
Abstract
Background:
Questions have been raised concerning the safety of intra-articular anterior cruciate ligament (ACL) reconstruction in prepubescent children aged <7 years. However, normal values for the width of the lateral femoral condylar epiphysis and height of the tibial epiphysis have yet to be established through the use of magnetic resonance imaging (MRI).
Purpose:
To determine normal values for the width of the lateral femoral condylar epiphysis and height of the tibial epiphysis at the knee in prepubescent children aged <7 years by use of MRI and to compare this age group with an older cohort of prepubescent children aged <10 years.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
An electronic search was conducted for pediatric knee MRI examinations at the authors’ institution from March 2003 to March 2013. The total and ossified lateral femoral condylar widths were determined on coronal proton density–weighted images. The total and ossified tibial epiphyseal heights were recorded on the sagittal T1-weighted image best containing the ACL footplate. The intraclass correlation coefficient (ICC) was calculated to determine interobserver agreement. Knees were stratified by age into 2 groups: children between the ages of 3 and 6 years (group 1) and children between the ages of 7 and 9 years (group 2). Each cohort was further stratified by sex.
Results:
Group 1 consisted of 10 children (mean age, 4.3 years) and group 2 consisted of 10 children (mean age, 8.5 years). There were a total of 20 knees. There was a statistically significant difference between groups 1 and 2 for the ossified lateral femoral condylar width where femoral tunnel location would be expected (20.00 ± 4.20 vs 26.27 ± 4.12 mm, respectively; P = .0035) and for total lateral femoral condylar width (25.57 ± 3.47 vs 29.43 ± 4.04 mm, respectively; P = .0339). No difference was found for total tibial epiphyseal height between the 2 groups. However, there was a difference between groups 1 and 2 for ossified tibial epiphyseal height (13.20 ± 1.63 vs 15.27 ± 0.94 mm, respectively; P = .0028). No difference was found for average ossified tibial epiphyseal height or ossified lateral femoral condylar width between boys and girls in the younger or older cohorts. The ICC was strong (>0.7) at femoral and tibial locations where tunnel placement would be expected.
Conclusion:
Prepubescent children <7 years old have smaller knee epiphyses than older prepubescent children, and on average, present with an osseous bone stock of 20 mm for lateral femoral condylar width and 13 mm for tibial epiphyseal height. Study results suggest that children aged <7 years possess enough osseous bone stock at the lateral femoral condyle to support transepiphyseal ACL reconstruction. However, future studies will be necessary to determine the safety and effectiveness of this procedure in children aged <7 years.
Clinical Relevance:
ACL tears in children are more frequently being recognized by the orthopaedic community. The trend toward increasing participation in competitive and recreational sports has contributed to this phenomenon. Young patients with complete ACL tears and open growth plates often provide a management dilemma for surgeons who wish to perform reconstructive surgery.
