with a history of nonmedical prescription opioid use compared with those without the same exposure. 7
Such trends directly impact the practice of orthopaedic sports medicine physicians, which often consists of a large proportion of adolescent and young-adult patients. In both the adult and pediatric populations, reports of opioid prescription excess of >80% have been estimated in patients recovering from various arthroscopic procedures.24,39,46 Such surplus of postoperative opioid prescription creates a conundrum, as many patients do not appropriately dispose of unused opioid pills 29 and the majority of recreational opioid users obtain these medications from friends or family. 46 This underscores the importance of safe, uniform prescription and disposal practices for these commonly used medications.
Thus, quantification of opioid consumption after common arthroscopic procedures has become a recent point of emphasis in attempts at refining prescribing practices and reducing opioid abuse. A systematic review estimated that patients consumed a mean of 273 morphine milligram equivalents (MMEs) (36 5-mg oxycodone tablets) postoperatively after arthroscopic rotator cuff repair. 11 Similar high-level studies have been performed with respect to anterior cruciate ligament reconstruction (ACLR),15,20,41 meniscal procedures,30,46 and hip arthroscopy.9,28 However, a survey of the American Academy of Orthopaedic Surgeons (AAOS) attendees highlighted many inconsistencies, and often excess, in opioid prescription patterns after common procedures, 35 and reliable, evidence-based opioid prescription recommendations after various arthroscopic procedures are sparse.27,30 The purpose of this study was to both quantify the amount of opioid prescription used after common sports medicine surgeries (meniscectomy, meniscal repair, ACLR with various graft selections, and hip and shoulder arthroscopy with labral repair) and further understand the allocation of opioid pain medications that go unused. It was our hypothesis that patients undergoing these operations would receive more opioid pills than they would utilize postoperatively and that the remaining prescription would be at risk for inappropriate disposal and potential diversion or nonmedical use. Furthermore, we believed that high school- and college-aged patients would have a greater propensity toward higher opioid usage and inappropriate disposal of postoperative opioids compared with their older counterparts.
Methods
Patients
After institutional review board approval (IRB #17D.016), a prospective observational study was conducted for patients undergoing ACLR, meniscectomy or meniscal repair, arthroscopic labral repair of the hip, or arthroscopic labral repair in the shoulder (including superior, anterior, and posterior labral repairs) at a single academic institution between June 2017 and April 2021. Patients between the ages of 15 and 40 years old were included in the study. Exclusion criteria included patients consuming opioids within 1 week before surgery or with a history of previous opioid addiction or chronic opioid use (>2 weeks), medication allergies, self-reported intolerance to nonsteroidal anti-inflammatory drugs (NSAIDs), age <15 or >40 years, a worker's compensation claim related to the injury, non-English-speaking patients, or incarceration. For patients with a labral injury of the shoulder, multidirectional instability surgery was excluded. For patients undergoing ACLR, exclusion criteria included additional ligamentous repair or reconstruction procedures, meniscal transplant, high tibial osteotomy procedures, and cartilage repair procedures other than chondroplasty. These additional procedures were perceived by the authors as potentially being more painful and not commonplace for ACLR surgery; thus, they were less representative of standard ACLR procedures. Due to the observational nature of the study without a control group, no pre hoc power analysis was performed as there was no comparison between groups. The medical record was reviewed for demographic information, including patient age at the time of surgery, sex, race and ethnicity, body mass index (BMI), type and quantity of opioid and nonopioid pain medications prescribed, graft selection for ACLR, and the use of a perioperative regional pain block and/or local anesthetic injections.
