
Abstract
Background:
Despite growing evidence on the role of the posterior ulnar collateral ligament (pUCL) in elbow stability, current ligament bracing techniques are mainly focused on the anterior ulnar collateral ligament (aUCL). A dual-bracing technique combines the repair of the pUCL and aUCL with a suture augmentation of both bundles.
Purpose:
To biomechanically assess a dual-bracing approach addressing aUCL and pUCL for humeral-sided complete UCL lesions to restore medial elbow laxity without overconstraining.
Study Design:
Controlled laboratory study.
Methods:
A total of 21 unpaired human elbows (11 right, 10 left; 57.19 ± 11.7 years) were randomized into 3 groups to compare dual bracing with aUCL suture augmentation and aUCL graft reconstruction. Laxity testing was performed with 25 N applied 12 cm distal to the elbow joint for 30 seconds at randomized flexion angles (0°, 30°, 60°, 90°, and 120°) for the native condition and then for each surgical technique. A calibrated motion capture system was used for assessment, allowing the 3-dimensional displacement during the complete valgus stress cycle between the optical trackers to be quantified as joint gap and laxity. The repaired constructs were then cyclically tested through a materials testing machine starting with 20 N for 200 cycles at a rate of 0.5 Hz. The load was increased stepwise by 10 N for 200 cycles until displacement reached 5.0 mm or complete failure occurred.
Results:
Dual bracing and aUCL bracing resulted in significantly (P = .045) less joint gapping at 120° of flexion compared with aUCL reconstruction. No significant differences in valgus laxity were found among the surgical techniques. Within each technique, there were no significant differences between the native and the postoperative state in valgus laxity and joint gapping. No significant differences between the techniques were observed in cycles to failure and failure load.
Conclusion:
Dual bracing restored native valgus joint laxity and medial joint gapping without overconstraining and provided similar primary stability regarding failure outcomes as established techniques. Furthermore, it was able to restore joint gapping in 120° of flexion significantly better than aUCL reconstruction.
Clinical Relevance:
This study provides biomechanical data on the dual-bracing approach that may help surgeons to consider this new method of addressing acute humeral UCL lesions.
Keywords
In the past, the posterior ulnar collateral ligament (pUCL) had not been regarded as biomechanically relevant in elbow dislocation injuries, 2 although current studies strongly support its role in elbow stability. 13,16,22,26,28 –30 In addition to these biomechanical findings, recent clinical and radiological observations confirmed that injury to the UCL can also occur because of acute isolated valgus trauma to the elbow. 7,23,27 Acute UCL injuries through an isolated valgus mechanism result in complete avulsions from the medial humeral epicondyle in a sleeve-like fashion in most of the cases. 23 A sufficient surgical treatment of the injured pUCL as well as anterior UCL (aUCL) would need to restore valgus as well as posteromedial stability.
Ligament bracing through suture augmentation of the medial collateral ligament of the elbow has been recently introduced and investigated in multiple studies. 4,11,17,18,32 However, these bracing techniques are mainly focused on the aUCL. 4,11,17,18,32 Dual bracing that fixes the ruptured pUCL as well as aUCL would allow simultaneous reattachment of the complete avulsed UCL at its humeral insertions. Furthermore, both injured UCLs are augmented along their anatomic course. Consequently, the dual-bracing technique bears the potential for higher primary stability throughout the complete range of motion because of an augmented posterior bundle. Therefore, the surgical treatment of elbow dislocations that affect the medial stabilizers would be optimized by this technique.
However, there might be concern when multiple bundles of flat braided polyethylene/polyester suture with a higher rigidity than the native tissue or a tendon graft are applied to re-create UCL function. Overconstraining of the medial elbow compartment after addressing the UCL has been biomechanically observed. 32 This could result in elevated joint pressure and might ultimately lead to earlier onset of joint degeneration. So far, only a reconstruction of the pUCL with a graft has been evaluated in scenarios with associated coronoid fractures. 13,31 A biomechanical evaluation of a dual-bracing technique addressing the complete UCL has, to the best of our literature research, not been widely described. When performing a biomechanical assessment of the introduced dual-bracing technique, which takes over the function of the pUCL as well as the aUCL, it should be initially clarified that this new surgical technique is able to re-create valgus stability as efficiently as established techniques and that it does not lead to overconstraining of the medial compartment of the elbow.
