
Abstract
Background:
Physeal-sparing anterior cruciate ligament (ACL) reconstruction is being performed increasingly in skeletally immature knees.
Purpose:
To determine normal values for the maximum oblique length and “safe” physeal-sparing length and their corresponding angular trajectories across the tibial epiphysis on reconstructed magnetic resonance images (MRIs) in children and adolescents.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
An electronic search for pediatric knee MR examinations from April 2003 to April 2013 was performed at our institution. A 3-dimensional system viewer was used to measure the maximum oblique length, physeal-sparing length, and their corresponding angular trajectories on reconstructed MRIs. Knees were stratified by age into 2 groups: group 1 consisted of boys <13 years and girls <12 years and group 2 consisted of older boys (13-14 years) and girls (12-14 years). Each cohort was further stratified by sex. Group 1 consisted of 36 knees (mean age, 10.9 years) and group 2 consisted of 59 knees (mean age, 13.6 years).
Results:
Significant differences existed for the maximum oblique length and its angular trajectory for the younger versus older cohort (22.2 ± 2.7 vs 23.8 ± 2.7 mm, P = .007; 42.0° ± 4.0° vs 39.4° ± 4.2°, P = .003) and for the physeal-sparing length and its angular trajectory (19.4 ± 2.8 vs 21.3 ± 2.9 mm, P = .001; 30.1° ± 4.1° vs 28.2° ± 4.5°, P = .042). In group 2, females had shorter maximal oblique length and physeal-sparing length than boys (22.7 ± 2.3 vs 25.0 ± 2.7 mm, P < .001; 20.3 ± 2.6 vs 22.4 ± 2.9 mm, P = .004).
Conclusion:
The maximum oblique length across the tibial epiphysis is shorter than previously believed, measuring approximately 22 mm and approximately 24 mm for high- and intermediate-risk knees, respectively. However, “safe” physeal-sparing lengths were only approximately 19 mm and 21 mm for the younger and older cohorts, respectively. The angles corresponding to the maximum and safe lengths are more acute than commonly thought, measuring approximately 40° and 30°, respectively. All prepubescent knees and intermediate-risk females should receive careful attention before ACL reconstruction due to the relative smaller size of their tibial epiphyses.
Clinical Relevance:
Physeal-sparing ACL reconstruction is gaining acceptance as a surgical option for complete ACL tear in skeletally immature knees. Iatrogenic growth disturbance after violation of an open growth remains a real concern for surgeons tasked with providing operative management for the unstable pediatric knee. Inadvertent iatrogenic growth plate injury to the tibial physis has been shown to occur more commonly than surgeons would intend during physeal-sparing ACL reconstruction.
The incidence of anterior cruciate ligament (ACL) injury is increasing for children and adolescents, as the rate of ACL reconstruction in pediatric knees nearly tripled between 1990 and 2009. 10,21,28,35 The rising participation of boys and girls in recreational activities and organized sports has contributed to this trend. 1,30 Early surgical intervention in skeletally immature knees after complete ACL tear is gaining acceptance in the orthopaedic community. 2,4,15,37 Avoiding delay in operative management may be important since active youths may not reliably follow medical advice to limit their participation in physically rigorous pursuits. 1,16 Nonoperative treatment or delayed ACL reconstruction are losing favor since these strategies are associated with higher rates of subsequent chondral and meniscal injuries. 4,13,17,24,29,30,33,37
Best management practices for ACL reconstruction in skeletally immature knees remain controversial. 12,21 The risk of iatrogenic growth disturbance after transphyseal ACL reconstruction remains a point of contention. Surgical techniques that violate open growth plates have been argued to be safe, 5 but evidence exists that iatrogenic injury can be associated with premature growth arrest, angular deformity, limb overgrowth, and leg length discrepancy. 6,11,14,22,34 One critical factor is skeletal maturity at the time of ACL reconstruction. Children and adolescents with ≥5 cm of expected future lower limb growth are at the greatest risk of iatrogenic growth disturbance after physeal injury. 3,16,32 Thus, physeal-sparing techniques that place graft tunnels entirely in the epiphyses during ACL reconstruction in skeletally immature knees with substantial remaining growth potential have been advocated. 2,12,15,25
Despite the intention of physeal-sparing ACL techniques to avoid growth plate injury, these procedures are not entirely without risk for iatrogenic growth disturbance. Inadvertent violation of the growth plate during physeal-sparing ACL reconstruction has been demonstrated to occur more commonly than previously believed, 31 and angular deformity and limb overgrowth have been reported in association with physeal-sparing techniques. 19 In addition, iatrogenic growth plate disturbance also has been shown to occur without direct violation of a physis during ACL reconstruction. 26 Therefore, the safety of physeal-sparing ACL reconstruction in skeletally immature knees remains unknown.