Perioperative Pain Management
Ten different fellowship-trained orthopaedic surgeons (S.H., K.B.F., J.S., W.E.) performed all procedures at 4 different outpatient surgical centers with the assistance of a fellow or resident. No modifications were made to surgeons’ intraoperative and postoperative procedures or protocols in this observational study. All patients underwent procedures under general anesthesia. Shoulder procedures were performed with the use of an interscalene block consisting of bupivacaine or liposomal bupivacaine, depending on the preferences of the anesthesia staff at the given surgical center. For ACLR procedures, the study took place during a transition period from regional anesthesia with femoral nerve catheters to adductor canal single-shot bupivacaine blocks. This transition took place early in the study period, so the majority of procedures were performed with the use of adductor canal blockade. Patients undergoing knee meniscal procedures and hip arthroscopy procedures received intra-articular marcaine. Patients were prescribed either 5 mg hydrocodone-325 mg acetaminophen, 5 mg oxycodone-325 mg acetaminophen, or 5 mg oxycodone in accordance with individual practice patterns of physicians in our group. Our institution has no formal policy for opioid prescription quantities based on age or other demographic factors. Due to the variation in preferred opioid agents among providers, all opioid pain medication dosages were converted to MMEs. MMEs were calculated for each patient using a conversion factor of 1.5 per milligram of oxycodone and oxycodone-acetaminophen and 1.0 per milligram of hydrocodone. Those patients who were not prescribed acetaminophen-containing narcotic medications were encouraged to take up to 1000 mg acetaminophen 4 times daily as needed. The majority of surgeons also prescribed 500 mg naproxen to be taken twice daily for 5 days postoperatively and 81 mg aspirin to be taken twice daily for deep vein thrombosis prophylaxis.
Opioid Usage Recording
After the surgical procedure, patients were instructed to keep a medication usage diary that tracked the daily opioid usage over the 2-week postoperative period. In this pain diary, patients were asked “How many pain pills did you take today?” Patients were reminded to fill out their pain diary by receiving a daily telephone call from a research assistant. The pain medication diary was also discussed at the first follow-up visit at 1 to 2 weeks after surgery. At postoperative day 21, patients were asked about continued opioid usage, what they planned to do with the remaining pain pills, and how long they planned to keep them if applicable (Appendix Figure A1). The primary outcomes were daily postoperative opioid consumption after the previously mentioned arthroscopic procedures. The secondary outcome was reported plans for use or disposal of unused opioids in the third postoperative week.
Statistical Analysis
To assess normality, both Shapiro-Wilk and Kolmogorov-Smirnov tests were run. However, all data were reported as means and standard deviations for consistency and ease of interpretation. Comparisons between groups were calculated using t tests or by performing analysis of variance tests for parametric continuous data of ≥3 groups. Categorical data are presented as count (%). A chi-square test or Fisher exact test was used to calculate P values for categorical data. P values <.05 were deemed significant. Subgroup analysis of opioid prescription, opioid usage, and disposal strategies was performed on patients aged ≤21 years compared with those patients aged >21 years at the time of surgery. Regression analysis was performed to assess and control for the effect of potential confounding variables such as patient age, sex, and race on opioid prescription utilization percentage and total MME utilization based on procedure. All statistical analyses were done using R Studio (Posit, PBC; Version 4.1.2).
Results
Over the course of a 4-year study period, 200 patients consented to participation and were enrolled in the study. A total of 24 patients did not meet inclusion criteria for analysis of the primary outcome due to lack of telephone call responses or incomplete pain diary recording for opioid usage assessment (Figure 1). A total of 176 patients (176/200; 88%) with a mean age of 26.1 years (SD, 7.38) underwent 85 (48.3%) ACLR procedures (including 11 hamstring tendon autografts, 2 quadriceps tendon autografts, 1 tibialis anterior allograft, 22 bone-patellar tendon-bone allografts, and 49 bone-patellar tendon-bone autografts), 34 (19.3%) arthroscopic shoulder labral repairs, 26 (14.8%) arthroscopic hip labral repairs, 18 (10.2%) meniscectomies, and 13 (7.4%) meniscal repairs. Detailed demographic data are given in Table 1.

Study flow diagram. ACLR, anterior cruciate ligament reconstruction.
Patient Demographic Information a

Data are presented as mean (SD) or patient count (percentage) for categorical data. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
Prescriptions
The most common opioids prescribed were 5 mg oxycodone-325 mg acetaminophen (47.2%; 83/176), 5 mg oxycodone (24.4%; 43/176), and 5 mg hydrocodone-325 mg acetaminophen (24.4%; 43/176). In addition to these opioids, 83.0% (146/176) of patients were prescribed an NSAID, with the most common agents being naproxen, ketorolac, or celecoxib.