The purpose of the present study was to biomechanically compare dual bracing with aUCL ligament bracing as well as with aUCL reconstruction. The aim of this initial evaluation was to clarify the effect of dual bracing on valgus stability as well as laxity in order to assess a possible overconstraining. It was hypothesized that equal biomechanical properties are present in the newly developed dual-bracing technique compared with aUCL bracing and aUCL reconstruction.
Methods
The study protocol was considered exempt from institutional review board approval. A total of 21 unpaired, fresh-frozen human cadaveric elbows (8 male, 13 female; 11 right, 10 left; mean [± SD] age, 57.19 ± 11.7 years) were used in this study. All specimens were obtained from Science Care. The specimens were randomized into 3 groups according to surgical procedure: dual bracing, aUCL bracing, or aUCL reconstruction.
Before testing, the bone mineral density (BMD) of a 1 × 1–cm section at the proximal ulna in the area of the sublime tubercle was determined in a lateral view for all specimens (GE Lunar Prodigy; GE Healthcare) to exclude differences between repair groups. Additionally, each specimen was visually and radiographically assessed for osteoarthritis and soft tissue damage.
Fresh-frozen cadaveric elbows were thoroughly dissected, leaving only medial and lateral static elbow stabilizers and joint capsule intact. 8 Before this, the palmaris longus tendon was harvested in every specimen when present. 24 The tendons were collected and stored in a freezer at –20°C. The palmaris longus tendon was randomly used for specimens that were allocated to the reconstruction technique. Specimen randomization was independent of palmaris longus presence. Humeri as well as radii and ulnas were transected at the mid-diaphysis with a handsaw and secured in neutral pronosupination of the forearm with a 1.5 inch–diameter polyvinyl chloride pipe by Bosworth Duz-All self-curing acrylic cement (Harry J. Bosworth). After dissection and potting, the specimens were stored in a freezer at –20°C. After a period of 24 hours prior to biomechanical testing, the specimens were thawed at room temperature.
In both setups applied for the biomechanical assessment, each specimen was mounted horizontally in a customized mount, allowing orientation of the medial side superiorly. The humerus was aligned parallel to the ground 4 and the ulnohumeral joint axis perpendicular to the humerus. To preclude any bias to the valgus laxity through changes of the specimens’ mount, the initial humeral attachment of the specimen was kept throughout testing. Furthermore, the surgery was performed while the humerus remained attached to the mount. Before testing, the specimens were cycled 5 times in their free range of motion. After evaluation of the native condition, complete humeral detachment of the medial UCL through dissection was performed. This re-created a sleeve-like UCL injury at the medial humeral epicondyle as observed after valgus trauma to the elbow. 23 Then the surgical procedure according to a priori randomization was performed, and the testing was repeated for the postoperative state.
Surgical Procedures
Single Bracing of the aUCL
The humeral detached aUCL was stitched with a Krakow pattern of nonabsorbable suture (No. 2 FiberWire, Arthrex) and reattached to the center of the native humeral aUCL footprint by using a 3.5-mm anchor (SwiveLock, Arthrex) that was loaded with the suture limbs fixing the aUCL fibers, as well as an additional 2-mm flat braided nonabsorbable suture (FiberTape, Arthrex) 11 (Figure 1A). At the apex of the sublime tubercle, the free end of the flat braided suture was loaded into a second 3.5-mm anchor and inserted with the same tension as the underlying aUCL into the ulna 11 (Figure 1B). This was performed while the joint was reduced with slight, continuous varus pressure at 20° of elbow flexion. 11 While the aUCL was reattached to the humerus (Figure 1A), the pUCL fibers were not addressed and were left untreated (Figure 1C).

(A) An anchor loaded with an additional suture tape and suture limbs fixing the anterior ulnar collateral ligament (aUCL) fibers was placed at the native humeral aUCL footprint. (B) The free end of the suture tape was loaded into a second anchor and inserted at the sublime tubercle, (C) while the posterior ulnar collateral ligament remained untreated.
