
Abstract
Background:
Growth disturbance to leg length or coronal plane alignment are important considerations in pediatric anterior cruciate ligament (ACL) reconstruction (ACLR).
Purpose/Hypothesis:
The purpose of this study was to investigate the lower limb alignment and leg length of pediatric patients preoperatively and at approximately 1 year after transphyseal ACLR. Our hypothesis was that there would be no significant change in leg-length discrepancy (LLD) or operated-side alignment at follow-up.
Study Design:
Case series; Level of evidence, 4.
Methods:
Data were extracted from the prospective Queensland Children’s Hospital Pediatric ACL Injury Registry. Long-leg alignment radiographs were captured preoperatively and at an approximately 12-month postoperative follow-up. Radiographic measures included leg length, LLD (injured minus uninjured leg length), mechanical axis deviation (MAD), mechanical and anatomical lateral distal femoral angle (mLDFA and aLDFA, respectively), and medial proximal tibial angle. We evaluated the effect of time (annual vs baseline) on imaging measurements with analysis of covariance, using the covariates of age, sex, and body mass index.
Results:
Data were available for 104 patients, of whom 34 (33%) had >12 months of skeletal growth remaining based on skeletal age. At an average follow-up time of 14.5 months after ACLR, there were no significant differences in mean lower limb alignment or longitudinal growth compared with baseline. However, seven patients demonstrated clinically significant changes to their mechanical axis or LLD (>10 mm change). A subgroup analysis of patients with >12 months of growth remaining (n = 34) demonstrated no statistically significant changes in mean alignment or LLD. Before surgery, LLD was -1.39 mm and the injured limb was in significantly more valgus compared with the uninjured lower limb (mean difference: MAD, 4.79 mm [95% CI, 2.64 to 6.94 mm]; mLDFA, -0.93° [95% CI, -1.29° to -0.57°], and aLDFA, -0.91° [95% CI, -1.31° to -0.50°]).
Conclusion:
After ACLR, there were no statistically significant changes in mean alignment or longitudinal growth; however, 7 out of 104 patients (6.7%) demonstrated clinically significant changes in alignment or LLD. Preoperatively, the injured limb was statistically significantly in more valgus compared with the uninjured limb with lateralized MAD.
Keywords
Although the incidence of pediatric anterior cruciate ligament (ACL) ruptures continues to increase, 24,25 there is a paucity of high-quality prospective trials comparing treatment approaches and surgical techniques. 1,19 In 2018, the International Olympic Committee (IOC) convened an expert advocate group of clinicians and released a consensus statement calling for more research into pediatric ACL injuries to evaluate long-term knee health and patient quality of life. 1 In response, the Queensland Children’s Hospital (QCH) established a prospective registry for pediatric and adolescent patients who present with ACL rupture.
Growth disturbance due to iatrogenic physeal injury is an important consideration in the surgical management of pediatric ACL injuries. 10,16 Several methods of ACL reconstruction (ACLR) have been described to minimize the likelihood of growth disturbance in skeletally immature patients 8,15,17 ; however, reports of limb alignment changes and leg-length discrepancy (LLD) due to overgrowth or undergrowth are described in all techniques. 16,21 Nonetheless, many studies that report growth disturbance are limited by sample size, radiographic field of view (ie, short-leg radiographs only) and/or by referencing postoperative imaging to typical data rather than the patient’s presurgical status. 3,5,9 Indeed, few studies have used standardized long-leg radiographs to evaluate postoperative lower limb alignment after ACLR in children and adolescents, and fewer still have compared these with preoperatively acquired long-leg radiographs. 11 Consequently, the effect of ACLR on postoperative skeletal growth remains unclear.
Taken together, the burden of pediatric ACL injuries and the paucity of high-quality prospective studies highlights the need to comprehensively evaluate radiographic parameters at multiple time points. The primary aim of this study was to determine whether growth disturbance occurred after pediatric ACLR by measuring lower limb alignment and leg length preoperatively and postoperatively. We hypothesized that there would be no significant change in LLD or alignment in the operative extremity at approximately 1 year follow-up after transphyseal ACLR.
Methods
Participant Recruitment
Institutional ethics approval for this study was received, and the guardians of all participants provided written informed consent. An a priori power analysis was conducted to determine participant numbers for this study based on a clinically significant LLD (calculated as the injured leg length minus the uninjured leg length) of >10 mm. 10 Given the pediatric cohort and the potential influences of maturation, height, and mass, we conservatively estimated the standard deviation for a change in LLD to be 15 mm. With an alpha = 0.05 and power = 0.90, the projected sample size to detect growth disturbance was 26 participants with both baseline and annual radiographs (G*Power Version 3.1.9.7).