Tibial tunnel length, angular trajectory, and proximity to the physis are critical parameters for the safety of physeal-sparing ACL reconstructive surgery. Anatomic variables relevant to tunnel placement entirely within the tibial epiphysis have been described on magnetic resonance imaging (MRI). These include the vertical height of the tibial epiphysis, the maximum oblique length of the tibial epiphysis, and its angular trajectory along the expected course of the tibial tunnel. 8,9,36 The maximum oblique length across the tibial epiphysis has been viewed as the more useful parameter, as compared with the vertical height, due to its closer proximity in actual length along the expected course of the tibial tunnel. Past studies have relied on conventional 2-dimensional (2D) sagittal images acquired during standard knee MRI for determination of maximum oblique length and its corresponding angular trajectory. However, this conventional technique provides only an estimate for these parameters. This method is limited by providing measurements that are not in line with the actual expected course of the tibial tunnel and falls short of the information that would be derived from 3-dimensional (3D) reconstruction techniques. 36 Image postprocessing with a 3D visualization system, on the other hand, allows for reconstruction of the true MR sagittal oblique image plane necessary to obtain the angular trajectory and oblique length of the tibial epiphysis along the course of the expected tibial tunnel placement. Likewise, use of a 3D visualization system also allows for localization of the superior tip of the tibial physis corresponding to the expected sight of the tibial tunnel placement, which is necessary to provide the most accurate measurements of tibial tunnel length and angular trajectory from the anterior margin of the tibial epiphysis to the ACL footplate.
The purpose of this study was to determine normal values for the oblique length and corresponding angular trajectory across the tibial epiphysis pertinent to physeal-sparing ACL reconstruction in children and adolescents. We hypothesized that the maximum oblique length is shorter and its corresponding angular trajectory more acute than previously reported, since prior studies did not obtain measurements corresponding to the superior tip of the tibial physis at the level of the anteromedial margin of the tibial epiphysis where tunnel placement would be expected to be placed. We also hypothesized that oblique lengths across the tibial epiphysis, measured at a distance from the physis and simulating a “safe” tunnel placement, would have a shorter length and a more acute angular trajectory than previously believed for children and adolescents.
Methods
The study was approved by an institutional review board and complied with Health Insurance Portability and Accountability Act guidelines. The requirement for patient informed consent was waived for this retrospective study. The study population consisted of children and adolescents between the ages of 10 and 14 years. Patients undergoing an MRI of the knee between April 2003 and April 2013 were identified through an electronic search of our departmental picture archiving and communication system (PACS). Inclusion criteria were as follows: (1) an intact ACL or a mild sprain of the ACL that did not preclude clear delineation of its normal landmarks and morphology and (2) normal morphology of the proximal tibia. A total of 109 knees were identified. Fourteen knees were excluded from the study for the following reasons: ACL tear (n = 8), ACL reconstruction (n = 2), Blount disease (n = 2), tibial fracture at the ACL insertion (n = 1), and an incomplete study without sagittal images (n = 1). Therefore, 95 knees (51 male and 44 female; mean age, 12.6 years; range, 10-14 years) were included in the study. The physis was discernable on all included knees, and no knee had to be excluded on the basis of a closed growth plate. We stratified our study population into either high- or intermediate-risk cohorts for iatrogenic injury after ACL reconstruction based on guidelines provided by Anderson and Anderson. 3 Group 1 consisted of boys younger than 13 years (range, 10-12 years) and girls younger than 12 years (range, 10-11 years); group 2 consisted of boys between the ages of 13 and 14 years and girls between the ages of 12 and 14 years. Knees were stratified by chronological age, and no attempt was made to identify bone age.
All MRI examinations were performed at 1.5 T or 3.0 T and included standard 2D sagittal spin-echo T1-weighted sequences, with a slice thickness of either 3 or 3.5 mm. Four examinations had a slice thickness of 4 mm on sagittal sequences. For a single examination, a standard 2D sagittal turbo spin-echo (TSE) T1-weighted fat saturation sequence was used due to absence of a T1-weighted sequence. Each knee examination also contained a short-tau inversion recovery (STIR) sequence or a sagittal TSE T2-weighted fat saturation that was available for comparison.