Dual Bracing of the UCL
The humeral detached aUCL and pUCL were each stitched with a Krakow pattern of nonabsorbable suture (No. 2 FiberWire). They were both loaded to one 4.75-mm anchor (SwiveLock) with an additional flat braided nonabsorbable suture. The anchor was fixed caudally to the medial epicondyle to reach an anatomic fixation of the aUCL as well as pUCL at their native humeral footprints (Figure 2A). Then, each of the free suture tape ends were aligned to follow the course of the aUCL or pUCL to their insertion at the ulna. The free suture tape end bracing the aUCL was fixed at the sublime tubercle by using a 3.5-mm anchor in 20° of flexion (Figure 2B). Similarly, the bracing suture tape end for the pUCL was fixed in full flexion underneath the sublime tubercle at the center of the ulnar pUCL insertion (Figure 2C). Each anchor loaded with a bracing suture limb was inserted into the ulna with the same tension as the underlying ligament tissue, while the joint was reduced with slight, continuous varus pressure.

(A) The aUCL and pUCL were both reattached close to their anatomic insertions at the ulnar humeral epicondyle with 1 anchor. (B) One limb of the additionally loaded suture tape followed the course of the aUCL and was fixed in 20° of flexion at the sublime tubercle. (C) The other suture tape limb was fixed similarly in full flexion at the center of the ulnar pUCL insertion. aUCL, anterior ulnar collateral ligament; pUCL, posterior ulnar collateral ligament.
Reconstruction of the aUCL
Converging 3.5-mm drill tunnels were positioned 1 cm apart at the sublime tubercle of the ulna and at the medial epicondyle of the humerus 11 (Figure 3, A and B). A palmaris longus tendon was first shuttled through the ulnar tunnel and then through the humeral tunnels as described by Dugas et al 11 (Figure 3C). The joint was reduced with varus pressure at 20° of elbow flexion, and both limbs were crossed as well as tensioned while the limbs were securely sutured (No. 2 FiberWire) together over the epicondyle 11 (Figure 3D). Additional sutures were passed around the ligament and tendon reconstruction to incorporate them together 11 (Figure 3D).
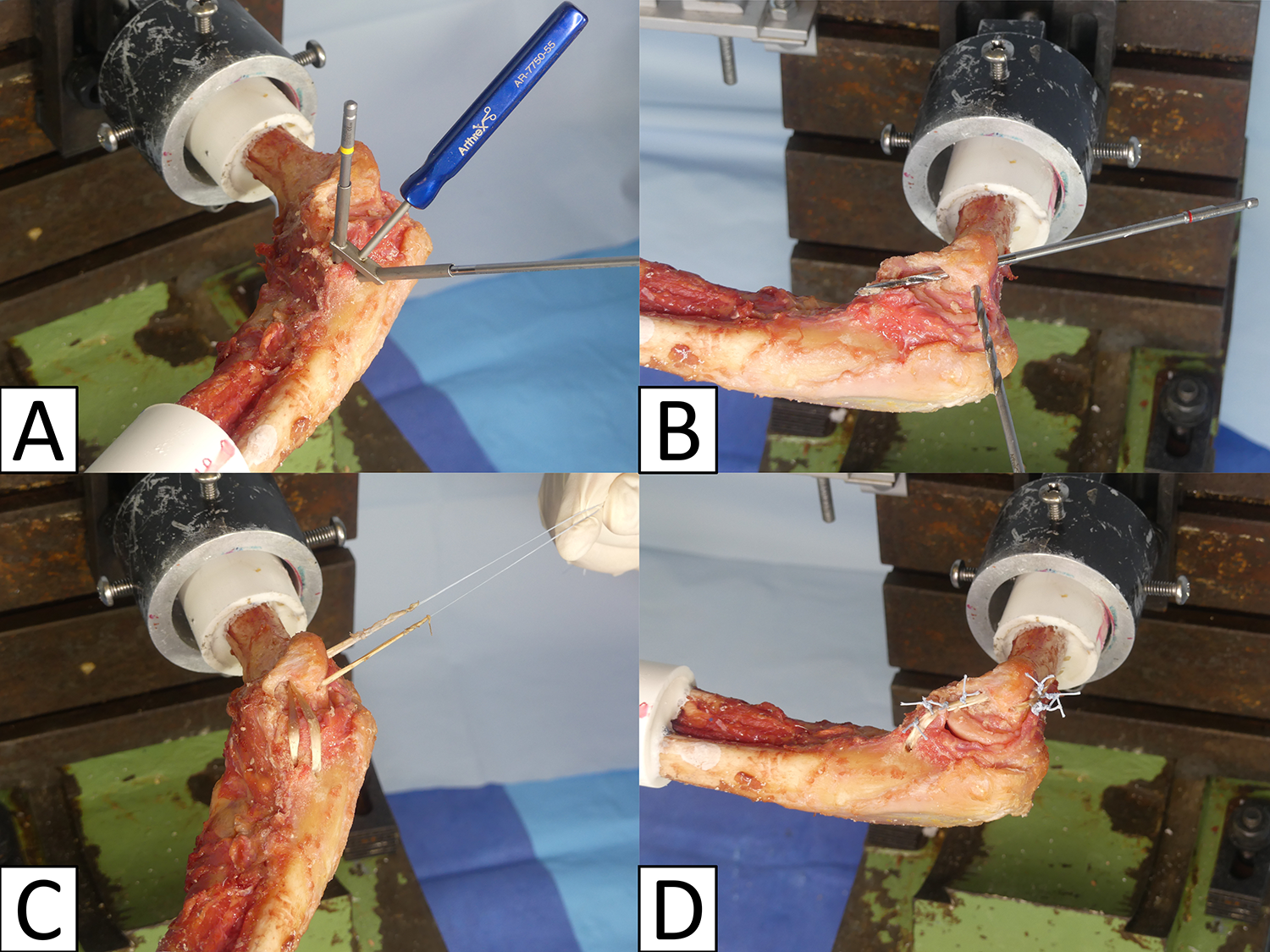
(A) Two converging drill tunnels (V shape) were created 1 cm apart from each other at the sublime tubercle. (B) At the medial epicondyle, 2 converging drill tunnels (Y shape) were established with a 1-cm bridge. (C) The palmaris longus graft was passed through tunnels, and (D) the tendon limbs were securely sutured together.
