
Abstract
Background:
Ulnar collateral ligament (UCL) injury is a common sports injury among overhead-throwing athletes and causes medial elbow pain and instability. UCL injury is generally diagnosed based on symptoms, physical findings, and image evaluation. To standardize the method for evaluating elbow valgus instability, more information is needed regarding changes in the medial elbow joint space (JS) in healthy elbows.
Purpose/Hypothesis:
The purpose of this study was to measure the JS during the application of elbow valgus stress at different elbow flexion angles and loads and to clarify the presence of defensive muscle contractions during elbow valgus stress. It was hypothesized that the JS will differ according to different limb positions and loads and that defensive contractions will occur when elbow valgus stress is >90 N.
Study Design:
Controlled laboratory study.
Methods:
Elbow joints on the nondominant side were examined in 20 healthy male university students (mean age, 21 ± 0.2 years) at 30°, 60°, and 90° of elbow flexion. To create valgus stress on the elbow, loads of 30, 60, 90, 120, and 150 N were applied with a Telos stress device and with gravity stress on the forearm. The medial JS was measured ultrasonographically during the application of elbow valgus stress. Electrodes were attached to the pronator teres muscle, and defensive muscle contractions were measured using electromyography during the application of elbow valgus stress. Repeated-measures analysis of variance and paired t tests were used to compare the JS at each elbow angle and each valgus stress load, and the Bonferroni method was used as a post hoc test.
Results:
At 30° of elbow flexion, the JS was significantly higher at 30 N versus 0 N and at 60 N versus 0 or 30 N (P ≤ .018 for all). At 60° of flexion, the JS was significantly higher at 30 N versus 0 N, at 60 N versus 0 and 30 N, and at 90 N versus 0, 30, and 60 N (P ≤ .024 for all). At 90° of elbow flexion, the JS was significantly higher at 30 N versus 0 N and at 60 N versus 0 and 30 N (P ≤ .028 for all). Defensive muscle contraction did not occur at any elbow flexion angles at elbow valgus stress ≤60 N.
Conclusion:
The lack of muscular contraction at elbow valgus stress ≤60 N may reflect the function of the medial collateral ligament.
Clinical Relevance:
Elbow valgus stress ≤60 N allows for the evaluation of the joint opening.
Ulnar collateral ligament (UCL) injury is a common sports injury among overhead-throwing athletes and causes medial elbow pain and instability. 19 UCL injury is generally diagnosed based on symptoms, physical findings, and image evaluation. Among the various diagnostic imaging modalities available, qualitative evaluation of the UCL by magnetic resonance imaging (MRI) is considered the widely used imaging tool. 12 However, MRI is a static image evaluation method and cannot evaluate elbow valgus instability dynamically. Ultrasonography allows not only direct visualization of the UCL but also observation of the medial elbow joint space (JS) during elbow valgus stress to identify elbow valgus instability. Ultrasound is thus a useful modality that allows dynamic evaluations. 4
In the evaluation of elbow valgus instability, the JS can be measured when elbow valgus stress is applied using a Telos stress device 2,4,6,8,9,21 or with gravity stress on the forearm. 9,10,20,23 Regarding the measured limb positions, it is important to be able to evaluate elbow valgus instability in elbow flexion angles of 60° to 90° (representing the late cocking phase to acceleration phase, where elbow valgus stress is most applied during pitching). 5 However, when using the Telos properly, performing evaluations at angles of elbow flexion exceeding 60° is difficult. 4 Furthermore, since the UCL is the main stabilizer during elbow valgus stress with 30° of elbow flexion, 4,15 the Telos method is most commonly used in 30° of elbow flexion 2,4,6,21 and is also performed with elbow flexion angles of 25° 8 or 60°. 9 Conversely, in the method using gravity stress on the forearm, elbow flexion of 90° 10,20 is the most common, along with elbow flexion of 30° 23 or 60°. 9 In addition, loads of 50 N, 9 69 N, 6 130 N, 21 150 N, 2,4,8 and gravity stress 9,10,20,23 have been reported to show elbow valgus stress. To standardize the method for evaluating elbow valgus instability, changes in JS during elbow valgus stress applied in different limb positions and loads in normal elbows need to be clarified.
