
Abstract
Background:
Surgeons are familiar with the complication rates and risks of knee arthroscopy, but comparative data between hip arthroscopy and knee arthroscopy are lacking.
Purpose:
To compare complications in knee arthroscopy, the most common arthroscopic procedure, with those in hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective matched-cohort study analyzing patients who received a primary hip or knee arthroscopy was performed using the PearlDiver database. A total of 19,735 patients were identified for each cohort. Systemic complications and readmissions were assessed at 3 months postoperatively. Local complications and reoperations were assessed at 6 months, 12 months, and 24 months postoperatively. All categorical variables were compared using chi-square analysis.
Results:
Hip arthroscopy had significantly higher rates of nerve injury, stiffness, heterotopic ossification, and avascular necrosis (all P < .001) than knee arthroscopy at all observed time periods postoperatively. Hip arthroscopy also had a greater rate of all local joint complications than knee arthroscopy (16.79% vs 11.80%; P < .001). Knee arthroscopy was found to have higher incidences of deep vein thrombosis (0.98% vs 0.66%; P < .001) and myocardial infarction (0.06% vs 0.00%; P < .001) as well as a higher overall systemic complication rate (3.93% vs 3.44%; P = .013). Hip arthroscopy was found to have higher rates of subsequent arthroscopy, arthroplasty, and overall reoperation when compared with knee arthroscopy (11.99% vs 14.99%; P < .001) at all time periods up to 24 months postoperatively.
Conclusion:
Although the systemic complication rate was higher in knee arthroscopy, local joint complications, reoperation, and total complication rates were higher for hip arthroscopy. Surgeons should be aware of these potential differences to best discuss and mitigate risks with this expanding patient population.
Keywords
Arthroscopic surgery is a fundamental procedure in the field of orthopaedic surgery, with more than 1 million arthroscopies performed annually in the United States alone. 5,12,14,19 Arthroscopic procedures are less invasive than open techniques and address intra-articular pathologies while minimizing soft tissue damage, postoperative pain, recovery time, infection, and arthrofibrosis. 38 However, arthroscopic surgery is not devoid of risk, with minor complication rates reported in as many as 4.7% of arthroscopic knee procedures 30 and up to 6.4% of arthroscopic hip procedures. 11,21,35,38
Knee arthroscopies account for not only the highest number of arthroscopic surgeries but also the highest volume of all orthopaedic surgeries completed in the United States. 19 While orthopaedic surgeons have routinely performed knee arthroscopies for decades, it was not until more recently that hip arthroscopies became standard practice as well. 10 Recent advancements in instrumentation and surgical techniques have led to a 365% increase of hip arthroscopy procedures from 2004 to 2009 and another 250% increase from 2007 to 2011. 23,34 In a systematic review of 92 studies consisting of more than 6000 patients, labral tears and femoroacetabular impingement (FAI) were the most common diagnoses treated with hip arthroscopy, while labral surgery with acetabuloplasty or femoral osteochondroplasty were the 2 most common procedures reported. 15
Understanding the different nuances and risk profiles for hip versus knee arthroscopy would allow surgeons to optimize patient education, safety, and outcomes. Surgeons are familiar with the complication rates and risks of knee arthroscopy, as it is so commonly performed, but comparative data are lacking between hip arthroscopy and knee arthroscopy. Therefore, the purpose of this study was to compare overall complication rates between hip and knee arthroscopy and, more specifically, systemic and local joint complication rates between the 2 procedures. We hypothesized that similar complication rates would be found between hip and knee arthroscopy; however, the types of systemic and local joint complications would differ.
Methods
Patient records were obtained from the PearlDiver software, a commercially available administrative claims database, using Current Procedural Terminology (CPT) codes and International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10) codes. This query used the M53Ortho data set, which contains the medical records of 53 million patients from 2010 to the first 3 months of 2020 from provider groups around the United States. Institutional review board approval was waived for this study, as the provided data were deidentified and compliant with the Health Insurance Portability and Accountability Act.
A retrospective cohort design was used to analyze the outcomes between patients who underwent hip arthroscopy and patients who underwent knee arthroscopy, as identified using CPT codes. Patients undergoing anterior cruciate ligament (ACL) reconstruction were excluded because of the variability in allograft donor quality and the invasive “open” nature of autograft harvesting. 33 A minimum 2-year follow-up was ensured for each patient to properly assess outcomes over this time period. The specific CPT and ICD codes used to identify the study cohorts, surgical complications, and reoperations are shown in Supplemental Tables S1 to S3, available separately.