A single musculoskeletal radiologist retrospectively reviewed all images on a 3D visualization system viewer (Aquarius iNtuition Edition, version 4.4; TeraRecon Inc). Aquarius iNtuition is a widely available commercial imaging viewer with tools that allow for 3D postprocessing of clinical MRI examinations. All measurements were performed after import of the sagittal T1 sequence into Aquarius iNtuition, and then each measurement was repeated 8 weeks later for calculation of intraobserver reliability. To determine interobserver reliability, a research assistant with training in Aquarius iNtuition performed measurements for one-half the total number of knees. The vertical height of the tibial epiphysis was evaluated from the sagittal T1 image best containing the ACL and its tibial footplate, as previously described by Davis et al. 9 The vertical height of the tibial epiphysis was measured as the vertical distance from the superior margin of the tibial epiphysis in line with the midpoint of the ACL footplate to the tibial epiphysis–physis interface. Since physeal-sparing ACL reconstruction necessitates avoidance of the growth plate, the superior tip of the tibial physis was localized at the anteromedial margin of the tibia on review of serial reformatted axial slices (Figure 1). Localization of the superior tip of the physis on axial images was necessary for determining where to measure maximum oblique length in the trajectory of a tibial tunnel. Drilling of a tibial tunnel in physeal-sparing ACL reconstruction requires an oblique course, beginning medially at the anterior tibial epiphyseal margin and exiting laterally at the ACL footplate (Figure 2). To produce the imaging plane in line with the true expected obliquity of a tibial tunnel, reformatted sagittal oblique images were obtained at 10° and 20° relative to the short axis of the tibia (Figure 3). The maximum oblique length of the tibial epiphysis and its corresponding angular trajectory were obtained on both the 10° and 20° sagittal oblique images from the anteromedial margin of the tibial epiphysis (corresponding to the level of the superior tip of the physis at the anteromedial margin of the tibia) to the midpoint of the ACL footplate (Figure 4). Then, a second physeal-sparing length and its corresponding angular trajectory were determined on both the 10° and 20° sagittal oblique images from the anteromedial margin of the tibial epiphysis (corresponding to a level 5 mm above the superior tip of the physis at the anteromedial margin of the tibia) to the midpoint of the ACL foot plate. It is not uncommon for prepubescent knees to be evaluated with incomplete ossification of the tibial epiphyseal cartilaginous anlage. 