In setting the load to elucidate elbow valgus stress, factors that affect JS must be considered. A previous study reported that patients with UCL injury showed a smaller JS in the injured elbow than in the uninjured elbow when 150 N of elbow valgus stress was applied. 2 Defensive contraction due to pain may be one such factor affecting the JS. 2 Otoshi et al 17 measured the JS on ultrasound during the application of elbow valgus stress and reported that JS decreased with the contraction of the forearm and finger flexor muscles. Given such findings, the JS may be reduced when defensive contraction of the forearm and finger flexor muscles occurs if pain is experienced during excessive elbow valgus stress. Evaluation of elbow valgus instability as a means of reflecting the function of the UCL would thus require using a load that does not cause defensive contraction.
The purpose of this study was to measure the JS opening during the application of elbow valgus stress at different elbow flexion angles and loads and to clarify the presence of defensive muscle contractions during elbow valgus stress. We hypothesized that the JS will differ according to different limb positions and loads and that defensive contractions will occur when elbow valgus stress is >90 N.
Methods
Study Participants
Included in this study were 20 healthy male university students (mean age, 21 ± 0.2 years; height, 170.5 ± 5.9 cm; weight, 63.6 ± 7.0 kg). We used the elbow joint on the nondominant hand for all measurements. Exclusion criteria were a history of orthopaedic disease in the elbow joint or elbow joint pain at the time of measurement. Handedness was confirmed using the Edinburgh handedness inventory. 16
This study was carried out with the approval of the university ethics review committee and was conducted in accordance with the Declaration of Helsinki. All participants provided informed consent before enrollment.
Measurement of Medial Elbow JS
All measurements were made by the same physical therapist (M.E.) and B-mode ultrasonography (Aplio 500; Toshiba Medical Systems) with a 4.8-cm linear probe (12 MHz; PLT-1204BT; Toshiba Medical Systems) was used for all measurements. With reference to a study by Ciccotti et al, 4 the ultrasound probe was applied to the medial side of the elbow joint, and the anterior bundle of the UCL was visualized using the humeral trochlea and ulnar sublime tubercle as landmarks. Using the ultrasonography device’s calipers, the JS was measured as the distance between the distal-medial corner of the trochlea of the humerus and the proximal edge of the sublime tubercle of the ulna (Figure 1).

Measurement of the medial elbow joint space using ultrasonography. (A) Measurement site at the ulnohumeral joint. (B) Long-axis image of the ulnohumeral joint. 1 = medial epicondyle; 2 = distal-medial corner of the trochlea of the humerus; 3 = proximal edge of the sublime tubercle of the ulna; 4 = anterior bundle of the ulnar collateral ligament. The dashed white line indicates the joint space opening.
The JS measurements were performed under 11 conditions: (1-3) at 30° of elbow flexion and loads of 30 N, 60 N, and gravity stress on the forearm; (4-7) at 60° of elbow flexion and loads of 30 N, 60 N, 90 N, and gravity stress on the forearm; and (8-11) at 90° of elbow flexion and loads of 30 N, 60 N, 90 N, and gravity stress on the forearm. The Telos measurement protocol was first used to take an ultrasound image of the medial elbow joint at the start limb position. Load was then gradually increased at 10 N/s, and an ultrasonographic image was again obtained while maintaining the default load.
In the JS measurement protocol for gravity stress on the forearm, ultrasonographic images of the medial elbow joint were first taken in the absence of gravity stress. The height of the bed on which the participant lay supine was then raised until the forearm was separated from the table, and ultrasound images were again obtained with gravity stress on the forearm. Three ultrasonographic images were taken within 10 seconds, and JS was calculated as the average value of the 3 images. A 5-minute rest period and a 2-minute measurement preparation period were provided between each measurement (Figure 2). The order of measurement was randomized, and measurements were obtained on 2 different days with an interval of 1 to 7 days.