Keywords
The diagnosis of anterior cruciate ligament (ACL) injury in the skeletally immature knee is increasing in frequency. 21,27,32 However, determining the best treatment option for complete ACL tear remains controversial. 11,21 Trends of increased participation in sports and recreational endeavors by children are contributing factors. Since skeletally immature patients may not reliably limit their physical activity following injury, 1,16,29 early surgical intervention to address complete ACL tear and to restore knee stability is gaining acceptance as a strategy for the prevention of chondral and meniscal abnormalities associated with nonoperative management. 1,2,13,17,23,28,29,34
Surgical techniques that spare knee physes are important for young populations, since the risk of iatrogenic growth disturbance is most concerning for children with at least 5 cm of remaining lower extremity growth potential. 4,16 Potential poor outcomes for children with ACL reconstructions that cross growth plates are known to include angular deformity and leg length discrepancies related to premature growth plate closure or lower extremity overgrowth. 6,7,10,14,22 Both intra-articular and extra-articular physeal-sparing ACL procedures exist to avoid physeal injury during reconstructive surgery. Intra-articular techniques have been championed recently as they have been shown to better restore normal knee kinematics. 2,15,24 However, intra-articular physeal-sparing ACL reconstruction procedures are not without risk, and the potential for growth plate injury has been described. 5,25
Questions about which children are too young to receive intra-articular physeal-sparing surgery have been raised in the literature. 3,30 Some proponents have suggested that this technique may be safe in children as young as 5 years, although no definitive evidence exists to support this procedure as an established practice. 3 Concerns about the safety of intra-articular physeal-sparing ACL reconstruction are relevant since complete ACL tears in children younger than 7 years have been reported. 8,31,35 Congenital absence of the ACL also has been described, and symptomatic knees in this population present a management dilemma similar to complete ACL tear. 19,20,33
As the orthopaedic community reduces the role of traditional nonoperative management in favor of earlier surgical intervention, open questions remain about what strategies constitute best management practices for young children. Variables relevant to surgical tunnel placement that are entirely in knee epiphyses have been described in prepubescent children and adolescents. These include the height of the tibial epiphysis and the width of the lateral femoral condylar epiphysis. 9,18 However, these parameters have not yet been established for children of early primary school age and younger (<7 years). Determining normal values for the width of the lateral femoral condylar epiphysis and the height of the tibial epiphysis for children younger than 7 years can provide a starting point for addressing the potential safety of intra-articular physeal-sparing ACL surgery in young prepubescent knees. Surgeons can use these values as a reference to aid in decision making about management during the workup of complete ACL tear or congenitally absent ACLs in young children.
The purposes of this study were to determine normal values for width of the lateral femoral condylar epiphysis and height of the tibial epiphysis in prepubescent children younger than 7 years using magnetic resonance imaging (MRI) of the knee and to compare this age group with an older cohort of prepubescent children younger than 10 years. We hypothesized that the younger cohort would have less ossified bone stock and smaller total size for the average width of the lateral femoral condylar epiphysis and height of the tibial epiphysis when compared with the older cohort.
Materials and Methods
The study was approved by the authors’ institutional review board and complied with Health Insurance Portability and Accountability Act guidelines. The requirement for patient informed consent was waived for this retrospective study.
The study population consisted of children between the ages of 3 and 9 years. Patients undergoing an MRI of the knee between March 2003 and March 2013 were identified through an electronic search of our departmental picture archiving and communication system (PACS). Inclusion criteria were as follows: (1) an intact ACL or a mild sprain of the ACL that did not preclude clear delineation of its normal landmarks and morphology, (2) normal proximal tibial epiphysis morphology, and (3) normal distal femoral epiphysis morphology. A total of 27 knees were identified during the search. Seven knees were excluded for the following reasons: Blount disease (n = 2), chondroblastoma at the lateral femoral condyle (n = 1), and wide field of view imaging not typically performed during routine MR knee examinations (n = 4). Therefore, 20 knees (12 male and 8 female; mean age, 6.4 years; range, 3-9 years) were included in the study. Children within the age range of this study have been described as high risk for iatrogenic physeal injury following transphyseal ACL reconstruction surgery. 4 We stratified our study population further into 2 cohorts. Group 1 consisted of younger children of toddler, preschool, and early primary school age (range, 3-6 years), and group 2 consisted of an older primary school age group (range, 7-9 years).
Most MRI examinations were performed at 1.5 T (Magnetom Avanto or Espree; Siemens, Erlangen, Germany) or at 3.0 T (Magnetom Trio; Siemens, Erlangen, Germany). Two MRI examinations, however, were performed at 1.5 T (Eclipse; Philips Medical System, Best, the Netherlands). MRI examinations included standard 2-dimensional (2D) coronal turbo spin-echo (TSE) proton density (PD)–weighted (or T1-weighted) and sagittal SE T1-weighted sequences, with a slice thickness of either 3 or 3.5 mm. A single examination had a slice thickness of 4 mm for coronal and sagittal sequences, and a single examination had a slice thickness of 2.5 mm for the sagittal sequence. For a single examination, a standard 2D coronal short tau inversion recovery (STIR)–weighted sequence was used because of the absence of a coronal PD- or T1-weighted sequence. Each knee examination contained a sagittal TSE T2-weighted fat saturation or STIR sequence that was available for comparison.