The study participants were recruited prospectively from the QCH Pediatric ACL Injury Registry between September 2018 and December 2022. Patients were enrolled after outpatient orthopaedic consultations for their ACL injuries. Included patients were ≤16 years of age and had ACL injuries for which surgical management was indicated. Exclusion criteria included extraphyseal or partial transphyseal ACLR, previous ACLR, congenital limb abnormalities, bony or soft tissue pathology affecting anatomy (infection or trauma), bilateral ACL injuries, and neurological or musculoskeletal impairment.
All ACLR procedures were performed by fellowship-trained consultant pediatric orthopaedic surgeons (I.P.A., D.B., L.J., S.M.) . Surgical techniques of ACLR were guided by case-by-case clinical indication. When appropriate, transphyseal approaches minimized physeal damage by avoiding the femoral perichondral ring and by orienting tibial and femoral tunnels more vertically and the tibial tunnel more centrally. Graft choice and graft fixation was guided case-by-case on clinical scenarios and by surgeon preference.
Medical Image Acquisition and Measurements
Long-leg standing radiographs, lateral knee radiographs, and bone age radiographs were collected from the QCH Department of Medical Imaging and Nuclear Medicine. The alignment radiographs were collected preoperatively and at a mean of 14.5 ± 2.5 months postoperatively. Long-leg radiographs were weightbearing, digitally stitched hip-knee-ankle teleoroentgenograms. Patient positioning was standardized with forward-facing patellae and knees in full extension. Coronal measurements of alignment included leg length, mechanical axis deviation (MAD), mechanical and anatomical lateral distal femoral angle (mLDFA, aLDFA), and medial proximal tibial angle (MPTA). 20 Leg length in millimeters was calculated from the center of the femoral head to the center of the tibial plafond. For MAD, valgus was coded as positive, and varus was coded as negative (Figure 1). We defined a clinically significant growth disturbance to be a >10-mm change in MAD or LLD. Posterior tibial slope angle (PTA) was measured on lateral radiographs of the injured knee and calculated as the angle between the proximal articular surface of the tibia and a line perpendicular to the posterior cortex of the tibia. Bone age radiographs were collected at baseline and comprised left wrist radiographs or anteroposterior and lateral elbow radiographs. These were reported with the Greulich and Pyle 12 or Sauvegrain et al 22 method, respectively.
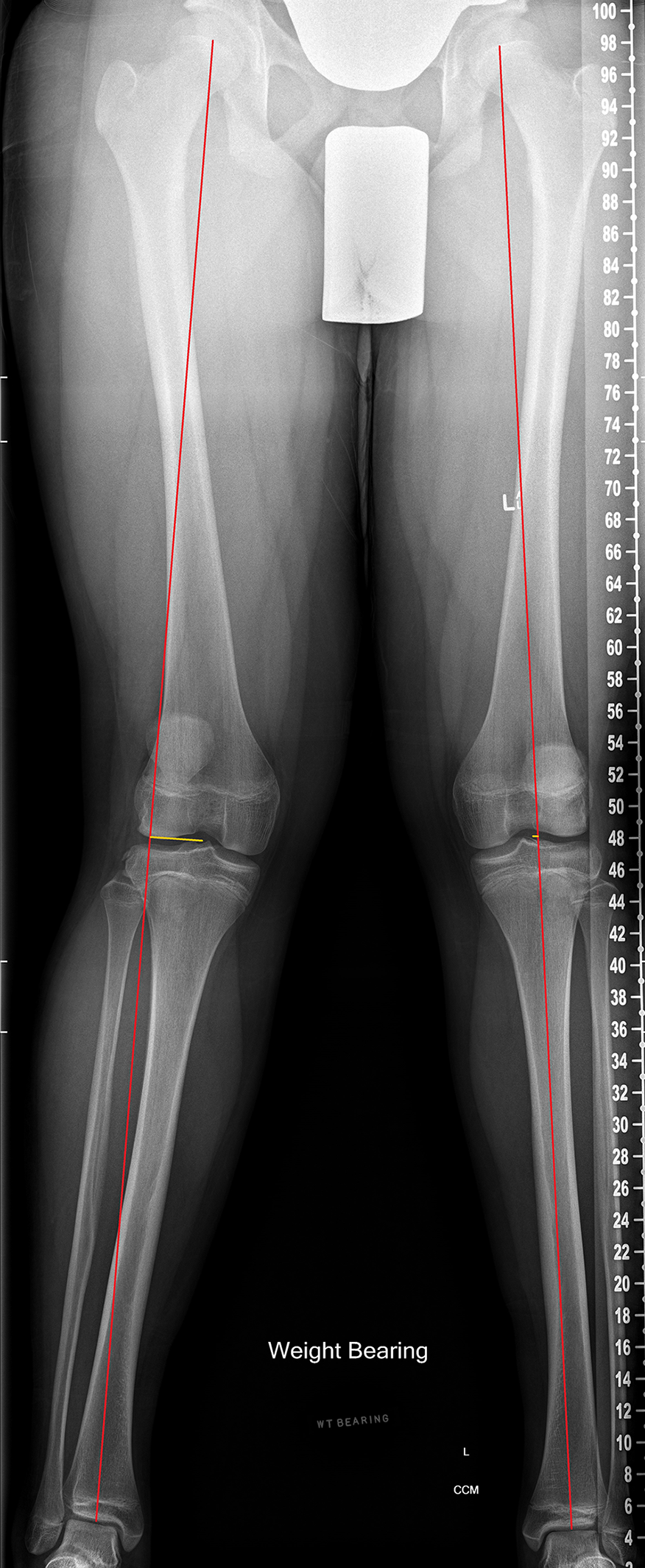
Measurement of mechanical axis deviation (MAD) in a 14-year-old male patient with right-side anterior cruciate ligament rupture. MAD, injured vs uninjured: 33.5 mm valgus vs 4.1 mm valgus. The mechanical lateral distal femoral angle, injured vs uninjured: 80.6° vs 83.9°. The anatomical lateral distal femoral angle, injured vs uninjured: 73.6° vs 74.6°.