A propensity match was performed to provide homogeneity in age, Elixhauser Comorbidity Index (ECI), sex, obesity, diabetes, and tobacco use between the hip arthroscopy and knee arthroscopy cohorts. The initial query is illustrated in the CONSORT (Consolidated Standards of Reporting Trials) diagram in Figure 1. Between 2010 and quarter 1 of 2020 in the PearlDiver M53Ortho database, 26,097 hip and 735,798 knee arthroscopies were performed. The number of knee arthroscopies was 676,155 after exclusion of ACL reconstruction. Of these totals, 19,766 hip arthroscopies and 569,085 knee arthroscopies included a 2-year follow-up. A count-based match process using sex, age, ECI, and common comorbidities yielded 2 matched cohorts containing 19,735 patients each (Figure 1). The study characteristics are reported in Table 1. The matched cohorts were proportionally identical in the demographic variables entered. Each cohort was composed of 69.16% female patients. The age composition of the cohorts was 11.43% younger than 19 years, 34.19% between 20 and 39 years, 44.36% between 40 and 59 years, and 10.03% age 60 years or older. Comorbidities were also controlled by the match, with diabetes present in 17.46% of patients in each cohort, obesity present in 25.91%, and tobacco use by 20.24%.

Flow diagram of cohort designation. ACL, anterior cruciate ligament.
Matched Cohorts and Characteristics of Patients Receiving Either Knee or Hip Arthroscopy a
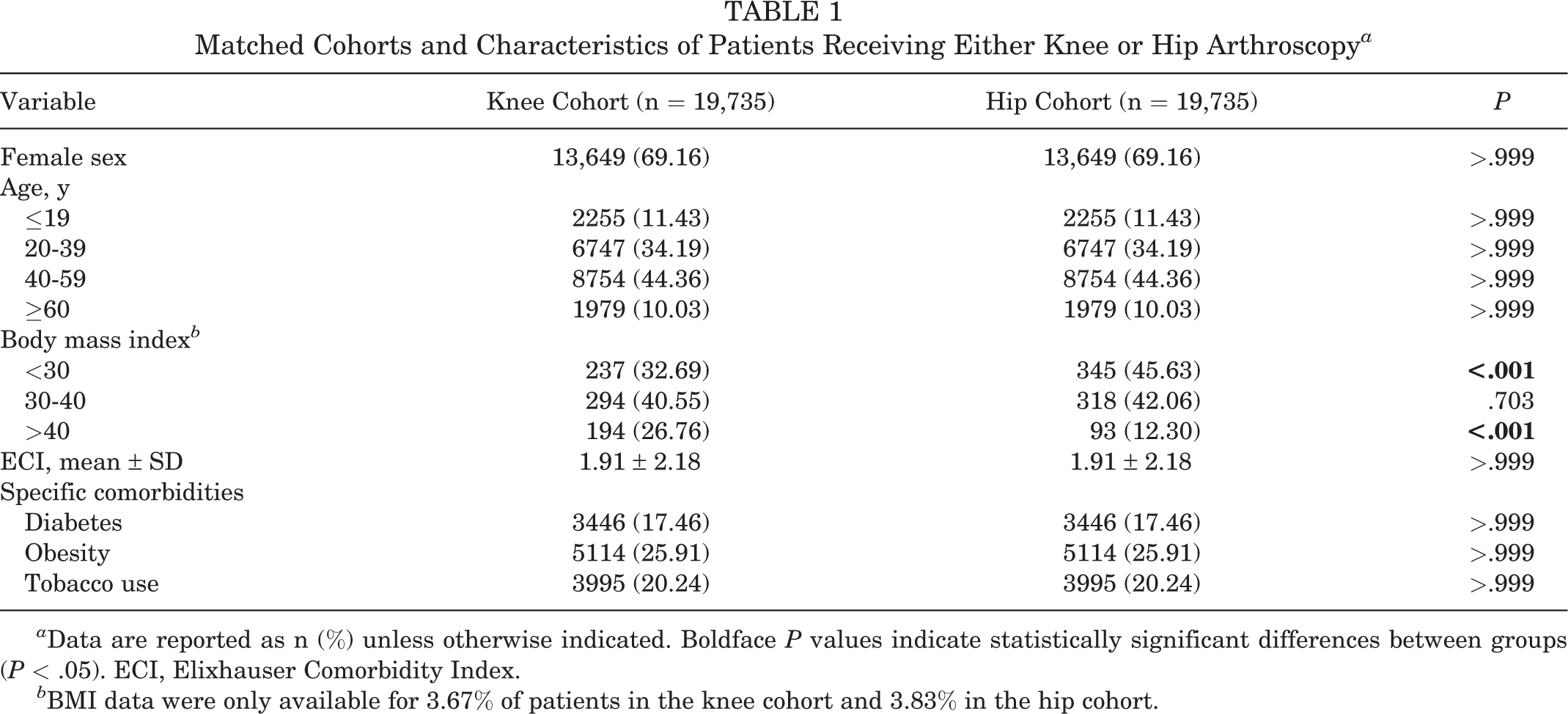
a Data are reported as n (%) unless otherwise indicated. Boldface P values indicate statistically significant differences between groups (P < .05). ECI, Elixhauser Comorbidity Index.