Two musculoskeletal radiologists and 1 musculoskeletal radiology fellow independently and retrospectively reviewed the images on a PACS workstation. The height of the tibial epiphysis was evaluated from the sagittal T1-weighted image best containing the ACL and its tibial footplate (Figure 1). 9 Two separate measurements were obtained: (1) The height of the tibial epiphysis was determined as the vertical distance from the cartilaginous attachment site at the midpoint of the ACL footplate to the proximal tibial epiphysis–physis interface and (2) the height of the ossified portion of the tibial epiphysis was also measured as the vertical distance from the superior margin of the ossified tibial epiphysis in line with the midpoint of the ACL footplate to the proximal tibial epiphysis–physis interface. In this study, we included knees that had intact ACLs or mild sprains, in order that the location of the tibial footplates could be readily identified. We did so to provide a reliable location for reproducible measurement and to provide a height of the tibial epiphysis that best correlated with the location of the native ACL footprint.
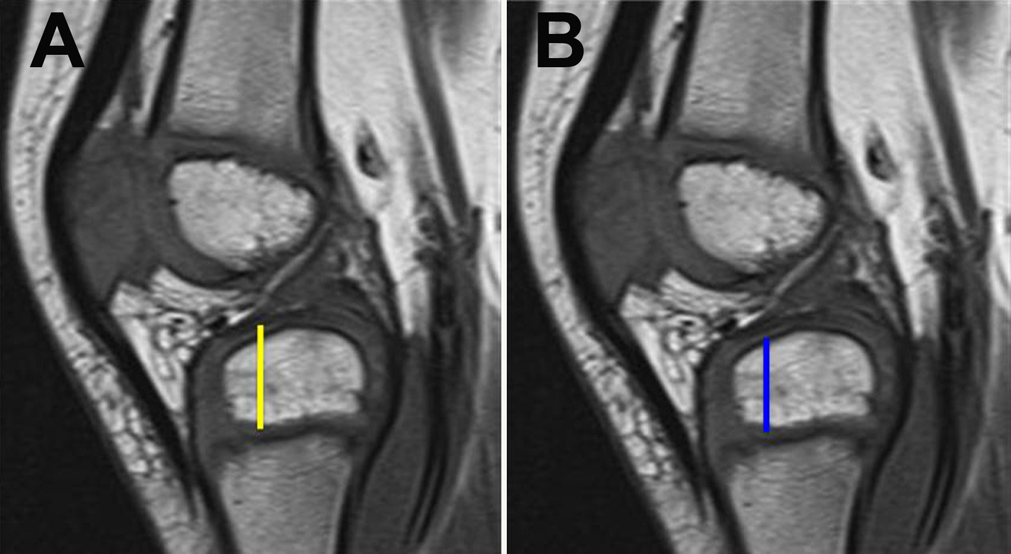
Sagittal T1-weighted magnetic resonance images demonstrating how tibial epiphyseal height measurements were obtained. (A) Total height, including ossified and cartilaginous anlage components (yellow line). (B) Ossified component only (blue line).
The width of the lateral femoral condylar epiphysis was determined using 2 separate techniques. 9 The first method (method 1) included finding the sagittal image best containing the ACL and the MR equivalent of the Blumensaat line; then, the localizer function at the PACS workstation was utilized to select the coronal PD image that corresponded to one-fourth the distance along the Blumensaat line in a posterior to anterior direction (Figure 2A). The distance from the footplate of the ACL to the lateral cartilaginous margin of the lateral femoral condylar epiphysis was then measured as a horizontal line (Figure 3A). Lastly, the distance from the footplate of the ACL to the lateral margin of the ossified portion of the lateral femoral condylar epiphysis was obtained (Figure 3B). The second method (method 2) involved identifying the anterior-most of 3 consecutive coronal slices through the lateral femoral condylar epiphysis on the sagittal image (Figure 2B), then measuring the total width and ossified width, as performed with the first method (Figure 3).