All measurements were performed by a single author (A.H.S.), who received training from the senior author (I.P.A.). A randomly generated subset of 15 patients was measured using the same method by a fellowship-trained consultant pediatric orthopaedic surgeon (I.P.A.) to ensure interrater reliability was acceptable. To evaluate intrarater reliability, the primary measurer (A.H.S.) repeated measurements on the same 15 patients two weeks after initial data collection.
Statistical Analysis
Normality was assessed using the Shapiro-Wilk method. Continuous data were recorded as mean and standard deviation if parametric or as median and interquartile range if nonparametric. Categorical variables were recorded as frequency and percentage. We evaluated the effect of time (annual vs baseline) on imaging measurements with analysis of covariance (ANCOVA) using the covariates of age, sex, and body mass index (BMI). A further ANCOVA was conducted to assess the effect of group (injured vs uninjured limb) on imaging measurements, using the same covariates of age, sex, and BMI. Compared with predefined radiographic reference ranges, the mean difference was calculated using single-sample t test. 20
A subgroup of patients with >12 months of growth remaining based on their skeletal age was defined to ensure overall results were not confounded by patients who were nearing physeal closure. The subgroup consisted of female and male patients with a skeletal age of <13 and <15 years, respectively, as determined by the Greulich and Pyle 12 or Sauvegrain et al 22 method. The imaging measurements were compared between baseline and annual time points as well as between limbs at baseline.
Intrarater and interrater reliability (2-way random with absolute agreement) were calculated using intraclass correlation coefficients (ICCs) and were interpreted in accordance with the method outlined by Koo and Li. 18 Statistical analyses were performed using SPSS (Version 25; IBM Corp) using 2-sided statistical tests with significance set at P < .05.
Results
Patients who underwent transphyseal ACLR (N = 104) had a mean age of 13.77 ± 2.18 years (male patients: 13.60 ± 2.30 years, female patients: 14.06 ± 1.97 years) and BMI of 23.61 ± 4.94 (Table 1). A total of 34 patients had >12 months of skeletal growth remaining (33%). Baseline radiographs were captured at a median of 61 days postinjury, for which LLD was -1.39 mm. Median time from injury to surgery was approximately 122 days. Mean follow-up time was 14.5 ± 2.5 months.
Baseline Participant Characteristics a

a Data are reported as n (%) or mean ± SD unless otherwise indicated. BMI, body mass index; LLD, leg-length discrepancy.
b LLD was calculated as injured limb – uninjured limb.