8 Only the ossified portion is visualized on radiographs but the entire tibial epiphysis is visible on MRI. A minority of knees (12.6%) included in the study had incompletely ossified tibial epiphyses, and the maximum oblique length and physeal-sparing length measurements for these knees included the entire distance from the anteromedial margin of the cartilaginous portion of the tibial epiphysis to the midpoint of the ACL footplate to determine the absolute amount of distance across the tibial epiphysis for each parameter.

Axial T1-weighted magnetic resonance images illustrating regions of proximal tibial anatomy. (A) Plane of the tibial physis; (B) superior tip of the tibial physis near the anteromedial margin of the tibia (arrow); (C) plane of the tibial epiphysis.
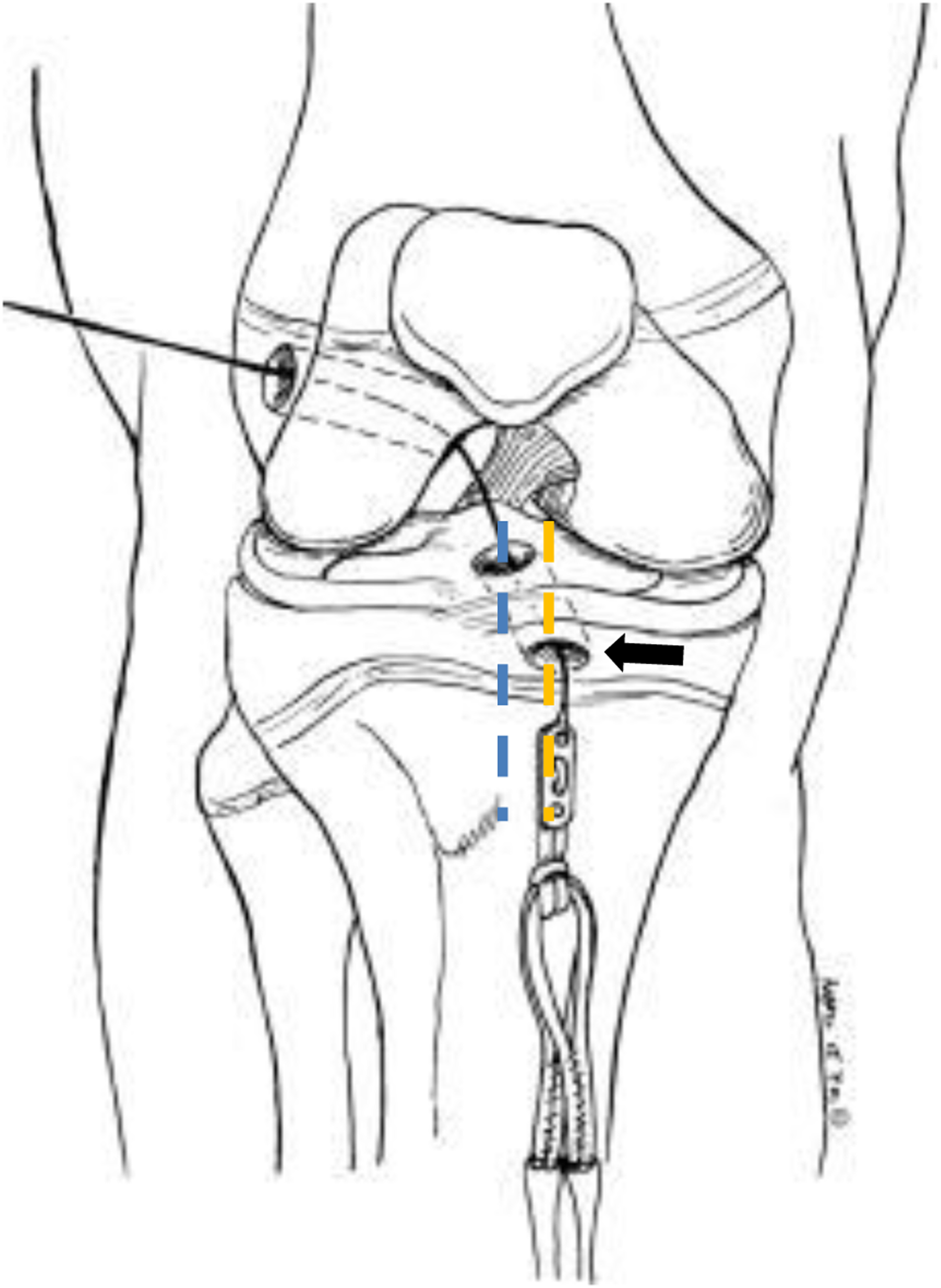
Illustration of the knee depicting an all-epiphyseal anterior cruciate ligament reconstruction. The arrow indicates the location of the entrance of the tibial tunnel at the anteromedial margin of the tibial epiphysis. The tibial tunnel follows an oblique course from medial to lateral, with the tunnel entrance (dashed yellow line) and exit (dashed blue line) located in different sagittal planes relative to the knee. Reprinted with permission from Anderson. 2

Method for selecting sagittal oblique T1-weighted magnetic resonance images (MRIs) for oblique length measurements across the tibial epiphysis. (A) Axial T1-weighted MRI showing the short and long axes of the tibial epiphysis (dashed white lines) at the level of the superior tip of the physis. The 10° (orange line) and 20° (blue line) sagittal oblique planes relative to the short axis of the tibial epiphysis at the anteromedial tibia are shown. (B) Sagittal oblique T1-weighted MRI corresponding to 10° relative to the short axis of the tibial epiphysis. (C) Sagittal oblique T1-weighted MRI corresponding to 20° relative to the short axis of the tibial epiphysis.
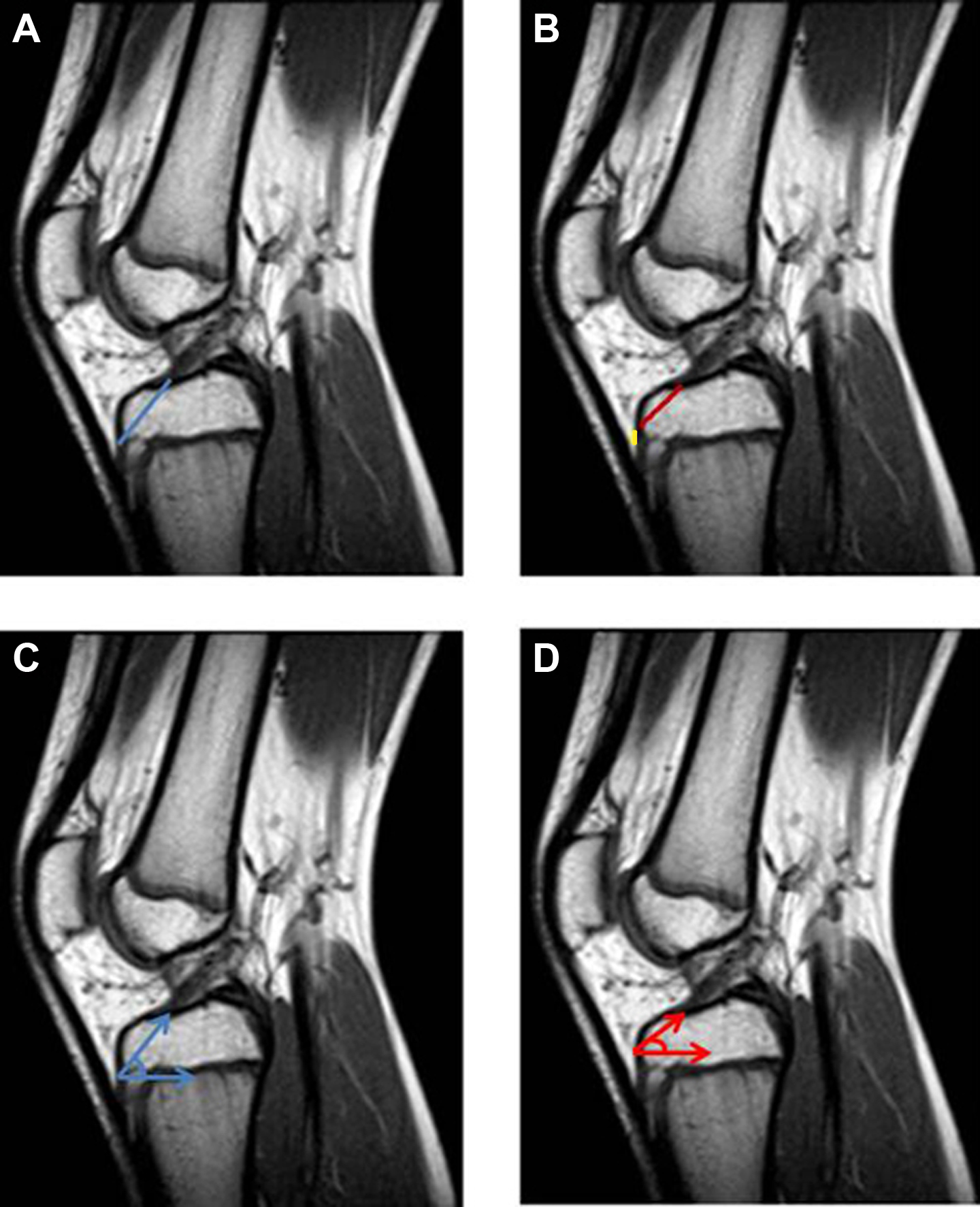
Sagittal oblique T1-weighted magnetic resonance images (MRIs) demonstrating how the oblique lengths and their corresponding angular trajectories across the tibial epiphysis were obtained. (A) Maximum oblique length, from the level of the superior tip of the tibial physis to the anterior cruciate ligament (blue line). (B) Physeal-sparing length, measured from a point 5 mm (yellow line) above the tibial physis to the anterior cruciate ligament (red line). (C) Angular trajectory corresponding to the maximum oblique length. (D) Angular trajectory corresponding to the physeal-sparing length.