b BMI data were only available for 3.67% of patients in the knee cohort and 3.83% in the hip cohort.
Outcomes were assessed by observing the presence and development of postoperative complications and reoperation rates. Selected local complications included infections, nerve injury, stiffness, heterotopic ossification (HO), osteoarthritis, fracture, and avascular necrosis (AVN). Local complications around the joint were assessed at 6 months, 12 months, and 24 months after initial arthroscopy. Systemic complications included deep vein thrombosis (DVT), urinary tract infection, respiratory failure, pneumonia, cerebrovascular events, myocardial infarction (MI), acute renal failure, and pulmonary embolism. Systemic complications were assessed at 3 months after initial arthroscopy. Reoperations considered included any readmission, secondary arthroscopy, incision and drainage, and total joint arthroplasty. Readmissions were assessed only for the 3-month postoperative interval, while reoperations were assessed at 6 months, 12 months, and 24 months after initial arthroscopy.
Statistical analyses were performed using the R software integrated within PearlDiver. A level of significance was set at a value of .05. To confirm the validity of our match, the homogeneity of our continuous variables between the 2 main cohorts was ensured via Welch t tests. All categorical variables were compared using chi-square analysis.
Results
Comparative data on joint complications are reported in Table 2. Patients undergoing hip arthroscopy had a significantly greater rate of nerve injuries at 6, 12, and 24 months postoperatively (all P < .001), at 0.21%, 0.35% and 0.54%, respectively, compared with the knee cohort rates of 0.00%, 0.06%, and 0.09%, respectively. Stiffness was also significantly greater in the hip cohort at each time frame (all P < .001), with rates of 3.24%, 3.54%, and 3.99% at 6, 12, and 24 months, respectively, compared with the knee cohort at 1.83%, 2.06%, and 2.40%, respectively. A greater proportion of HO was found in the hip cohort (all P < .001), with 0.07%, 0.15%, and 0.21% at 6, 12, and 24 months, respectively, compared with no incidence at any time in the knee cohort. The hip cohort exhibited significantly greater incidence of osteoarthritis (all P < .001), with 4.54%, 6.79%, and 9.94% at 6, 12 and 24 months, respectively, compared with 3.74%, 5.74%, and 8.52%, respectively, in the knee cohort. Incidences of AVN were also greater in the hip cohort (all P < .001), with 0.51%, 0.74%, and 0.98% at 6, 12, and 24 months, respectively, compared with 0.00%, 0.06%, and 0.07%, respectively, in the knee cohort. Overall, local joint complications were significantly greater in the hip cohort than in the knee cohort (16.79% vs 11.80%; P < .001).