Protocol for measurement of the medial elbow joint space. US, ultrasonography.
To verify the intrarater reliability of the JS measurements, we investigated the elbow joint of the nondominant hand side in 8 of the participants (mean age, 21 years; height, 170.5 ± 6.5 cm; weight, 63.8 ± 6.8 kg) during a 60-N load at 30°, 60°, and 90° of elbow flexion, and during gravity stress on the forearm at 90° of elbow flexion. All measurements were performed using the same method and by the same examiner as above. The measurement order was random, and measurements were performed with at least a 1-week interval between the tests.
Measurement of Defensive Muscle Contractions
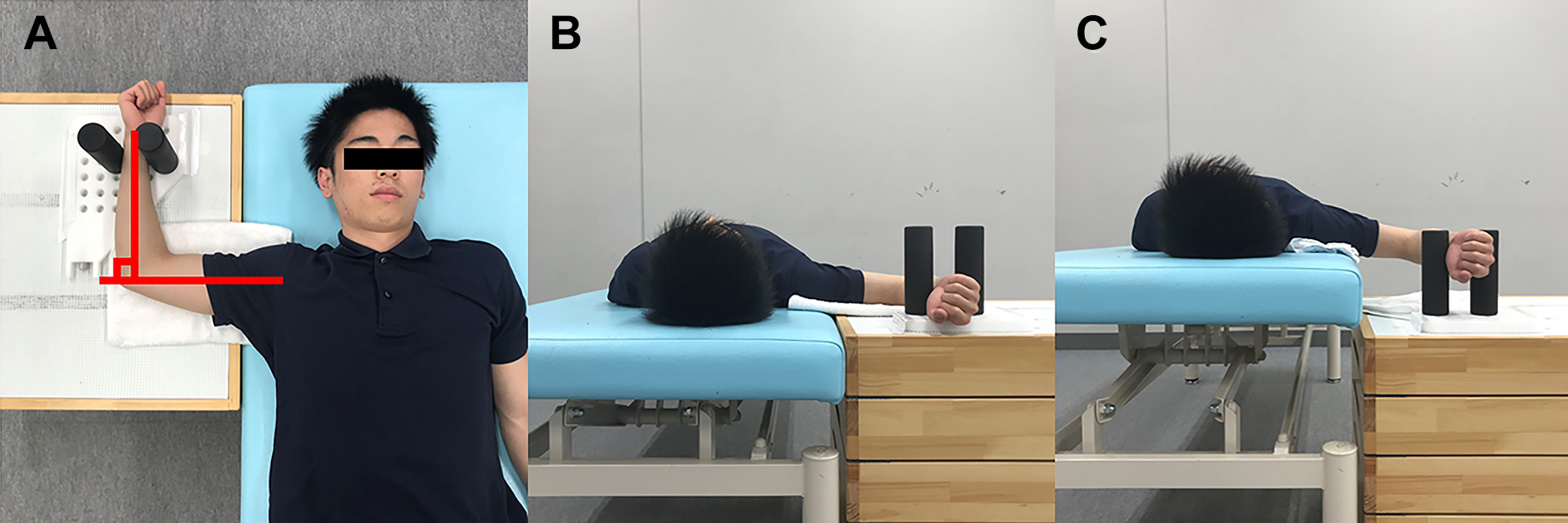
For measured limb positions, the angle of elbow flexion was 30°, 60°, or 90°. Using a Telos stress device (Aimedic MMT), the elbow was loaded to measure valgus stress at 30, 60, 90, 120, and 150 N; in addition, gravity stress on the forearm was measured in the same 3 elbow flexion angles. For Telos measurements at 30° or 60° of elbow flexion, the participant was seated and the limb positioned at 90° of shoulder abduction, 90° of external rotation, and 90° of forearm supination, with the forearm fixed within the Telos using a goniometer (Nishikawashinwa) (Figure 3, A and B). For Telos measurements at 90° of elbow flexion, the participant was seated and the limb was positioned at 60° of shoulder abduction, 90° of external rotation, and 90° of forearm supination, with the forearm fixed within the Telos device (Figure 3C). For measurements without and with gravity stress on the forearm, the participant was positioned supine, with the limb at 90° of shoulder abduction, 90° of external rotation, and 90° of forearm supination (Figure 4).