Daily Opioid Usage
The mean total MME consumption in the 14 days after each procedure was calculated: ACLR (95.7 MMEs, 12.8 oxycodone tablets; 44% of prescription), hip arthroscopy (84.8 MMEs, 11.3 oxycodone tablets; 37%), shoulder arthroscopy (57.2 MMEs, 7.6 oxycodone tablets; 35%), meniscectomy (18.4 MMEs, 2.5 oxycodone tablets; 27%), and meniscal repair (32.1 MMEs, 4.3 oxycodone tablets; 42%). For patients undergoing ACLR, there was no significant difference in MMEs consumed (P = .194) or prescription utilization percentage (P = .419) between patellar tendon autograft and allograft and hamstring tendon autografts. Mean MME consumption was greatest on postoperative day 1 in the hip, shoulder, and meniscal procedures; it was greatest on postoperative day 2 in ACLR; 71% of all opioids were consumed within the first 3 days postoperatively and 63% of patients reported no opioid use by postoperative day 4. A total of 12 patients reported no opioid usage throughout the study period, whereas 5 patients requested and were given refills within the first 2 weeks postoperatively. Detailed opioid consumption data for each group is given in Figure 2.

Daily opioid consumption. Data are reported as MMEs. ACLR, anterior cruciate ligament reconstruction; MME, morphine milligram equivalent.
As opioid prescriptions varied based on procedure, the percentage of utilization was also evaluated. Detailed opioid prescription, consumption, and utilization data are given in Table 2 and Figure 3. There were no significant differences in percent utilization of prescribed opioids among ACLR (P = .961), labral repair of the hip (P = .072) and shoulder (P = .979), or meniscal procedures (P > .05) when 5 mg oxycodone-325 mg acetaminophen, 5 mg oxycodone, or 5 mg hydrocodone-325 mg acetaminophen were prescribed. Regression analysis controlling for age, BMI, and sex was performed (Tables 3 and 4) with estimates of decreased opioid utilization percentage and total MME consumption after ACLR (P = .018 and P = .025, respectively) and labral repair of the shoulder (P = .004 and P = .015, respectively) in female patients.
Opioid Prescription Utilization a

Data are presented as mean (SD) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; MME, morphine milligram equivalent.

Opioid prescription utilization. ACLR, anterior cruciate ligament reconstruction; MME, morphine milligram equivalents.
Regression Analysis of Opioid Utilization Percentage Controlling for Age, BMI, and Sex a
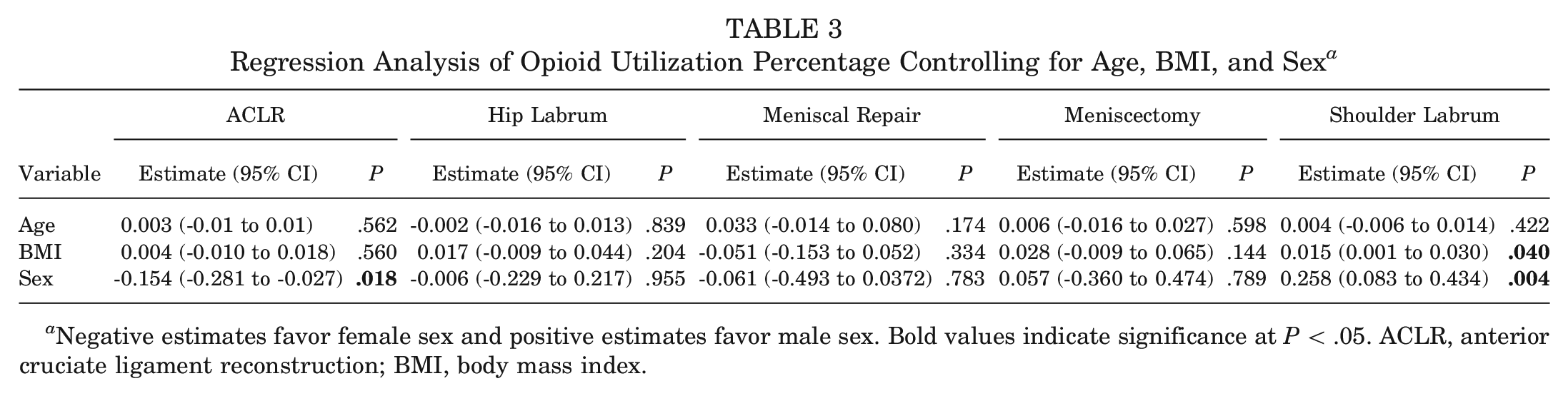
Negative estimates favor female sex and positive estimates favor male sex. Bold values indicate significance at P < .05. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
Regression Analysis of Total MME Consumption Controlling for Age, BMI, and Sex a

Negative estimates favor female sex and positive estimates favor male sex. Bold values indicate significance at P < .05. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; MME, morphine milligram equivalent.