Local Joint Complications Between Knee Arthroscopy and Hip Arthroscopy Cohorts a
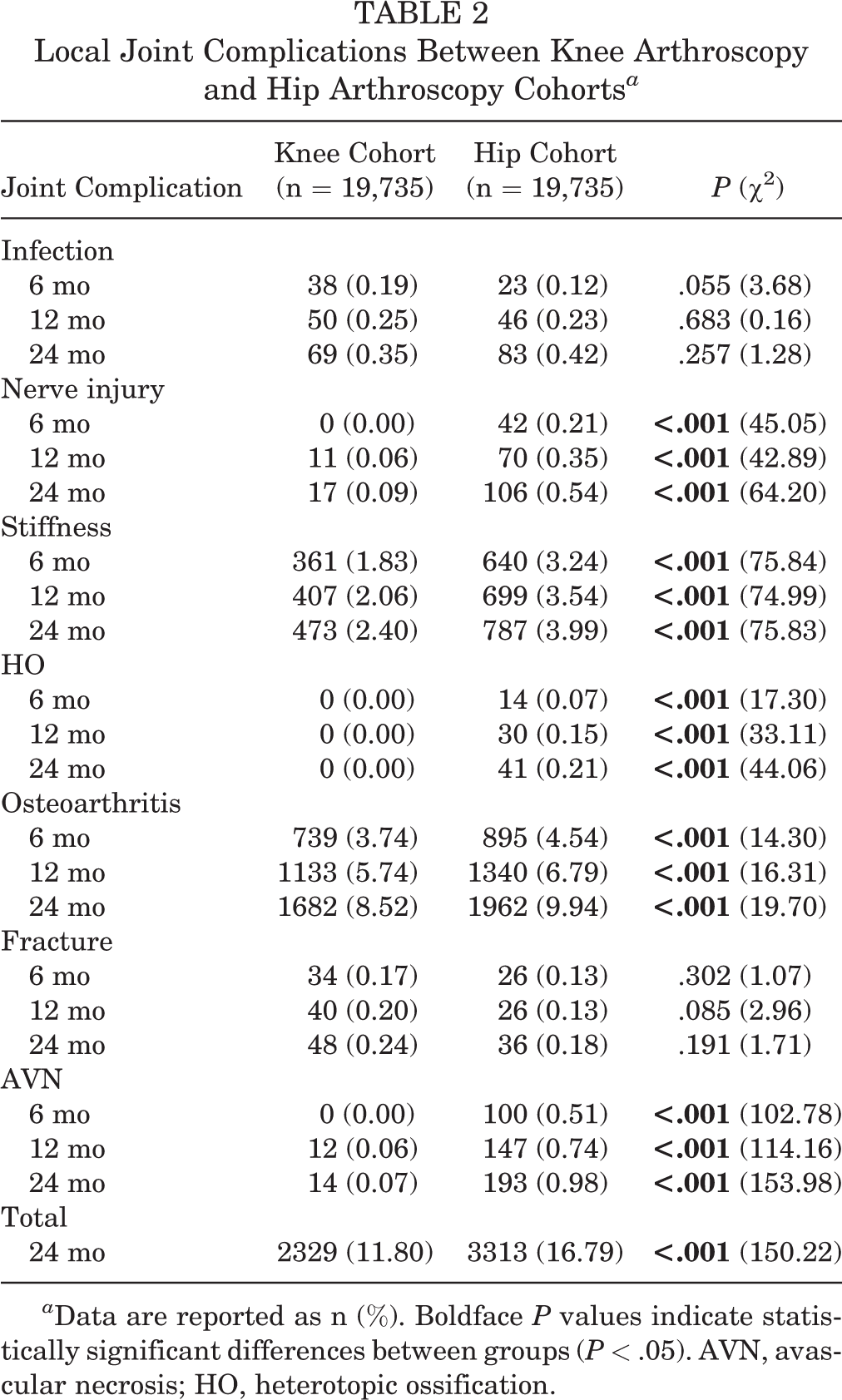
a Data are reported as n (%). Boldface P values indicate statistically significant differences between groups (P < .05). AVN, avascular necrosis; HO, heterotopic ossification.
Comparative data regarding systemic complications are reported in Table 3. Patients undergoing knee arthroscopy had significantly greater incidences of DVT (0.98% vs 0.66%; P < .001) and MI (0.06% vs 0.00%; P < .001) within 3 months than those undergoing hip arthroscopy. Overall, systemic complication rates within 3 months of surgery were greater in the knee cohort than in the hip cohort (3.93% vs 3.44%; P = .013).