To achieve the same tension as the native medial UCLs, each surgical technique had to resist the gravitational valgus at the same height level as the native state in the applied horizontal mount. For each specimen, the height of the distal ulna with the medial UCLs intact because of the gravitational valgus was documented as well as marked for the corresponding joint position relevant to the surgical procedure. For each surgical technique, it was ensured that each specimen had no slack in its constructs and that the distal ulna was at the same horizontal level as in native gravitational valgus.
Valgus Joint Laxity Testing
The setup was adapted from prior biomechanical studies evaluating the UCL of the elbow, allowing 5 degrees of freedom while constraining only the flexion angle. 1,8,15,32 The elbow was aligned with the medial side to the top and the humerus parallel to the ground to apply valgus stress 4 (Figure 4A). A force of 25 N was applied 12 cm distal to the anatomic axis of rotation of the elbow to achieve a 3.0-N·m moment at the joint as described in a previous biomechanical study 8 (Figure 4, A and B). The weight was applied for 30 seconds at randomized elbow flexion angle positions of 0°, 30°, 60°, 90°, and 120°. 8,32 After laxity testing of the intact condition, the humeral attachments of the UCL were released from the humeral epicondyle. The laxity test protocol was repeated after surgical procedures.

Biomechanical setup for (A and B) valgus joint laxity and (C) failure load interval. Arrows indicate applied force.
A calibrated motion capture system with 4 infrared cameras (Vero Version 1.3; Vicon) documented the 3-dimensional displacement during the complete test cycle of valgus stress between the optical trackers (Figure 4A). The optical trackers were securely fixed to the medial side of the ulna as well as the humerus by Steinman pins, with parallel alignment to the anatomic axis of the ulna and humerus, respectively (Figure 4, A and B). The infrared cameras operated at a frame rate of 250 Hz with a positioning accuracy of 0.01 mm and 0.1°. The collected data were processed with a motion analysis software (ProCalc; Vicon), and measurements were compared with the initial native status as well as between the surgical techniques. Three measurement runs were performed for each evaluated flexion angle, and the resulting means for valgus angle and joint gapping were statistically processed.