Methods of selecting coronal images for lateral femoral condylar width measurement. (A) Method 1: Sagittal T1-weighted magnetic resonance image at the Blumensaat line (line). One fourth the distance posterior (Pos) to anterior (Ant) was ascertained (asterisk), and the localizer function provided the corresponding coronal image for measurement. (B) Method 2: Sagittal T1-weighted image showing the first 3 coronal slices through the lateral femoral condyle. The coronal image from the third slice was used for measurement.
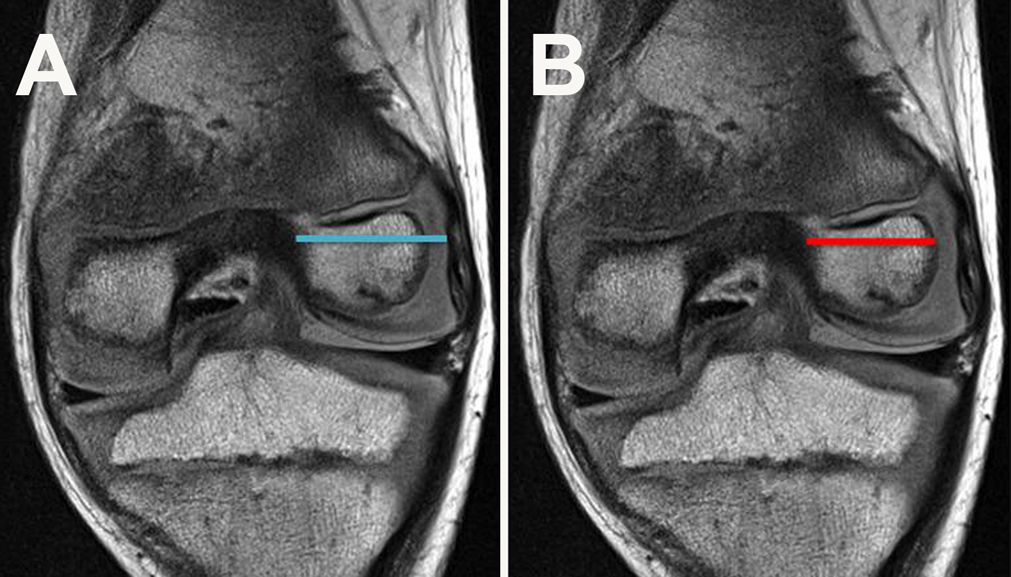
Coronal proton density–weighted magnetic resonance images demonstrating how lateral femoral condylar width measurements were obtained. (A) Total width, including ossified and cartilaginous anlage components (blue line). (B) Ossified component only (red line).
Statistical analysis was performed by calculating the mean tibial epiphyseal height (total height and ossified height) and lateral femoral condylar width (total width and ossified width) for each individual knee from the measurements provided by each observer. Group 1 and group 2 mean measurements were compared using the unpaired t test. Each cohort was further stratified by sex and also compared by use of the unpaired t test. In addition, the mean age of group 1 and group 2, and the mean age by sex in each cohort, were compared with the unpaired t test. A P value <.05 was considered to indicate a significant difference. Interobserver agreement was assessed by calculating intraclass correlation coefficient (ICC) on a scale of 0 to 1 (0.0-0.2 = poor agreement, 0.3-0.4 = fair agreement, 0.5-0.6 = moderate agreement, 0.7-0.8 = strong agreement, and >0.8 = nearly perfect agreement).