All measures from the randomly generated subset of 15 patients showed good-to-excellent interrater ICCs: leg length, 1.000 (95% CI, 0.997-1.000); MAD, 0.995 (95% CI, 0.980-0.998); mLDFA, 0.925 (95% CI, 0.826-0.967); aLDFA, 0.831 (95% CI, 0.183-0.946); MPTA, 0.946 (95% CI, 0.835-0.979); and PTA, 0.823 (95% CI, 0.547-0.930). Excellent ICCs were observed for intrarater reliability: leg length, 1.000 (95% CI, 0.998-1.000); MAD, 0.998 (95% CI, 0.994-0.999); mLDFA, 0.964 (95% CI, 0.911-0.986); aLDFA, 0.953 (95% CI, 0.883-0.981); MPTA, 0.983 (95% CI, 0.957-0.993); and PTA, 0.955 (95% CI, 0.869-0.985).
Growth Disturbance Resulting in LLD or Change in Alignment
After adjustment for covariates, there were no statistically significant differences in mean lower limb alignment compared with baseline, with the exception of aLDFA on the uninjured limb (Table 2). There was a statistically significant overgrowth in the injured limb postsurgery (change in LLD of 1.79 mm). Two patients had a >10-mm change in LLD and five had a >10-mm change in MAD post-ACLR. Of these seven patients, three had >12 months of skeletal growth remaining, whereas four had <12 months of growth remaining.
Comparison of Baseline and Annual Alignment in All Patients (n = 104) a
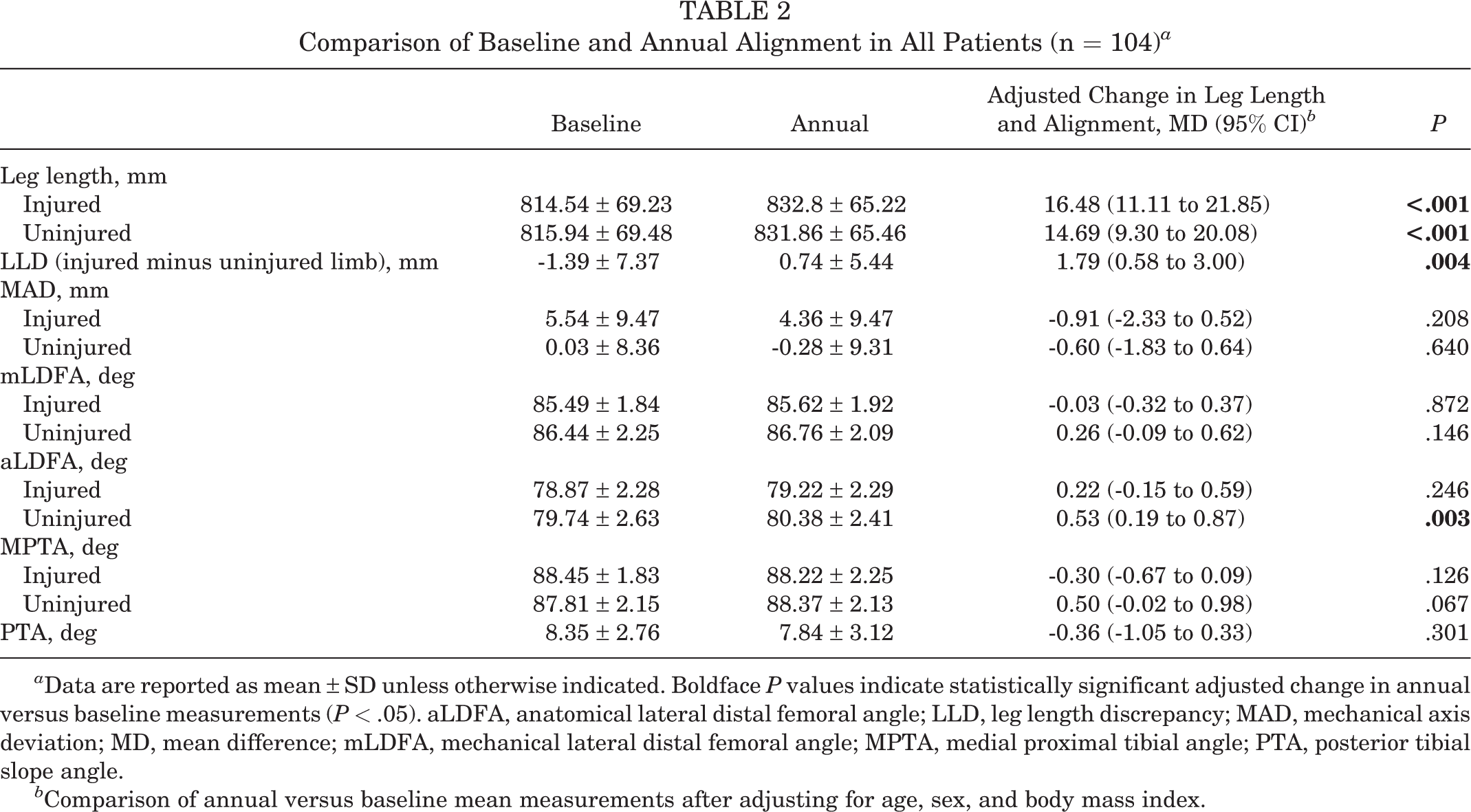
a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant adjusted change in annual versus baseline measurements (P < .05). aLDFA, anatomical lateral distal femoral angle; LLD, leg length discrepancy; MAD, mechanical axis deviation; MD, mean difference; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; PTA, posterior tibial slope angle.