Statistical analysis was performed using SPSS v22 (IBM Corp). The mean vertical height, maximum oblique length, and physeal-sparing length of the tibial epiphysis were calculated for each individual knee from the separate measurements performed by the single observer. The mean angles corresponding to the trajectories along the maximum oblique and physeal-sparing lengths of the tibial epiphysis were also calculated for each individual knee from the separate measurements performed by the single observer. Group 1 and group 2 mean measurements were compared by use of the unpaired t test. Each cohort was stratified further by sex and compared by use of the unpaired t test. The mean ages of group 1 and group 2 and the mean age by sex in each cohort were compared with the unpaired t test. A P value less than .05 was considered to indicate a significant difference. Intraobserver and interobserver agreement were assessed by calculating the intraclass correlation coefficient (ICC) according to the method proposed by Landis and Koch. 23 Pearson correlation coefficients (r) were calculated between vertical height and maximum oblique length of the tibial epiphysis at 10° and 20°. Pearson correlation coefficients were also calculated between vertical height and physeal-sparing lengths of the tibial epiphysis at 10° and 20°. No sample size calculation was performed.
Results
Group 1 (n = 36) consisted of a younger cohort of knees (64% male, 36% female) with a mean age (± SD) of 10.9 ± 0.8 years (range, 10-12 years). Group 2 (n = 59) consisted of an older cohort of knees (47% male, 53% female) with a mean age of 13.6 ± 0.9 years (range, 12-14 years). The age difference for group 1 versus group 2 was statistically significant, with a P value of less than .001. The mean vertical height of the tibial epiphysis showed no statistical difference, measuring 15.6 and 15.4 mm for the younger and older cohorts, respectively (Table 1). However, significant differences were identified between group 1 and group 2 with regard to the mean maximum oblique length at 10° and 20° (P = .009 and P = .007, respectively) and the mean physeal-sparing length at 10° and 20° (P = .004 and P = .001, respectively). The mean maximum oblique lengths for the younger cohort were 21.2 and 22.2 mm at 10° and 20°, respectively; the mean maximum oblique lengths for the older cohort were 22.7 and 23.8 mm at 10° and 20°, respectively (Table 1). The mean physeal-sparing lengths for group 1 were 18.3 and 19.4 mm at 10° and 20°, respectively. The mean physeal-sparing lengths for group 2 were 19.9 and 21.3 mm at 10° and 20°, respectively (Table 1).
Tibial Vertical Height, Oblique Length, and Angular Trajectory: Group 1 Versus Group 2 a

a Data are presented as mean ± standard deviation.
The angle corresponding to the trajectory of the maximum oblique length was significantly different between younger and older cohorts (P = .001 at 10°; P = .003 at 20°), and there were also significant differences for the angle corresponding to the trajectory of the physeal-sparing lengths when comparing the younger and older group of knees (P = .017 at 10°; P = .042 at 20°). The mean angle corresponding to the maximum oblique lengths for the younger cohort were 42.4° and 42.0° at 10° and 20°, respectively. The mean angle corresponding to maximum oblique lengths for the older cohort were 39.5° and 39.4° at 10° and 20°, respectively. The mean angle corresponding to the physeal-sparing lengths for younger cohort was 30.0° for both 10° and 20°; the mean angle corresponding to the physeal-sparing lengths for older cohort were 27.7° and 28.2° at 10° and 20°, respectively.
There were no significant differences found between female and male knees in the younger cohort (Table 2). Significant differences were identified between female and male knees in the older cohort with regard to the mean vertical height (P < .001), the mean maximum oblique length at 10° and 20° (P < .001 and P < .001, respectively), and the mean physeal-sparing length at 10° and 20° (P = .001 and .004, respectively) of the tibial epiphysis (Table 3). The mean vertical height for the older cohort of girls and boys was 14.5 and 16.5, respectively. The maximum oblique length for older girls was 21.6 and 22.7 mm at 10° and 20°, respectively. The maximum oblique length for the older boys was 24.0 and 25.0 mm at 10° and 20°, respectively. The physeal-sparing length for older girls was 18.9 and 20.3 mm at 10° and 20°, respectively. The physeal-sparing length for the older boys was 21.1 and 22.4 mm at 10° and 20°, respectively.