Limb position for muscle contraction measurements using the Telos stress device. For measurements at (A) 30° and (B) 60° of elbow flexion, the limb was at 90° of shoulder abduction and external rotation and 90° of forearm supination. For measurements at (C) 90° of elbow flexion, the limb was positioned at 60° of shoulder abduction, 90° of external rotation, and 90° of forearm supination.
Limb position for muscle contraction measurements with gravity stress on the forearm. (A) The patient was positioned supine, with the limb at 90° of shoulder abduction, 90° of external rotation, and 90° of forearm supination. (B) Without gravity stress on the forearm. (C) With gravity stress on the forearm.
Muscle contractions were measured using electromyography (EMG) (DPA2078; DiaMedical Systems). After setting the distance between the electrodes to 1.0 cm and thoroughly wiping the skin with alcohol, surface electrodes (Blue Sensor; METS) were attached to the pronator teres muscle at a 1000-Hz sampling frequency. The pronator teres muscle was selected because of its location in the superficial layer of the forearm flexor muscle group as a clearly identifiable muscle under the skin. Data were converted using an analog-to-digital converter (Power Lab; AD Instruments) and input into a computer, where path filter processing (20-500 Hz) for full-wave rectification was performed using EMG analysis software (Chart 7 for Windows).
For the Telos measurements, the muscle contractions were first measured for 10 seconds in the starting limb position (0 N). Load was then gradually increased at a rate of 10 N/s, and contractions were measured at 30, 60, 90, 120, and 150 N for 10 seconds each (Figure 5A). For the gravity stress measurements, the muscle contractions were measured for 10 seconds during rest with no gravity stress applied to the forearm. The bed on which the participant lay supine was raised until the forearm was separated from the table, and muscle contractions were measured for 10 seconds with gravity stress on the forearm (Figure 5B). The order of the 2 types of measurement was randomized. After the Telos and gravity stress measurements, participants were allowed rest periods of 10 and 5 minutes, respectively.

Measurement protocol for muscle contractions on electromyogram. (A) Elbow valgus stress using Telos measurements. (B) Elbow valgus stress using gravity stress on the forearm.
The calculated muscle contraction values were normalized to premeasured values taken during maximum isokinetic tension at 90° of elbow flexion and were expressed as percentage maximum voluntary contraction (%MVC). During all measurements, EMG activity was required to be <2.5% MVC. 1 In addition, during measurements, the intensity of pain in the medial elbow joint at each load was scored using a numerical rating scale (NRS) in 11 steps, from 0 (no pain) to 10 (most severe pain imaginable). If the NRS score reached 10, measurement was stopped. Furthermore, it was fully explained in advance that the experiment could be stopped at the will of the participant, even if their pain was less than NRS 10.
Statistical Analysis
The intrarater reliability of the JS measurements was assessed using the intraclass correlation coefficient (ICC). ICC values were interpreted according to the criteria of Landis and Koch 13 : <0.00, poor; 0.00 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, almost perfect reliability.
We calculated the minimal detectable difference at the 95% confidence interval (MDD95) using the following equation: MDD95 = z × SEM ×Ö2, where z is 1.96 and SEM is the standard error of measurement, calculated as SEM = SDÖ(1 − ICC). Repeated-measures analysis of variance and paired t tests were used to compare the JS at each elbow angle and each valgus stress load, and the Bonferroni method was used for post hoc testing. The level of significance was set at 5%. All statistical analyses were performed using SPSS (version 24.0; SPSS Japan).
Results
Measurement of Medial Elbow JS
Table 1 summarizes the intrarater reliability of the ultrasound measurements of elbow JS. The ICCs ranged from 0.815 to 0.955, indicating almost perfect reliability.