b Comparison of annual versus baseline mean measurements after adjusting for age, sex, and body mass index.
The subgroup analysis of patients with >12 months of growth remaining (n = 34) demonstrated no statistically significant change in mean alignment after transphyseal ACLR after adjusting for covariates. In terms of longitudinal growth, these patients demonstrated no statistically significant change in LLD but significant increases in leg length on both the injured and the uninjured limbs (P < .001 for both), consistent with their level of maturation and therefore with expected growth (Table 3).
Comparison of Baseline and Annual Alignment in Patients With >12 Months of Growth Remaining (n = 34) a

a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant adjusted change in annual versus baseline measurements (P < .05). aLDFA, anatomical lateral distal femoral angle; LLD, leg length discrepancy; MAD, mechanical axis deviation; MD, mean difference; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; PTA, posterior tibial slope angle.
b Comparison of annual versus baseline mean measurements after adjusting for age, sex, and body mass index.
Baseline Alignment
When evaluating presurgical alignment, we incidentally observed that the injured limb was in statistically significantly more valgus compared with the uninjured limb after adjustment for covariates. The MAD was 4.79 mm more lateral on the injured limb compared with the uninjured limb (P < .001). When comparing the injured with the uninjured limb, the distal femur (mLDFA and aLDFA) and proximal tibia (MTPA) had numerical tendencies toward valgus (Table 4). Compared with historical control values, 20 the injured limb was in statistically significantly more valgus whereas the uninjured limb was in slightly more valgus (P < .001 for both) (Table 4).
Baseline Alignment Between Limbs and Compared With Control Ranges in All Patients a

a Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups compared (P < .05). ACL, anterior cruciate ligament; aLDFA, anatomical lateral distal femoral angle; MAD, mechanical axis deviation; MD, mean difference; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; NA, not applicable; PTA, posterior tibial slope angle.
b Positive values indicate lateral mechanical axis deviation, negative values indicate medial mechanical axis deviation.
c Adjusted for age, sex, and body mass index.
Discussion
We conducted a comprehensive prospective evaluation of lower limb alignment in children and adolescents who underwent transphyseal ACLR. We concluded that, after ACLR, there was no significant change in mean lower limb alignment or longitudinal growth when compared with preoperative assessment of the injured limb. However, 7 of 104 patients (6.7%) did develop clinically significant changes to alignment or LLD. We also incidentally observed preoperative differences between the injured and uninjured limbs, suggesting that some patients who present with ACL rupture may have preexisting malalignment of their injured limb.
Overall, ACLR did not lead to a significant change in mean lower limb alignment or longitudinal growth across the entire cohort or within the subgroup of patients with 12 months of growth remaining. However, we found that there was a statistically significant change after ACLR for aLDFA on the uninjured limb. This finding may have been influenced by the relatively low interrater ICC for the aLDFA and, since it was not associated with a corresponding change in MAD or mLDFA in the uninjured limb, it should be interpreted with caution. In agreement with the findings of Koch and colleagues, 14 the leg length on the injured limb demonstrated a small tendency toward overgrowth, as reflected by a positive change in LLD of 1.79 mm toward the injured limb. Although statistically significant, this change in LLD would not be considered clinically significant. It is plausible that measurement error may have contributed to the finding. Indeed, this change in LLD or other changes in alignment were not observed in the subgroup of patients with >12 months of growth remaining, where growth disturbance would be more likely to occur.