Prolonged Opioid Use, Plans for Disposal
When surveyed on postoperative day 21 regarding opioid medication needs 3 weeks postoperatively, patients had a mean of 11 (SD, 9.36) unused pills or 77.7 MMEs (SD, 70.0 MMEs) remaining (Table 5). Only 7.04% of all patients reported continued opioid use in the third postoperative week. These patients were only those undergoing ACLR and hip and shoulder labral repair. When surveyed regarding plans for unused opioid medication, of those with remaining medication, 24.7% intended to keep their medication for future use (Figure 4). Of note, (142/200) 71.0% of the included patients were available for this survey.
Continued Opioid Use and Remaining Opioids a
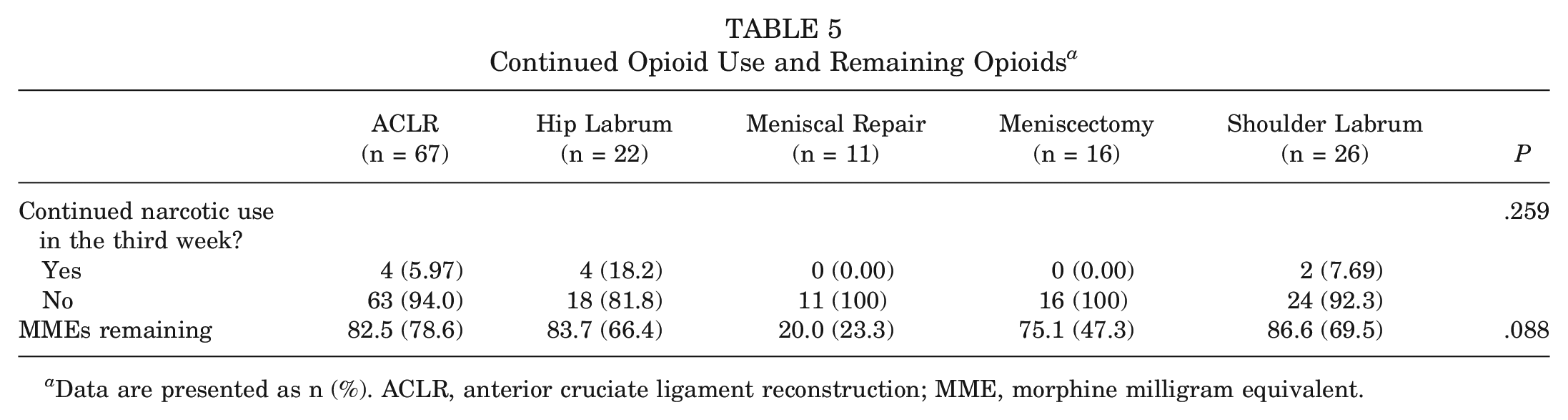
Data are presented as n (%). ACLR, anterior cruciate ligament reconstruction; MME, morphine milligram equivalent.

Plan for unused narcotics for all procedures in patients with opioids remaining.
Opioid Consumption by Age
An additional subgroup analysis was performed on opioid prescriptions, usage, and plans for opioid disposal after use based on patients >21 or
Age-Related Opioid Usage a

Data are presented as mean ± SD. MME, morphine milligram equivalent.