Evaluation for Failure
Valgus loading was applied to the ulna 12 cm distal to the anatomic axis of rotation of the elbow 3 through a materials testing machine (Bionix 858; MTS Systems) to test each surgical technique (Figure 4C). For this evaluation, the elbow was aligned with the medial side to the top in 90° of flexion 3,8 (Figure 4C). A beginning load of 20 N, applied for 200 cycles with a rate of 0.5 Hz, was increased by steps of 10 N for 200 cycles until 5.0-mm displacement was detected or complete failure was observed. 3,8 The peak failure load interval as well as cycles to failure were documented, and measurements were statistically compared between all techniques.
Statistical Analysis
Sample size calculation was carried out a priori using estimates from the literature. 3 For load to failure, a common standard deviation of 10 N was assumed. A sample size of 7 per group would provide 80% power to detect a 20-N difference in load to failure between the groups at an alpha level of .05. Outcome data were assessed for normality by evaluation of their distributions. Given the skewed distributions, the nonparametric Wilcoxon test and Mann-Whitney U test were used to determine whether a statistically significant difference between the native and the postoperative state, as well as among the surgical techniques, was present. A post hoc adjustment for multiple testing was applied according to Bonferroni-Holm. Statistical analysis was performed with SPSS Version 26 (IBM).
Results
The mean BMD (0.94 ± 0.27 vs 0.97 ± 0.28 vs 0.91 ± 0.26 g/cm2) and mean age (55.29 ± 12.58 vs 60.86 ± 9.95 vs 55.43 ± 11.60 years) were not significantly different between specimens treated with either dual bracing, aUCL bracing, or aUCL reconstruction.
Given the stiffness of the elbow joint capsule, full extension was not possible to achieve in every specimen for each surgical group (aUCL brace, n = 2; dual bracing, n = 4; aUCL reconstruction, n = 4). Consequently, the evaluation at full extension could not be performed and was continued at 30° of flexion and beyond for the native and postoperative states.
Throughout the evaluated joint positions, native and postoperative valgus laxity showed no significant differences for each type of surgical repair (Figure 5, A-C), and aUCL bracing, dual bracing, and aUCL reconstruction showed no significant differences when compared with each other (Figure 5D).

Comparison of valgus laxity (A-C) for each surgical technique compared with the native state and (D) between techniques. aUCL, anterior ulnar collateral ligament; n.s., not significant.
Gapping of the native and the repaired joint showed no significant differences for each surgical technique (Figure 6, A-C). However, dual bracing and aUCL bracing showed significantly (P = .045) less joint gapping in 120° of flexion as compared with aUCL reconstruction (Figure 6D). In the remaining flexion angles, no significant differences for joint gapping were observed between aUCL bracing, dual bracing, and aUCL reconstruction.

Comparison of joint gapping (A-C) for each surgical technique compared with the native state and (D) between techniques. aUCL, anterior ulnar collateral ligament; n.s., not significant.
There were no significant differences among aUCL bracing, dual bracing, or aUCL reconstruction for cycles to failure (mean, 1051.29 ± 590.04 vs 1040.86 ± 298.04 vs 809.86 ± 543.29) and failure load (mean, 68.57 ± 28.50 vs 68.57 ± 15.52 vs 57.14 ± 30.10 N) (Figure 7, A and B). No complete failures were observed during testing.
Between specimens with extension deficit and specimens with free range of motion, there were no significant differences in any of the parameters.

Comparison of (A) number of cycles until failure and (B) failure load cycles between specimens of each surgical technique. aUCL, anterior ulnar collateral ligament; n.s., nonsignificant.