Reliability of Joint Space Measurements on Ultrasound (N = 8 Elbows) a

a Data are presented as mean ± SD unless otherwise indicated. ICC, intraclass correlation coefficient; MDD95, minimal detectable difference at the 95% confidence interval.
Comparison of JS at the Start Limb Position
Table 2 shows the JS at the start limb position of the Telos measurements at each angle of elbow flexion. No significant difference in JS at the start limb position was identified between loads.
Medial Elbow Joint Space at the Start Limb Position for Each Elbow Flexion Angle (N = 20 Elbows) a

a Data are presented as mean ± SD. NA, not applicable.
Comparison of JS Between Loads at Each Angle of Elbow Flexion
Table 3 shows the JS at each elbow flexion angle and each load. At 30° of elbow flexion, the JS was significantly higher at 30 N versus 0 N and at 60 N versus 0 or 30 N (P ≤ .018 for all). At 60° of flexion, the JS was significantly higher at 30 N versus 0 N, at 60 N versus 0 or 30 N, and at 90 N versus 0, 30, or 60 N (P ≤ .024 for all). At 90° of elbow flexion, the JS was significantly higher at 30 N versus 0 N and at 60 N versus 0 or 30 N (P ≤ .028 for all).
Medial Elbow Joint Space Stratified by Elbow Flexion Angle and Load (N = 20 Elbows) a

a Data are presented as mean ± SD. NA, not applicable.
Statistically significant difference at 30° of elbow flexion:
bP < .001 versus 0 N.
cP = .018 versus 30 N.
Statistically significant difference at 60° of elbow flexion:
dP = .004 versus 0 N.
eP < .001 versus 0 N.
fP = .024 versus 30 N.
gP < .001 versus 30 N.
hP = .001 versus 60 N.
Statistically significant difference at 90° of elbow flexion:
iP = .028 versus 0 N.
jP < .001 versus 0 N.
kP = .004 versus 30 N.
lP = .001 versus 30 N.
mP < .001 versus 60 N.
nP < .001 versus 90 N.
oP = .002 versus gravity stress at 30° of elbow flexion.
pP = .006 versus gravity stress at 60° of elbow flexion.
Comparison of JS Between Elbow Flexion Angles at Each Load
At 0 N, the JS was significantly lower at 90° versus 60° of elbow flexion (P = .005). At 30 N, the JS was significantly lower at 90° versus 30° of elbow flexion (P = .023) and 90° versus 60° of elbow flexion (P = .006). At 60 N, the JS was significantly lower at 90° versus 30° of elbow flexion (P = .019) and at 90° versus 60° of elbow flexion (P = .015). At 90 N, the JS was significantly lower at 90° versus 60° of elbow flexion (P < .001).
Comparison of JS With Gravity Stress at 90° of Elbow Flexion and With Each Load at 30°, 60°, and 90° of Elbow Flexion
The JS was significantly lower with gravity stress at 90° of elbow flexion versus 30° (P = .002) and 60° (P = .006). At 90° of elbow flexion, the JS was significantly lower with gravity stress versus loads of 60 N (P < .001) and 90 N (P < .001).
Confirmation of Defensive Muscle Contractions
Table 4 shows the number of participants showing defensive muscle contractions (muscle contractions, ≥2.5% MVC) under each condition. Defensive contraction was not observed in any participants for 11 elbow conditions with 30 N, 60 N, and gravity stress on the forearm with 30° of elbow flexion; 30 N, 60 N, 90 N, and gravity stress on the forearm with 60° of elbow flexion; and 30 N, 60 N, 90 N, and gravity stress on the forearm with 90° of elbow flexion. In addition, 2 patients with 150 N with 30° of elbow flexion, 2 patients with 150 N with 60° of elbow flexion, and 1 patient with 150 N with 90° of elbow flexion complained of severe pain (NRS 10), so measurements were discontinued.
Participants With Defensive Muscle Contractions Stratified by Elbow Flexion Angle and Load (N = 20 Participants) a

a Data are presented as number of participants with defensive muscle contractions. Defensive muscle contractions were defined as those with ≥2.5% maximum voluntary contraction.