Systemic Complications at 3 Months Postoperatively Between Matched Knee Arthroscopy and Hip Arthroscopy Cohorts a
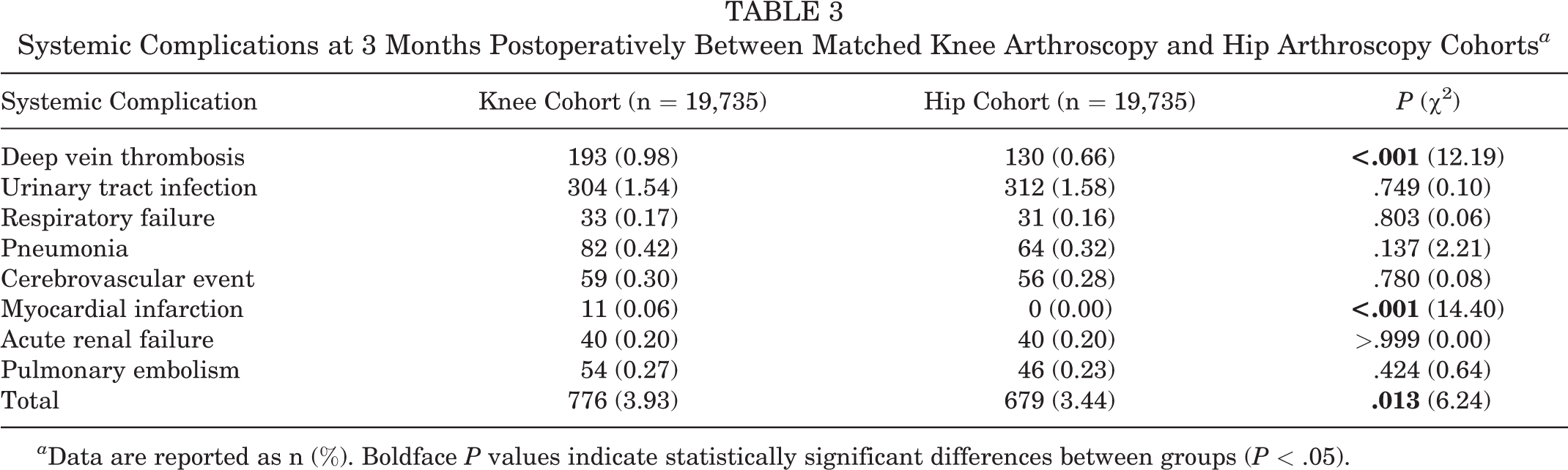
a Data are reported as n (%). Boldface P values indicate statistically significant differences between groups (P < .05).
Comparative data on readmissions and reoperations are reported in Table 4. No significant difference was found in rates of readmissions within 3 months of the discharge date. Hip arthroscopy patients underwent a significantly greater rate of subsequent arthroscopies (P < .001) and total joint arthroplasty (P < .001) at all time intervals. Conversely, knee arthroscopy patients exhibited greater rates of postoperative incision and drainage procedures at all time intervals (P = .002 at 6 months, P = .003 at 12 months, and P = .010 at 24 months). Overall, reoperation rates within 24 months of surgery were significantly greater in the hip cohort than in the knee cohort (11.99% vs 14.99%; P < .001).
Reoperation and Readmissions Between Matched Knee Arthroscopy and Hip Arthroscopy Cohorts a

a Data are reported as n (%). Boldface P values indicate statistically significant differences between groups (P < .05).
Overall complication rates (joint and systemic) are reported in Table 5. The hip cohort had a significantly higher overall complication rate than the knee cohort (15.73% vs 20.23%; P < .001).