Discussion
The most important finding of this biomechanical evaluation was that dual bracing of the UCL was able to restore the native valgus laxity of the elbow joint. Consequently, no signs of overconstraining after dual bracing by augmenting aUCL as well as pUCL with flat braided nonresorbable suture were present. Furthermore, no significant differences for valgus laxity and failure outcomes were observed in comparison with the established surgical techniques of aUCL bracing and reconstruction. Additionally, dual bracing was able to restore joint gapping significantly better than aUCL reconstruction in 120° of elbow flexion.
Ligament bracing of the medial UCL of the elbow has been previously described, but these techniques have been focused on the aUCL. 11,17,32 However, recent clinical and biomechanical investigations support the importance of the pUCL in elbow stability. 13,22,26,28 –31 Especially in the setting of a coronoid fracture, the high relevance of the pUCL on posteromedial rotatory instability (PMRI) has been observed. 13,31 As suggested by Sard et al, 26 the authors strongly support addressing the pUCL when complete injury to the UCL occurs.
Bodendorfer et al 4 found no significant difference for valgus opening between aUCL bracing and aUCL reconstruction. When comparing modified aUCL bracing to aUCL reconstruction, Urch et al 32 observed restoration to the intact state for all evaluated flexion angles. Whereas aUCL reconstruction could only restore native valgus laxity at 60° of flexion, it led to significant overconstraining at 90° as well as 120° of flexion and failed to restore native valgus laxity at full extension and 30° of flexion. 32 In the current study, there was no significant difference between both bracing techniques, which indicates that dual bracing might be as efficient as aUCL bracing in restoring valgus laxity.
Dugas et al 11 also biomechanically compared aUCL reconstruction and aUCL bracing. Ligament bracing of the aUCL led to a significantly lower joint gapping than the reconstruction of the aUCL. In particular, aUCL bracing was able to significantly reduce joint gapping compared with the torn condition. 11 Jones et al 17 observed a significantly lower joint gapping after surgical treatment when comparing aUCL bracing with aUCL reconstruction as well. With consideration of the observed joint gapping behavior after aUCL bracing 11,17 and the current findings, dual bracing of the UCL can be considered an equivalent technique to aUCL bracing for restoring native joint gapping.
Previous studies have observed no significant difference between aUCL reconstruction and aUCL bracing when comparing torque, stiffness, and gapping at failure. 4,11,17 However, Urch et al 32 observed a significantly higher torque at failure for aUCL reconstruction, when compared with aUCL bracing. If the current observations and the findings of prior biomechanical studies 4,11,17 are considered, dual bracing represents a surgical alternative that shows equal primary stability compared with aUCL bracing and aUCL reconstruction.
From a clinical perspective, dual bracing might allow us to better re-create the anatomy and re-establish elbow stability, which is very important in particular for upper extremity athletes. Here, throwing athletes who rely on joint stability throughout the complete range of motion, especially in higher flexion, could benefit. Based on the observations from prior biomechanical studies, 13,31 an even higher effect by restoring the pUCL function can be expected when the coronoid process is fractured. In this setting, the additional reconstruction of the pUCL with a graft has already biomechanically proven to be able to reduce PMRI. 13,31 By addressing both relevant ligamentous stabilizers of the medial elbow—the aUCL and pUCL—dual bracing bears great potential to lead to an equal restoration of posteromedial rotational stability. Because of the high primary stability of the suture tape applied for dual bracing, without the need for healing of a tendon graft in bone tunnels, an accelerated rehabilitation protocol and return to play could be considered. This might help the patient to return to activity earlier and sequelae related to postoperative immobilization could be avoided. Under consideration of these potential clinical benefits, dual bracing might be especially interesting for surgeons treating patients with higher physical demands. However, the present study can only directly answer to the observations for valgus stress at time zero.
Overconstraining of the medial elbow compartment by applying ligament bracing can be an undesired consequence resulting in permanent stress shielding to the UCL. 32 This has the potential to lead to altered biomechanics with increased joint pressure at the medial compartment of the elbow. However, the introduced dual-bracing technique showed equal laxity and joint gapping when compared with the native state. Consequently, the risk for overconstraining to the medial elbow compartment might be negligible for the dual-bracing technique, despite the rigidity of the applied suture material.