Discussion
Using patient-reported medication consumption data, we found that patients used only 74.1 MMEs (a mean of 15.5 narcotic-based pills pills) or 39% of the mean postoperative opioids prescribed (189 MMEs) after various arthroscopic procedures. At the third postoperative week, only 7% of patients continued to use opioids, but there were notable differences in postoperative opioid utilization among different procedures. ACLR (95.7 MMEs) as well as hip (84.8 MMEs) and shoulder labral repairs (57.2 MMEs) utilized substantially more mean MMEs relative to meniscal procedures (18.4 MMEs for meniscectomy and 32.1 MMEs for meniscal repair). Among the ACLR cohort, there was no statistically significant difference in MMEs consumed among autograft and allograft or graft donor site (hamstring vs bone-patellar tendon-bone) after ACLR. Overall, 71% of all opioids were utilized within the first 3 days postoperatively and approximately 25% of patients with unused opioid prescriptions intended to keep these medications for future use. In contrast to our initial hypothesis, patients of younger age consumed fewer opioids and were less likely to save unused opioids for future use in comparison with the older cohort. However, analysis of our prescribing patterns demonstrated that patients <21 years old were prescribed significantly fewer opioids.
The findings of the present study, in which only 39% of prescribed opioids were utilized postoperatively, with over 70% of these opioids consumed in the first 3 days after surgery, are consistent with previous literature highlighting similar trends in opioid overprescription after arthroscopic procedures. 30 Sheth et al 32 systematically reviewed 8 studies on opioid use after arthroscopic procedures, concluding that up to 60% of prescribed opioids remained unused after arthroscopic procedures of the shoulder, knee, and hip. Kamdar et al 17 demonstrated that 90% of patients undergoing meniscal procedures consumed ≤5 pills postoperatively and nearly 60% of patients did not even consume any opioids. Despite these findings, an expert panel has provided recommendations for prescription of as many as 30 opioid pills after simple knee arthroscopy, 36 and some researchers reported mean opioid prescriptions of >50 opioid pills after arthroscopic shoulder procedures before an institutional opioid-reduction initiative. 5 Fortunately, the American College of Surgeons Opioids After Surgery Workgroup has recognized these inconsistences and proposed guidelines for opioid prescriptions after common arthroscopic surgeries, 27 and legislation limiting narcotic prescription duration has been enacted on the state level. 26 As the third leading prescriber of opioids across the United States, 42 it is within the scope of the orthopaedic surgeon to combat the well-documented tendency toward opioid overprescription to positively impact opioid prescription patterns nationwide.
Not all arthroscopic procedures are created equal with respect to the degree of expected postoperative pain and opioid requirements. In this study, ACLR and hip labral repairs required a substantially larger amount of postoperative MMEs relative to shoulder labral repairs, which required significantly greater MMEs than meniscal procedures. This has been borne out in the literature14,17,29,30,32 and makes intuitive sense as more invasive procedures requiring bony manipulation should necessitate higher opioid requirements. Despite the procedural differences in postoperative opioid requirements (ie, ACLR requiring higher MMEs than diagnostic arthroscopy), the amount of opioid utilization reported after the same group of procedures (ie, shoulder arthroscopy, knee arthroscopy) is not uniform in the literature. Sheth et al 32 demonstrated that the mean MMEs consumed after hip and shoulder arthroscopy were 418 and 223 MMEs, respectively - nearly double that reported in the present study. The reason for this variation is likely 2-fold. First, Sheth et al 32 included a more heterogeneous collection of procedures including rotator cuff repairs, which have traditionally required a greater number of postoperative opioids. 44 This highlights the need for future research to clearly differentiate opioid consumption across the broad spectrum of arthroscopic procedures. More interestingly, however, it is possible that these patients utilized more opioids because they were simply provided a larger prescription (mean, 610 MMEs for hip and shoulder procedures).31,34 This discrepancy could be attributable to a phenomenon described in other orthopaedic literature in which patients after similar procedures consumed approximately 50% of prescribed medications regardless of the initial prescription amount.3,19,23 The true basis of such trends, whether it be coincidental, psychological, or multifactorial, should be recognized and is a topic that must be better understood.