Results
Group 1 (n = 10) consisted of a younger cohort of knees with a mean age of 4.3 years (standard deviation [SD], ±1.2 years; range, 3-6 years). Group 2 (n = 10) consisted of an older cohort of knees with a mean age of 8.5 years (SD, ±0.9 years; range, 7-9 years). The age difference for group 1 versus group 2 was statistically significant (P < .0001). The mean total tibial epiphyseal height showed no difference. The ossified tibial epiphyseal height, however, did significantly differ between cohorts (P < .003, Table 1). The younger cohort of knees had a mean ossified tibial height of 13.2 mm versus 15.3 mm for the older children. Significant differences also were identified between group 1 and group 2 with regard to the mean total width of the lateral femoral condylar epiphysis by the first method and the mean width of the ossified portion of the epiphysis by the first and second methods (Table 1). The largest mean measurement by either method for the total width of the lateral femoral condyle was 25.6 and 29.4 mm for the younger and older groups, respectively. The ossified portion of the lateral femoral condyle for each group was smaller, with the mean for group 1 measuring 20.0 mm as compared with 26.3 mm for group 2. There was no significant difference in ossified tibial epiphyseal height or ossified lateral femoral condylar width between male and female patients in group 1 (Table 2). Girls had less total tibial epiphyseal height than boys in group 1, measuring 14.7 versus 16.3 mm on average, respectively (P = .0191). Girls also had less total lateral femoral condylar width than boys in group 1, measuring 23.3 versus 27.9 mm on average, respectively (P = .0247). There was no significant difference between total or ossified tibial epiphyseal height and lateral femoral condylar width between male and female patients in group 2 (Table 3). A summary of age, sex, and mean measurements for each knee is presented in Table 4. There was no significant difference in age between boys and girls in group 1 or group 2, respectively. The general measure of agreement among radiologists for each measurement is provided in Table 5. During this study, strong interobserver agreement was found for each parameter except for determination of the total height of the tibial epiphysis, where moderate-to-strong agreement was present.
Tibial Epiphyseal Height and Lateral Femoral Condylar Width for Group 1 Versus Group 2

a Values are expressed in millimeters as mean ± standard deviation.
Tibial Epiphyseal Height and Lateral Femoral Condylar Width for Girls Versus Boys in Group 1
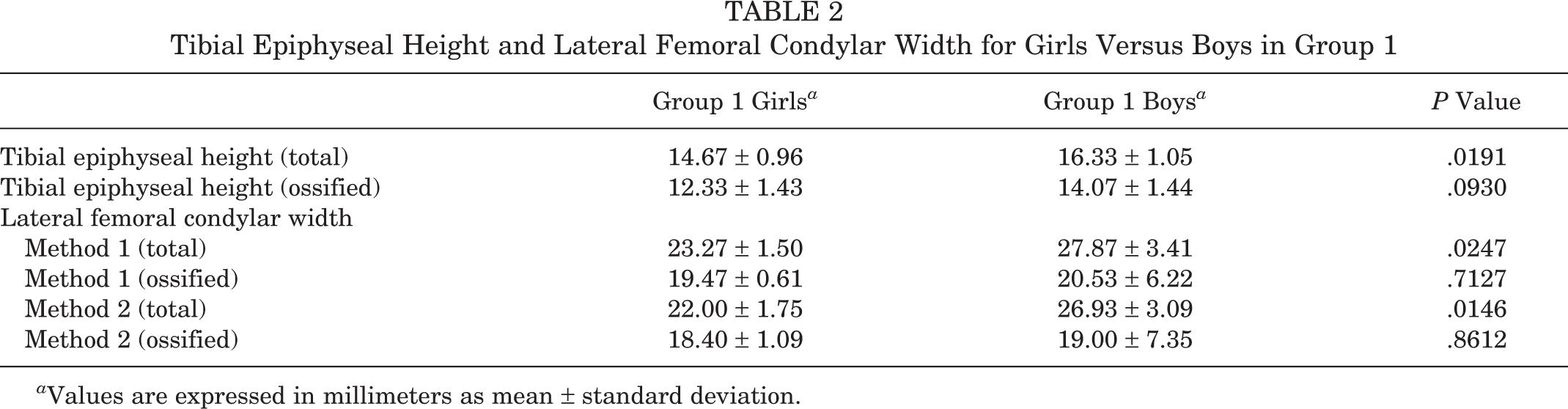
a Values are expressed in millimeters as mean ± standard deviation.