Limitations and Strengths
There are limitations to this biomechanical study. In all 3 groups, not all the evaluated specimens were assessed in full extension because of capsular stiffness. Osteoarthritis had been visually and radiographically excluded for each specimen. Consequently, the current observations for full extension between the groups are confounded by these reduced sample sizes. However, in full extension osseous stability is enhanced when the tip of the olecranon engages into the olecranon fossa, 5,9,25 and the influence of the capsuloligamentous complex on elbow stability might be not as relevant as in higher flexion angles. Comparable variations in specimens’ range of motion affecting full extension have been reported earlier as well. 6 The complete humeral-sided cut of the aUCL and the pUCL to simulate a humeral avulsion injury resulted in a high degree of valgus instability that was not verifiable. In detail, the applied force of 25 N led to such a deflection of the ulna that the attached 3-dimensional marker was moved out of the measuring scope of the Vicon system. Nevertheless, the authors believe that the comparison between the repair state and the native condition provides important data. Especially when evaluating for overconstraining of the medial elbow compartment, the comparison between the repair state and the native condition is of higher importance than comparing an insufficient state with the repair state. Another limitation of the current study is that the observations were performed at time zero without the influence of the dynamic stabilizers of the elbow. 10,12,14
Nevertheless, this study has several strengths. The biomechanical setup has been validated in prior studies evaluating the UCL of the elbow, and the valgus laxity setup in particular allowed 5 degrees of freedom while constraining only the flexion angle. 1,15,32 BMD assessment was performed using a standardized method that allows accurate measurement with minimal measurement inaccuracy at the sublime tubercle, which is an ulnar site relevant to surgical intervention. 1,11,17,18,32 We consider the area of the sublime tubercle to be less prone to measurement error than the medial epicondyle of the distal humerus. Because of the close proximity of the medial epicondyle to the olecranon fossa and the humeral trochlea, we believe that creating an area of 1 cm2 at the distal humerus will not provide accurate measurements in either a lateral or anteroposterior view. In addition, the anteroposterior view may be affected by the superposition of the olecranon, leading to erroneous values. Consequently, BMD assessment was performed strictly without superposition of the radius in an adapted lateral view at the sublime tubercle to ensure standardized comparison between specimens. Moreover, a precise optical tracking system allowing positioning accuracy of 0.01 mm and 0.1° was used, which has been validated in prior studies 19 –21 and has already been used for evaluation of the elbow. 13,30,31 Furthermore, the introduced ligament bracing technique avoids the need for a tendon graft. This is especially helpful if an autologous graft (palmaris longus or gracilis tendon) is not harvestable or allografts are not available.
In addition, the current biomechanical data on combined ligament bracing of both the posterior and the anterior UCLs, with particular emphasis on valgus joint laxity, have not been widely described. This study critically examined the potential risk of overconstraining the medial compartment with this procedure, which has also been observed biomechanically with UCL reconstruction using a tendon graft. Concerns could be raised if multiple bundles of flat braided polyethylene/polyester sutures, which are stiffer than native tissue or a tendon graft, are used to reconstruct both the posterior and the anterior UCLs. The current results showed that the evaluated technique of dual-ligament bracing does not lead to overconstraining of the medial compartment of the elbow. These findings add relevant information to the current literature and may assist surgeons in the surgical management of both the posterior and anterior UCLs in humeral avulsion injuries.
Conclusion
Dual bracing of the UCL restored native valgus joint laxity and medial joint gapping without overconstraining. Dual bracing provided similar primary stability regarding failure outcomes as established techniques. Furthermore, it was able to restore joint gapping in 120° of flexion significantly better than aUCL reconstruction. Further clinical research is needed to clarify the impact of dual bracing of the UCL on better restoring posteromedial rotatory stability.
Footnotes
Final revision submitted January 29, 2023; accepted February 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The University of Connecticut Health Center/UConn Musculoskeletal Institute receives funding from Arthrex. The company had no influence on study design, data collection, or interpretation of the results or the final manuscript. A.O. has received material support from Arthrex. A.B.I. has received personal fees outside the submitted work from Arthrex, Medi, and Arthrosurface. A.D.M. has received grant support from Arthrex. S.S. has received personal fees from Arthrex, Martin, and Medartis. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by UConn Health.