Discussion
This study was to measure joint space (JS) opening during the application of elbow valgus stress with different elbow flexion angles and loads and to clarify the presence of muscle contractions as a defensive mechanism during elbow valgus stress. To the best of our knowledge, no studies have appropriated elbow valgus stress using the Telos stress device, which can be applied to reflect UCL function without risking defensive muscle contraction.
Our results indicated that there was no significant difference in JS at the start limb position during Telos measurements at any elbow flexion angle. When comparing JS between different angles of elbow flexion, JS was significantly lower at 90° than at 30° or 60° of elbow flexion for the most loads. Among patients with an injured UCL, an anterior bundle injury is common. 14 A cadaveric study reported that 90° of elbow flexion showed greater elbow valgus angle after the anterior bundle amputation than 30° and 60° of elbow flexion. 3,15 In this study, alignment such as articular shape and carrying angle is not considered, but evaluation at 90° of elbow flexion may more readily reflect the functionality of both the anterior bundle and the overall UCL.
The JS was significantly lower with gravity stress at 90° of elbow flexion than with gravity stress at 30° of elbow flexion (P = .002) and gravity stress at 60° of elbow flexion (P = .006). In addition, at 90° of elbow flexion, the JS was significantly lower with gravity stress compared with 60-N and 90-N loads (P < .001 for both). Gravity stress at 90° of elbow flexion may thus represent a load that produces a smaller JS than 60 N at 90° of elbow flexion.
In this study, some patients showed defensive muscle contractions with loads ≥90 N at 30° of elbow flexion and with loads ≥120 N at 60° and 90° of elbow flexion. Some patients with UCL injury have reportedly shown a lower JS in the injured elbow than in the uninjured elbow when elbow valgus stress of 150 N is applied, but a protective factor due to pain that may have affected JS has also been reported. 2 Also, elbow valgus stability by the flexor-pronator muscles contractions has been reported. 11,18,22,24 The results of the present study suggest that defensive muscle contraction did not occur at any elbow flexion angles with elbow valgus stress ≤60 N using the Telos device, and JS increased as load increased. Ligaments have the property that strain increases with increasing stress. 7 Elbow valgus stress ≤60 N using the Telos device may thus be applicable to reflecting UCL function without risking defensive muscle contraction.
Several limitations must be considered in this study. First, the electromyograms could not be accurately measured because of the noise generated by ultrasonic waves during JS measurement, and the presence or absence of defensive contraction could not be confirmed. This study, therefore, investigated loads that did not cause defensive contraction under conditions of elbow valgus stress in the same participant in advanced research. Based on those preliminary results, defensive contraction was not considered to occur during standard protocols for JS measurement. Second, because of the characteristics of the Telos device, there was a possibility that valgus stress was slightly applied to the elbow joint even at the start limb position (0 N), so there was a significant difference in JS between the start limb position and when there was no gravity stress on the forearm. Third, this study targeted the elbow joint on the nondominant hand side among healthy male university students. In the future, investigations on the dominant side of both symptomatic and asymptomatic throwing athletes will be needed. Last, in this study, elbow valgus stability by the flexor-pronator muscles 11,18,22,24 was not considered.
Conclusion
This study suggests that elbow valgus stress ≤60 N using a Telos device could allow the evaluation of UCL function without muscle contraction. Alignment such as articular shape and carrying angle is not considered, but evaluation at 90° of elbow flexion may more readily reflect the functionality of both the anterior bundle and the overall UCL. Also, gravity stress on the forearm in 90° of elbow flexion may represent a load that produces a smaller JS than 60 N in 90° of elbow flexion. This study is considered to be useful basic research for standardizing the method for evaluating elbow valgus instability.
Footnotes
Final revision submitted April 29, 2021; accepted June 8, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a Grant-in-Aid for Scientific Research (19K11358) from the Japanese Society for the Promotion of Science (JSPS) and was commissioned by the Japan Sports Agency (Female Athletes Development and Support Projects 2020). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Niigata University of Health and Welfare (study No. 18430).