Although alignment after transphyseal ACLR has been previously evaluated postoperatively in pediatric patients, these studies have been limited by sample size, radiographic field of view (ie, short-leg radiographs only) and/or by referencing postoperative imaging to typical data rather than the patient’s presurgical status. 3,5,9,11 This study prospectively compared preoperative with postoperative long-leg radiographs and showed that there were no statistically significant changes in mean alignment or longitudinal growth after transphyseal ACLR. However, caution regarding the possibility of growth disturbance should persist given that 7 out of 104 postsurgical patients demonstrated a change in mechanical axis of >10 mm (five patients) or a change in LLD of >10 mm (two patients). For this reason, we recommend clinical and radiographic monitoring of lower limb alignment in all patients with growth remaining who have undergone transphyseal ACLR. This is in keeping with the IOC consensus statement, 1 which suggests that early detection of physeal disturbance is enabled by 12-month postoperative radiographs.
An unexpected finding was that the injured limb demonstrated statistically significant deviation of MAD laterally by a mean of 4.79 mm and a tendency toward a valgus femur and tibia compared with the uninjured limb at baseline. To our knowledge, this is the first study to report asymmetric preoperative alignment using long-leg radiographs in pediatric patients with ACL injuries. Nonetheless, we are likely not the first to observe the phenomenon, as guided growth and simultaneous ACLR has been reported previously. 6 Likewise, a study of 59 pediatric and adolescent patients undergoing transphyseal ACLR identified asymmetric valgus alignment when comparing baseline with postoperative radiographs; however, this was not directly attributed to preoperative deformity. 2 In response to this study, an editorial by Fabricant 7 emphasized that preoperative alignment radiographs should be taken when the patient can fully extend one’s knee. Indeed, Heath and colleagues 13 suggested caution in interpreting long-leg standing radiographs after injury in this cohort. They observed that some patients radiographically demonstrated an LLD that was not present on subsequent imaging. The authors postulated that these patients were altering their stance with flexion at the injured knee, which resulted in the initial observed LLD. In their study, Heath and colleagues reported that 52% of patients had a baseline LLD of >5 mm compared with our cohort, which demonstrated a mean baseline LLD of -1.39 mm. We feel that the absence of a significant LLD at baseline (-1.39 mm) in our study suggests that patients were standing with knees fully extended. This may have been assisted by the lengthy duration between injury and preoperative imaging (∼61 days) giving adequate time for pain and swelling to settle and allow normal positioning of the injured knee joint in stance for the radiograph. We believe this makes interpretation of our cohort’s alignment more valid.
Ultimately, the clinical significance of our incidentally observed preoperative injured limb valgus remains to be determined. When considering malalignment and risk of pediatric ACL rupture, only the posterior tibial slope has been associated with increased risk of pediatric ACL rupture. It is uncertain whether other radiographic parameters indicating malalignment are associated with ACL injuries. 4 Therefore, the influence of valgus alignment on rates of ACL rupture, graft rerupture, meniscal injury, and patient-reported outcomes will be evaluated in the context of our aforementioned registry. Regardless, these findings warrant a more comprehensive collection of preoperative imaging.
Limitations
There are several limitations that should be recognized when interpreting the findings of this study. First, the radiological measures were conducted by a single author. Nonetheless, the ICCs of our radiographic measures in our subgroup analysis were either equivalent or superior to literature values. 23 Second, our follow-up time was a mean of 14.5 months, which may underreport the incidence of growth disturbance in younger patients ofour cohort. However, these patients are monitored until skeletal maturity and the IOC consensus statement advocates for radiological follow-up within 12 postoperative months to detect early physeal disturbance. 1 Importantly, our subgroup analysis of patients with >12 months of skeletal growth remaining demonstrated the same results as the overall group. Finally, although radiographs were captured when patients were able to bear weight, patients may alter their stance postinjury. All efforts to control for this confounder were made through standardized training of appropriate staff.
Conclusion
At a mean postoperative follow-up of 14.5 months, our results demonstrate that pediatric transphyseal ACLR can be performed safely in the majority of patients in this study population although clinically significant changes occurred in roughly 6.7% of patients studied. For this reason, we recommend regular follow-up of patients with growth remaining undergoing transphyseal ACLR.
Footnotes
Acknowledgment
The authors acknowledge the advice and insight of Garrett Malayko.
Final revision submitted March 4, 2023; accepted April 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.P.C. and D.B. have received grant funding to their institutions from Children’s Hospital Foundation (Brisbane) and Smith & Nephew. S.M. has received honoraria from Smith & Nephew. I.P.A. has received consulting fees and honoraria from Smith & Nephew and Orthofix. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children’s Health Queensland Hospital and Research Service (No. HREC/18/QRCH/182).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.