Fortunately, the effect of physician prescribing patterns on opioid consumption appears to be recognized by orthopaedic surgeons, as an analysis of over 5 million Centers of Medicare and Medicaid opioid claims showed a decrease in opioid prescription rate across all orthopaedic subspecialities between 2014 and 2018. 1 In addition, rising awareness of the orthopaedist's role in combating the opioid epidemic has inspired a newfound interest in patient education with success. A randomized clinical trial by Syed et al 38 demonstrated that a preoperative opioid-related educational video alone could reduce the use of opioids after arthroscopic rotator cuff repair. Stepan et al 36 demonstrated similar results in ambulatory orthopaedic surgeries after implementation of a provider education program. Despite this progress in patient education, there still remains a dilemma for proper disposal of unused opioids as there is a well-documented link between misuse of prescription opioids and future illicit opioid abuse.22,46 Bicket et al 4 reported that 75% of unused opioids are handled improperly, and Sheth et al 32 reported that only 40% of patients receive proper disposal instructions for their unused opioids. In our study, 25% of patients reported intention to save their opioids for future use despite the Hawthorne effect and all patients being given thorough disposal instructions - substantially better than the 59% reported by Sabatino et al 29 in a similar study. This suggests that, although the orthopaedic community is making advances, efforts must even be further intensified toward education of our patients on proper handling and disposal of unused opioids.
Of patients included in this study, 37% (65/176) were <21 years old. Youth patients are believed to be at greater risk of opioid overdose and dependence due to the developmentally immature brain being unable to moderate substance use or refrain from the opioid-related rewards. 45 Misuse of prescription opioids is believed to be a leading cause of unintentional death and injury in adolescents and young adults, 16 and patients aged <21 years are felt to be at particularly high risk.8,43 Despite our hypothesis that patients of high school or college age would be more likely to improperly dispose of their unused opioids, or even consume more than their adult counterparts, the opposite was true as patients <21 years of age consumed significantly fewer opioids (52.6 vs 86.6 MMEs, P = .001) and were 48% less likely to keep their unused opioids for future use. The reasons for this were likely multifactorial. Most notably, patients <21 years old were prescribed significantly fewer opioids (157 vs 208 MMEs, P < .001) than their elder counterparts undergoing similar procedures. In addition, it is very likely that parental monitoring, awareness, and control of opioid medication administration in the younger cohort contributed to these study findings. 45 While there is a paucity of literature pertaining to adolescent opioid pain management after outpatient orthopaedic procedures, 10 this contrast in prescription pattern suggests that providers are cognizant of the dilemma and striving for responsible opioid stewardship. However, despite this initiative, 64% of the opioids prescribed to the high-risk patients <21 years old went unused, further highlighting the need for continued refinement of our opioid prescribing patterns or even opioid-free arthroscopic surgery. 25
Limitations
First, this is an observational cohort study in which patients and researchers were not blinded to the overall purpose of the study. Therefore, assessor bias is present and patients may have underutilized prescribed opioids or modified their survey responses due to the Hawthorne effect. This is a limitation of many postoperative opioid utilization studies as highlighted by Scarcella et al 30 ; however, we attempted to mitigate this bias by having all data collection and study communication be performed by members of the research team – a separate entity from the treating surgeon and care team. Second, while this study suggests that nearly 60% of postoperatively prescribed opioids go unused and previous literature demonstrates that unused opioids are commonly misused for nonmedical purposes, 22 the present study cannot demonstrate causality or definitively conclude that unused pills were used inadvertently. Third, surgeries were performed by 10 sports medicine fellowship-trained physicians (S.H., K.B.F., J.S., W.E.) and this study took place over several years. During this period, changes in regional anesthesia practices such as the transition from femoral nerve catheters to adductor canal single-shot blocks took place. Although the present study contains variation in regional anesthesia techniques as well as surgeon opioid and nonopioid medication preference, this variation inherently compromises homogeneity and challenges internal validity; however, it comes at the benefit of improved generalizability of results. Fourth, this study took place at a single academic institution across 4 surgery centers within the same geographic region and included only 1 Black patient among 176 surgical patients (0.6%), which is substantially lower than the approximately 12% of Black individuals making up the US population. Therefore, these findings may not be generalizable to the national population. In addition, the results of the present study's age-related subgroup analysis demonstrating that patients aged >21 years of age utilized higher MME prescriptions is likely influenced by numerous factors that cannot be controlled for in this study. Specifically, younger patients were provided a smaller initial opioid prescription, likely had parental oversight into their opioid use, and may have experienced more diligent opioid usage counseling from their providers due to their age and perceived increased risk of opioid misuse. Last, opioid usage rates were dependent upon patients reporting in their daily pain diary, and opioid usage was not confirmed through the use of the opioid prescription monitoring program.