Overall Complications Between Matched Knee Arthroscopy and Hip Arthroscopy Cohorts a
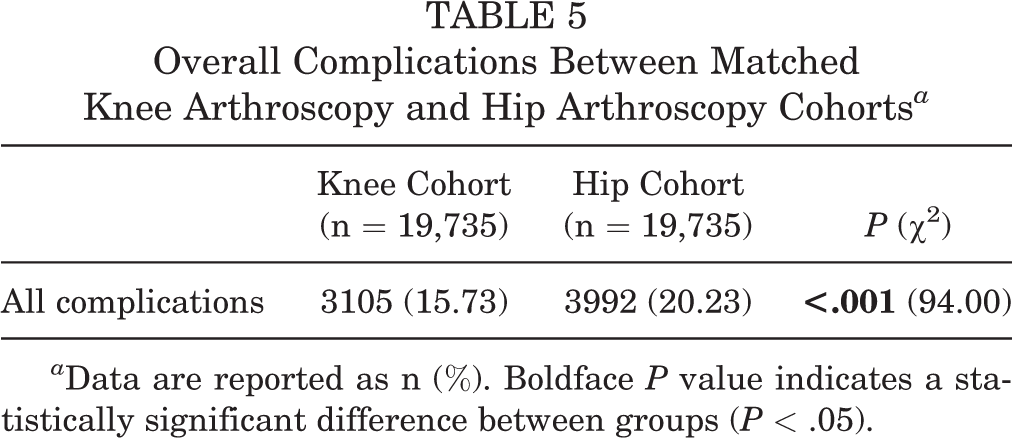
a Data are reported as n (%). Boldface P value indicates a statistically significant difference between groups (P < .05).
Discussion
The results of this study demonstrated significantly higher rates of overall systemic complications after knee arthroscopy (3.93% vs 3.44%; P = .013), while hip arthroscopy showed higher rates of local complications (16.79% vs 11.80%; P < .001). There was an increased risk of AVN, HO, stiffness, and osteoarthritis (all P < .001) in the hip cohort, as expected based on the inherent nature of the joint, 27 and a lower incidence of DVT and MI (both P < .001). In addition to complications, the hip arthroscopy cohort also had significantly higher rates of subsequent arthroplasties, total joint arthroplasties, and total reoperations (all P < .001).
Knee arthroscopy is the most common procedure performed by orthopaedic surgeons. 19 While not all knee pathology may warrant an arthroscopic procedure, patients with acute meniscal pathology or meniscal injury secondary to osteoarthritis may benefit from arthroscopy. 17,18 Additionally, knee arthroscopy has been evaluated to be beneficial in the setting of a knee presenting with mechanical blocks to motion, 18 symptomatic loose bodies, 36 synovial pathology, 3 and known or suspected septic arthritis. 16 Arthroscopy of the knee can also be instrumental in ligament reconstruction, cartilage restoration procedures, and assisting in fracture reduction. 25 Hip arthroscopy has become increasingly common and a beneficial alternative to open procedures in patients with FAI, 8 addressing labral pathology, cartilage lesions, and trochanteric pain syndrome. 4 As hip arthroscopy grows in popularity, the understanding of potential complications and differences between the procedures becomes increasingly important.
DVT after knee arthroscopy is documented in the literature at a rate of 2.0% of patients within 2 months after surgery, with the highest rates among ACL procedures. 29 This study found a DVT rate of 0.98% at 3 months after surgery, which was similar to previous studies. Comparatively, hip arthroscopy DVT incident rates have been reported at 0.76% and 1.4%, 1,13 while our study reported a rate of 0.66% at 3 months after surgery. The greater rate of DVT in knee arthroscopy may be explained by the proximity of the knee joint to the most commonly thrombosed veins, tourniquet use in knee arthroscopy, or activity levels after surgery. 24
MI after joint surgeries is known to be significantly less common in arthroscopies than in arthroplasties. 32 There is, however, a paucity of literature directly comparing cardiac incidents between hip and knee arthroscopies. While a higher rate of MI has been reported in total knee arthroplasties over hip arthroplasties, 26 this study is the first to report a significantly greater incidence of MI in knee arthroscopies compared with hip arthroscopies (P < .001). Although matching between cohorts was performed, a disparity in body mass index (BMI) proportions persisted, which may have contributed to these findings. However, these results also exhibit the overall risk of MI to be extremely low for both procedures, making clinical comparisons difficult.
Up to 10% of total hip arthroplasties in the United States are aimed at treating AVN of the hip, which develops from a decrease in femoral head perfusion by the lateral ascending branch of the medial femoral circumflex artery. 9,20,22 Paradoxically, AVN can also serve as a complication of hip arthroscopy, albeit rare. 31 The knee, in comparison, lacks this fragile localized group of vessels that it is plausible to damage during hip surgery. During this procedure, distraction of the joint and insufflation of the capsule allow for a brief disruption in perfusion of the femoral head, potentially leading to AVN. Longitudinal studies regarding length of traction and distraction time, as well as insufflation, are warranted in this rare but severe complication that was found to increase during the 2 years after index hip arthroscopy.