Tibial Vertical Height, Oblique Length, and Angular Trajectory for Group 1: Girls Versus Boys a

a Data are presented as mean ± standard deviation.
Tibial Vertical Height, Oblique Length, and Angular Trajectory for Group 2: Girls Versus Boys a

a Data are presented as mean ± standard deviation.
The mean angle corresponding to the trajectory of the physeal-sparing length was significantly different between girls and boys in the older cohort (P = .013 at 10°; P = .010 at 20°), while there were no significant differences for the mean angle corresponding to the trajectory of the maximum oblique length (Table 3). The mean angle corresponding to the physeal-sparing lengths for the older girls was 26.4° and 26.8° at 10° and 20°, respectively; the mean angle corresponding to the physeal-sparing lengths for the older boys was 29.2° and 29.7° at 10° and 20°, respectively. The mean angle corresponding to the maximum oblique lengths for the older girls was 38.7° and 38.6° at 10° and 20°, respectively; the mean angle corresponding to maximum oblique lengths for older boys was 40.4° and 40.1° at 10° and 20°, respectively.
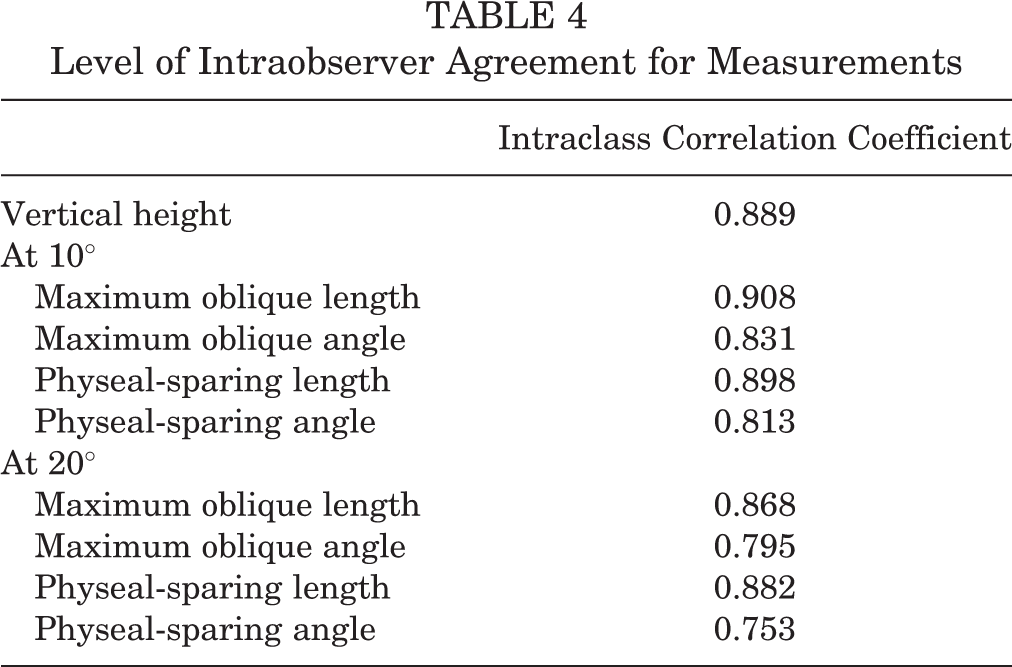
There was a strong correlation between the vertical height and maximum oblique length of the tibial epiphysis at 10° (r = 0.689, P < .001) and 20° (r = 0.632, P < .001) in the study (Figure 5). There was also strong correlation between the vertical height and physeal-sparing length of the tibial epiphysis at 10° (r = 0.655, P < .001) and 20° (r = 0.597, P < .001) (Figure 6). During this study, strong intraobserver agreement was found for all parameters. The ICC for the maximum oblique length was 0.908 and 0.868 at 10° and 20°, respectively, and 0.831 and 0.795 for the maximum oblique angle at 10° and 20°, respectively. The general measure of intraobserver agreement for all measurements is provided in Table 4. Strong interobserver agreement was found for the maximum oblique length, with an ICC of 0.821 and 0.767 at 10° and 20°, respectively. Strong interobserver agreement also was found for the physeal-sparing length at 10° and 20° (Table 5). Moderate interobserver agreement was found for maximum oblique angles, while poor to fair agreement was found for physeal-sparing angles (Table 5).

Correlation between vertical height and maximum oblique length of the tibial epiphysis at (A) 10° and (B) 20°.

Correlation between vertical height and physeal-sparing length of the tibial epiphysis at (A) 10° and (B) 20°.