Author Recommendations
The authors recommend an individualized approach toward postoperative pain management utilizing a multimodal strategy considering the surgical procedure, patient-related factors, and other medical comorbidities. Based on the present study, prescription of 20 5-mg oxycodone pills for ACLR using autograft or allograft, 18 pills for hip labral repair, 12 pills for shoulder labral repair, 9 pills for meniscal repair, and 3 pills for meniscectomy would provide sufficient quantity of opioids for >80% of patients undergoing their respective procedures. Table 7 represents our procedure-specific multimodal perioperative pain regimen based on mean MMEs consumed and consideration of the consensus guidelines suggested by the American College of Surgeons Opioids After Surgery Workgroup. 27 It should be noted that patients are encouraged to take their nonopioid pain medications on a scheduled basis, reserving opioids for use only on an as needed basis. Patients are also encouraged to contact the clinical staff if they require a prescription refill, which is honored at the discretion of the treating physician.
Recommended Postoperative Multimodal Pain Regimen a

ACLR, anterior cruciate ligament reconstruction; PO, per os/ by mouth; PRN, pro re nata/as needed.
Regarding nonopioid analgesia strategies, the majority of patients receive regional anesthesia in the form of a local infiltrative block (intra-articular injection for meniscal and hip procedures) or regional anesthesia nerve blockade in the form of an interscalene block for arthroscopic shoulder procedures or adductor canal block, often in addition to an infiltration of the interspace between the popliteal artery and capsule of the posterior knee for ACLR. All multimodal postoperative pain regimens should emphasize nonopioid analgesics, particularly acetaminophen 1000 mg per os (PO) every 6 hours as well as an NSAID such as naproxen 500 mg PO every 12 hours or ketorolac 10 mg PO every 6 hours for 5 days. 2 In addition, many providers in our practice have prioritized prescribing narcotic precriptions which do not contain acetaminophen (ie. oxycodone-acetaminophen), particularly oxycodone, so that patients may take acetaminophen on a scheduled basis and benefit from the analgesic effects of acetaminophen without necessitating opioid use.
Conclusion
The results of our study indicate that patients who undergo arthroscopic procedures consume <75 MMEs in the 2-week postoperative period, translating into a mean of 10 to 15 pills consumed. Approximately 60% of total opioids prescribed went unused, and one-fourth of patients intended to keep their remaining medication for future usage. We have provided general prescribing guidelines and recommend that surgeons carefully consider customizing their opioid prescriptions on the basis of procedure site to balance optimal postoperative analgesia with avoidance of dissemination of excess opioids.
Footnotes
Appendix Figure A1 Patient Survey in the 3rd Postoperative Week
Did you continue to take narcotic pain medication pills in the third week after surgery?
How many narcotic pain medication pills do you have remaining?___________________
If you have narcotic pills remaining, what do you plan to do with them?
Final revision submitted October 6, 2023; accepted November 16, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.B.F. has received consulting fees from Vericel, Innocoll, and Medical Device Business Services; a grant from Vericel; education payments from Liberty Surgical; nonconsulting fees from Vericel; and honoraria from Vericel. J.P.S. has received consulting fees from Stryker. S.H. has received nonconsulting fees from Arthrex; education payments from Paladin Technology Solutions and Liberty Surgical; and hospitality payments from Smith+Nephew and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University.