Tibial Epiphyseal Height and Lateral Femoral Condylar Width for Girls Versus Boys in Group 2

a Values are expressed in millimeters as mean ± standard deviation.
Sex, Age, and Average Measurements for Each Knee a

a Values are expressed in millimeters.
Level of Interobserver Agreement for Measurements

Discussion
Early surgical intervention is gaining acceptance as a treatment strategy for complete ACL tear in the skeletally immature knee. 1,2,13,17,23,28,29,34 However, best management practices remain a subject of controversy in the orthopaedic community. 11,21 Questions persist about which knees are too immature for intra-articular ACL reconstruction. 3,30 Concerns about growth plate disturbance persist, since iatrogenic complications may result in the need for major limb reconstruction. 20 As a consequence, many surgeons still prefer initial nonoperative management for complete ACL tear in the young prepubescent knee despite the risk of poor outcomes. 21 Some authors have suggested ACL reconstruction should be avoided entirely in prepubescent children who are shorter than older siblings and parents by at least 10 to 15 cm. 27
The incidence of skeletally immature knees requiring ACL reconstruction is poorly understood for prepubescent children younger than 7 years. Complete ACL tears in this age group are thought to be uncommon, and a few cases are reported in the literature. Waldrop and Broussard 35 reported a case of a 3-year-old girl who suffered a complete ACL tear at the midsubstance after a fall. The ligament was debrided but ACL reconstruction was not performed because of concerns about epiphyseal growth arrest. Schaefer et al 31 reported a case of a 4-year-old boy who sustained a complete ACL tear at the midsubstance after falling off a toboggan. The ACL tear was treated with primary repair, but the ACL was completely absent at follow-up arthroscopy 5 years later. Corso and Whipple 8 described a case of a 3-year-old boy who presented without a known history of trauma and who was shown to have an unusual avulsion of the ACL that peeled off the cartilage anlage of the femoral epiphysis at arthroscopy. Treatment involved debridement and reapproximation of the ligament with the femoral attachment site, followed by immobilization with the knee in extension.
Symptomatic congenital absence of the ACL is another source of knee instability for young children. Case reports have described ACL reconstruction in children younger than 7 years. Kocher et al 20 presented a case of a 3-year-old boy with symptomatic knee instability from congenital absence of the ACL and associated proximal femoral focal deficiency. ACL reconstruction was performed with an iliotibial band graft as a combined intra-articular and extra-articular reconstruction. Knorr et al 19 reported a case of a 3-year-old boy who presented with an isolated congenital aplasia of the ACL. A Clocheville ligamentoplasty was performed at age 5 years because of instability at the knee.