Level of Intraobserver Agreement for Measurements
Level of Interobserver Agreement for Measurements

Discussion
ACL reconstruction is gaining acceptance as an early intervention for treatment of complete ACL tear in children and adolescents to restore knee stability and to avoid long-term complications of subsequent chondral and meniscal injuries. 1,2,4,15,16,30,33,37 However, opinions differ on the safety of transphyseal ACL reconstruction in skeletally immature knees. 3,5,32 Children and adolescents at greatest risk for iatrogenic growth disturbance from violation of the growth plate are those with at least 5 cm of future lower limb growth potential. 2,16,32 Long-term iatrogenic complications remain a real concern for orthopaedic surgeons, and reports of angular deformity, premature growth arrest, leg length discrepancy, and limb overgrowth have been described. 6,11,14,22,34
The development of significant growth disturbances in the skeletally immature knee have been demonstrated when ≥7% of the physeal volume is injured, raising concerns about the safety of transphyseal ACL reconstruction techniques. 27 The volume of physeal damage is proportional to the size of tunnel diameter and has been shown to increase an average of 1.1% for every additional millimeter added from 6 to 11 mm. 18 Placement of a tibial tunnel across the tibial physis has additional concerns, since growth disturbance has been shown to occur in a rabbit model with only 4% of physeal damage. 14 Preoperative planning for ACL reconstruction to avoid the growth plate is most important for young knees, since the percentage of physeal injury increases linearly relative to decreasing age. Younger prepubescent children sustain a greater percentage of physeal volume loss than older pubescent adolescents. 18 Thus, physeal-sparing techniques have been developed to avoid violation of the growth plate entirely in skeletally immature knees at greatest risk of iatrogenic growth disturbance. 2,12,15,25
Despite the intention of avoiding the growth plate, physeal-sparing ACL reconstruction techniques violate the tibial physis more frequently than previously believed by the orthopaedic community. Nawabi et al 31 studied 15 skeletally immature knees after all-epiphyseal ACL reconstruction on quantitative MRI ≤24 months postoperatively. Ten of the 15 knees demonstrated violation of the tibial physis, typically at the anteromedial region where tunnel drilling was performed. The mean volume of physeal damage for the group was 2.1%, but 2 of the knees had a physeal injury greater than 6%. 31 One factor that accounts for the greater than expected rate of tibial physeal violation is the anatomy of the proximal tibia. The tibial physis is not uniform in the axial plane along the short axis of the proximal tibia and has an undulating course between the epiphysis and metaphysis. The growth plate is convex in shape when viewed from above but is concave at the midline in the posterior central intracondylar region. 7
An important parameter for physeal-sparing ACL reconstruction at the tibia is proximity of the tibial tunnel to the growth plate. Accounting for the location of the physis near the anteromedial margin of the tibia in the exact plane of tibial tunnel course is necessary to prevent inadvertent violation of the growth plate during tunnel drilling. To avoid the physis, the tibial tunnel must be placed in a position entirely superior to the growth plate. Exact localization of the superior margin of the physis is a pitfall during fluoroscopy-guided procedures, since the 3D anatomy of the physis is masked in the 2D fluoroscopic image. Similar errors in tunnel placement are also possible during tibial tunnel placement with intraoperative computed tomography (CT) if the displayed 2D reconstructed CT image corresponds to a nearby parasagittal plane but is not in line with the exact course of tibial tunnel drilling. In our study, we included a hypothetical physeal-sparing length and its corresponding angular trajectory, in addition to the maximum oblique length and its corresponding trajectory, to provide measurements of a simulated “safe” tibial tunnel course across the tibial epiphysis. We chose to measure the physeal-sparing parameters at a distance of 5 mm above the physis with the assumption that a 6-mm drill bit would produce 3 mm of tunnel both above (superior half) and below (inferior half) the center of the drill bit, leaving a zone of at least 2 mm of epiphyseal bone between the tibial tunnel and anteromedial margin of the tibial physis. Having a zone of epiphyseal bone between the tibial tunnel and tibial physis is important, since reports of growth disturbance without direct violation of the physis also have been described in physeal-sparing ACL reconstruction in skeletally immature knees. 26 Mechanisms of injury include thermal, pressure, and mechanical effects from nearby tunnel drilling. 19,26 Clinically, our method of image postprocessing with a 3D visualization system from preoperative MRI examinations has the potential to add value to surgical planning for skeletally immature knees by forecasting the available tunnel length and proximity to the physis along the expected course of tunnel drilling.