HO has been noted to occur in a range of 1% to 12% of patients undergoing hip arthroscopy and is 13.6 times more likely to occur without prophylaxis. 6,7,28 This study found an HO incidence rate of 0.21% in the hip arthroscopy cohort, which was significantly greater than the knee cohort (P < .001). It has been hypothesized that a higher incidence of HO in hip arthroscopies may relate to the central location of the arthroscopic portals or capsulotomy, as these are the most common locations for HO occurrence. 40 However, the hip remains the most common site of HO following spinal cord or traumatic brain injury, suggesting a complex interplay between multiple local and systemic factors that increase ossification. 37 While HO largely remains an incidental radiographic finding that does not necessitate intervention when asymptomatic, its potential impact on long-term patient outcomes should be considered alongside the increasing utilization of hip arthroscopy.
Limitations
An inherent limitation of a database claims study is human error created from medical billing code input, leading to errors within the results. However, a study from the Centers for Medicare and Medicaid Services reported that such instances make up only 1.0% of overall payments. 39 To mitigate these errors and to account for the lack of continuity in diagnosis/procedural codes during the transition from ICD-9 to ICD-10, a code translator was used to match corresponding codes. The decision to control for age, BMI, sex, ECI, tobacco use, and diabetes mellitus was made based on confounders listed as known risk factors by the American Academy of Orthopaedic Surgeons for arthroplasty infections, as these confounders have been shown to affect outcomes. 2 However, BMI was only available for a small proportion of patients and remained disparate between groups even after matching. This disparity may contribute to the increased systemic complications seen in the knee cohort. Despite matching, there remains a possibility of other confounding influences. There is also the binary presence or absence of any complication such that it is not possible to evaluate the severity of a particular complication. It is also not a direct comparison with regard to surgical exposure for hip and knee arthroscopy. Hip arthroscopies can require more extensive setup, exposure, and longer surgical times, so the length of anesthesia could be higher in this group; however, there was no increase in systemic complications in the hip cohort, suggesting the relative systemic safety of hip arthroscopy when compared with knee arthroscopy. While the presence of complications was queried such that the claim had to occur after the surgical procedure, it is impossible to determine whether some conditions, such as AVN, were present and accurately diagnosed before or during the index procedure.
Finally, as arthroscopy is a method of approach rather than an operation in and of itself, the findings present in this study are likely a result of various approaches for different operations during knee and hip arthroscopies rather than any single operation. However, given the nature of large database studies, the effects of different approaches for knee and hip arthroscopy are likely nullified by the comprehensive analyses of all the preferred approaches across the United States. While knee arthroscopy is routinely indicated and performed in active patients of all ages, hip arthroscopy tends to be limited to patients in the fifth decade and younger and thus warrants individualized analysis. Hip arthroscopy demonstrates greater complication rates at the local joint level in a matched cohort, supporting its differing safety profile when compared with the greater complication rates at the systemic level in knee arthroscopies.
Conclusion
As hip arthroscopy volume increases, understanding the safety profile is paramount to obtaining optimal outcomes. Although the systemic complication rate is higher in knee arthroscopy, local joint complication, reoperation, and total complication rates are higher for hip arthroscopy. Surgeons should be aware of these potential differences to best discuss and mitigate risks with this expanding patient population.
Supplemental Material for this article is available at http://journals.sagepub.com/doi/full/suppl/10.1177/23259671221131059#supplementary-materials.
Supplemental Material
Supplemental Material, sj-docx-1-ojs-10.1177_23259671221131059 - Local and Systemic Complications of Knee and Hip Arthroscopy: A Matched-Cohort Study
Supplemental Material, sj-docx-1-ojs-10.1177_23259671221131059 for Local and Systemic Complications of Knee and Hip Arthroscopy: A Matched-Cohort Study by William F. Sherman, Nathan P. Verzeaux, Christina Freiberger, Olivia C. Lee, J. Heath Wilder, Travis R. Flick and Wendell M.R. Heard in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted May 10, 2022; accepted August 2, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.F.S. has received honoraria from Encore Medical. W.M.R.H. has received hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived (reference No. 2021-608).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.