The lower age limit for ACL reconstructive surgery in the skeletally immature knee has not been established. Some authors have suggested that this procedure should be avoided in prepubescent children with substantial remaining growth potential. 27 However, in a survey of the Herodicus Society and The ACL Study Group in 2002, respondents claimed to have performed ACL reconstructions in patients as young as 2 years, although details about indications or techniques were not provided. 21
Some authors have speculated that intra-articular physeal-sparing ACL reconstruction is theoretically possible in prepubescent children younger than 7 years. 3 However, intra-articular ACL reconstructions that do not cross physes are not entirely without risk for growth plate injury. Lawrence et al 25 reported the case of an adolescent who suffered premature closure of the lateral femoral physis following revision ACL reconstruction despite the belief that no direct transgression to the physeal plate had occurred. Theoretical mechanisms for injury to the femoral physis, in addition to direct transphyseal drilling, were speculated to include indirect thermal and pressure insults that occurred at the time of epiphyseal drilling. Proximity of the femoral physis to the femoral origin of the ACL is another important variable relevant to the safety of ACL reconstruction techniques in children, with ramifications for intra-articular or combined extra-articular and intra-articular procedures. 5,26 Iatrogenic injury to the gastrocnemius tendon, lateral collateral ligament, and popliteus tendon have been described as other potential risks during transepiphyseal ACL reconstruction. 12
For young, prepubescent children younger than 7 years, establishing the expected average normal size of epiphyses at the knee is important since there is less margin for error during surgery as compared with older children and adolescents. Young prepubescent children have smaller bones. In addition, children younger than 7 years have a higher percentage of nonossified cartilage anlage at the knee compared with older children. Davis et al 9 used MRI to determine normal references for the average tibial epiphyseal height and lateral femoral condylar width in children and adolescents aged 7 to 16 years. We are unaware of any similar study in the literature that evaluates tibial epiphyseal height and lateral femoral condylar width in children younger than 7 years on MRI. Our study divided knees into 2 cohorts: (1) children aged 3 to 6 years and (2) children aged 7 to 9 years. The difference between the mean ages of the younger and older cohorts was statistically significant, with a P value <.0001.
With regard to the height of the ossified portion of the tibial epiphysis, in our study, a significant difference existed between the younger and older cohort of knees, measuring 13.2 and 15.3 mm, respectively (P = .0028). Therefore, we conclude that prepubescent children (<7 years) have less osseous bone stock in terms of tibial height than their older counterparts (≥7 years). There was no difference between the 2 groups with regard to the average total tibial epiphyseal height (cartilage anlage and ossified portion). Interestingly, where interobserver agreement was strong for osseous tibial epiphyseal height measurement, interobserver agreement was only moderate to strong for total tibial epiphyseal height measurements. This most likely reflects the more difficult task of differentiating the superior margin of the thin tibial epiphyseal cartilage anlage from the insertion site of the distal ACL, especially in the older cohort of knees. When comparing boys and girls in the same cohort, no difference was found for the older group of knees. In the younger cohort, girls demonstrated a 1.6-mm shorter total tibial epiphyseal height on average than boys (P = .0191), but there was no sex difference for the ossified tibial epiphyseal height.
Significant differences also existed for the width of the ossified bone stock of the lateral femoral condylar epiphysis between the 2 groups. The maximum widths obtained in the study were acquired by the first method (method 1). The average width of the younger cohort was smaller than the older cohort by 6.2 mm (P = .0035). Therefore, in a similar fashion to tibial epiphyseal height, we conclude that prepubescent children (<7 years) of toddler, preschool, and early primary school age have less expected osseous bone stock in terms of lateral femoral condylar epiphyseal width than older children (≥7 years). Our study found that the expected average normal ossified portion of lateral femoral condylar width for children younger than 7 years was 20.0 mm. For the total lateral femoral condylar epiphyseal width (cartilage anlage and ossified portion), the maximum average widths were also obtained using the first method (method 1) for both groups. The younger cohort was smaller in width than the older cohort by 3.8 mm (P = .0339). The second method (method 2) produced smaller average values than the first method (method 1) for total and ossified lateral femoral condylar width measurements for both groups, reflecting that the first method coronal slice was more anterior than the second method coronal slice. 9 When comparing boys and girls in the same cohort, no difference was found for the older group of knees. In the younger cohort, girls demonstrated on average 4.6 mm less (P = .0247) total lateral femoral condylar width than boys, but no sex difference was found for ossified lateral femoral condylar width.