Angular trajectory of the tibial tunnel, in addition to proximity of the tunnel to the growth plate, is another critical factor for the safety of physeal-sparing ACL reconstruction. 18,20,31 Swami et al 36 reported that the angular trajectory corresponding to the maximum oblique length across the tibial epiphysis ranged from 48.3° to 50.3° for skeletally immature knees from the chronologic ages of 10 to 14 years. Their study provided new insights into the angular trajectory of the expected course of the tibial tunnel necessary for physeal-sparing ACL reconstruction, but their methods utilized conventional 2D sagittal images that neither corresponded to the true sagittal oblique plane of an expected tibial tunnel placement nor localized the exact superior margin of the tibial physis at the anteromedial margin of the proximal tibia. 36 Angular trajectory of the tibial tunnel placement is important since this variable is associated with violation of the tibial growth plate and the safety of ACL reconstruction. 18,20 Kocher et al 20 evaluated the feasibility of tibial tunnel placement at 30°, 45°, and 60° in 4 cadaver knees, aged 7 and 12 years. They found that an angular trajectory of 30° for tibial tunnel placement was feasible in the 12-year-old knee since the tunnel course avoided the growth plate. However, their 45° and 60° tunnels violated the growth plate. 20
Our findings show that the average angular trajectory corresponding to the expected tunnel course across the tibial epiphysis is more acute than previously believed for physeal-sparing ACL reconstruction in skeletally immature knees at high and intermediate risk of iatrogenic growth disturbance. The average angle corresponding to the maximum oblique length across the tibial epiphysis was only 42° and 39° for the younger and older cohorts of knees, respectively. Also, the average angle corresponding to the physeal-sparing length was only 30° and 28° for the younger and older cohorts of knees, respectively. Our results support the previous findings of Kocher et al 20 in 12-year-old cadaver knees. Angles >40° are more prone to violate the tibial physis, and safe tunnel placement corresponds to an angular trajectory of 30°.
The maximum oblique length across the tibial epiphysis is also shorter than previously described. Swami et al 36 reported an average distance of 30 mm for knees from 11 to 15 years of age. We identified a maximum average length across the tibial epiphysis of only 22.2 mm for the younger cohort and 23.8 mm for the older cohort. Our average physeal-sparing lengths, corresponding to a “safe” tunnel placement, were only 19.4 and 21.3 mm for the younger and older cohorts, respectively. These distances have major ramifications for physeal-sparing ACL reconstruction across the tibial epiphysis. Physeal-sparing lengths of <18 mm were not uncommon in our study, as physeal-sparing lengths between 15 and 17 mm represented 17% and 10% of knees in the younger and older cohorts, respectively. Thus, procedures that require a minimum of 20 mm or more for placement of an interference screw may not be possible without violation of the growth plate in all skeletally immature knees at high and intermediate risk for iatrogenic growth disturbance. 25 Kercher et al 18 studied tibial tunnel angular trajectories on 3D MRI models in 31 skeletally immature knees, aged 10 to 15 years, corresponding to a minimum tibial tunnel length of ≥20 mm. Their simulations of tibial tunnel angle ranged from 40° to 85° (mean, 65°). As the tibial tunnel angle increases, the risk of violation of the growth plate is greater in physeal-sparing ACL reconstruction.
Our study found significant differences between the younger prepubescent and older adolescent knees for maximum oblique length, physeal-sparing length, and angular trajectory corresponding to the physeal-sparing length across the tibial epiphysis. Prepubescent knees are more diminutive in size and present a smaller margin for error during physeal-sparing ACL reconstruction. We also found sex-related differences among knees, similar to previous studies. 9,36 Adolescent female knees are smaller than their male counterparts, with a significant difference existing between sexes for vertical height, maximum oblique length, physeal sparing length, and angular trajectory corresponding to the physeal-sparing length across the tibial epiphysis. We also demonstrated that a strong correlation exists in our population of skeletally immature knees between the vertical height and maximum oblique length of the tibial epiphysis as well as between the vertical height and physeal sparing length of the tibial epiphysis.
Although statistically significant differences for tunnel lengths and angles were shown to exist between the younger and older cohorts of knees, and also between boys and girls, the amount of difference between these groups may lack clinical significance for immature knees requiring a physeal-sparing ACL reconstruction. In current clinical practice, differences of 1 to 2 mm or 2° to 5° may have limited impact on preoperative clinical decision making or surgical approach in the operating room.
The limitations of this study include the retrospective nature of the methods. Knee MRI examinations were identified by a search of our hospital PACS without regard for clinical history or physical examination findings. Also, knees were evaluated by chronological age, and no prospective correlation with skeletal age or sexual maturity was performed. Future studies addressing skeletal age will be necessary. An analysis comparing males and females of equal size was not performed since the weight and height of study participants was unknown. Future studies will be necessary to determine whether sex differences exist for knees between boys and girls of equal size. In addition, no analysis of variance was performed, which is a limitation for identification of possible confounding factors among the study variables. Another limitation was the use of different MRI scanners at our hospital center. However, the imaging protocols in the study were similar with regard to sequences acquired and slice thickness.
Conclusion
We found that the average oblique length across the tibial epiphysis in the prepubescent knee associated with a “safe” physeal-sparing ACL reconstruction, without concern for violation of the growth plate, was approximately 19 mm, with a corresponding average angular trajectory of approximately 30°. The average “safe” oblique length across the tibial epiphysis in adolescent knees at intermediate risk for iatrogenic growth disturbance was approximately 21 mm, with a corresponding angular trajectory of approximately 28°. The differences between our younger and older cohorts of skeletally immature knees for the maximum and “safe” oblique lengths across the tibial epiphysis were statistically significant, although the small difference between these groups may lack clinical significance. Additionally, adolescent girls at intermediate risk for iatrogenic growth disturbance after physeal-sparing ACL reconstruction have significantly shorter maximum and “safe” oblique lengths across the tibial epiphysis as compared with boys.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.