Currently, the minimum length of femoral graft required for ACL reconstruction is unknown. 36 Although the average total lateral femoral condylar width for prepubescent children younger than 7 years was 25.6 mm, the ossified width was only 20.0 mm in our study. Lawrence et al 24 described a procedure that placed a 23-mm interference screw across the femoral epiphysis in an older subset of children (aged 10-12 years). Because of the limitations of the ossified width of the lateral femoral condyle, ACL reconstruction with a suspensory soft tissue graft mechanism may be a more feasible method in children younger than 7 years. A technique proposed originally for older prepubescent children and adolescents by Anderson 2 described a minimum length of 20 mm of quadruple hamstring tendon graft for the femoral tunnel. However, in a skeletally mature goat model, Zantop et al 36 showed no difference in knee kinematics or structural properties between knees with 15 versus 25 mm of soft tissue femoral graft at 12 weeks following intra-articular ACL reconstruction. This suggests that prepubescent children younger than 7 years possess enough ossified bone stock at the lateral femoral condyle to support a soft tissue graft ACL reconstruction. However, future studies will be necessary to assess long-term outcomes, safety, and applicability to young, skeletally immature human knees. One important variable that remains unknown is the healing response of the nonossified cartilage anlage at the lateral femoral condylar epiphysis following soft tissue graft placement. In the study by Zantop et al, 36 the goat model involved at least 25 mm of ossified femoral bone stock for each knee even though only 15 mm of soft tissue graft was placed in the femoral tunnel. Other relevant variables, with implications for the safety of ACL reconstruction in the skeletally immature knee, are the relationship between the length versus volume of soft tissue graft in the femoral tunnel and the ramifications of tunnel diameter.
Our study determined the size of the tibial epiphysis as a vertical height, but this measurement may have shortcomings since the tibial tunnel is instead placed along an oblique course during transepiphyseal ACL reconstruction. 2,15,24 Kim et al 18 described an equation to convert the vertical height of the tibial epiphysis obtained on lateral knee radiographs into a longer oblique length to establish the maximum interference screw size that could be placed at surgery without violating the tibial physis. Future studies directly measuring the expected length of the tibial epiphysis along the oblique trajectory of the tibial tunnel on cross-sectional imaging may provide further insights for intra-articular ACL reconstruction techniques that involve a suspensory soft tissue graft method, since the length of graft in the tibial tunnel affects the amount of available graft that can be pulled into the femoral tunnel. 36
Magnetic resonance imaging is a particularly useful modality for the evaluation of the prepubescent knee in children younger than 7 years, since bone and cartilage anlage can be directly evaluated and studies are performed without ionizing radiation. MRI is a valuable resource for preoperative planning before intra-operative fluoroscopy-guided physeal-sparing ACL reconstructive surgery with regard to (1) localization of physes, (2) evaluation of epiphyseal size, (3) estimation of osseous epiphyseal bone stock, and (4) planning of tunnel course and angle. Preoperative MRI planning coupled with the use of intraoperative 3D computed tomography during ACL reconstruction has the potential to optimize tunnel placement and decrease the risk of physeal injury. 24,25
The limitations of our study include the retrospective nature of the research. Knees were identified by a search of our hospital PACS without regard for patient history or physical examination findings. Also, no prospective correlation with skeletal age was performed. The small number of knees included in the study is a limitation. Our results may not be applicable to the general population because of the small sample size. Future studies with a larger number of knees may be required to validate the conclusions of this study. Another possible limitation is that the MRI examinations were performed on different scanners within our hospital system, however, all imaging protocols were similar in terms of sequences acquired and slice thickness.
Conclusion
We found differences for the width of the lateral femoral condylar epiphysis between our younger and older cohorts of skeletally immature knees. Prepubescent children younger than 7 years are more likely to have smaller lateral femoral condyles, and on average, present with an osseous bone stock of 20 mm for lateral femoral condylar width. Therefore, our study suggests that children younger than 7 years possess enough osseous bone stock at the lateral femoral condyle to support transepiphyseal ACL reconstruction based on prior research in an animal model. However, future human studies are necessary to determine the safety and effectiveness of this procedure in children younger than 7 years. The osseous tibial epiphyseal height in young prepubescent children is also less than in older children. On average, children younger than 7 years have 13 mm of osseous bone stock for the height of the tibial epiphysis.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.