
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic significantly affected the lives of Japanese collegiate men’s basketball players.
Purpose:
To describe the incidence of lower extremity injuries in Japanese collegiate men’s basketball during the COVID-19 pandemic and examine the effects of the pandemic on injury patterns.
Study Design:
Descriptive epidemiological study.
Methods:
Using data from a surveillance project of the Department of Medicine and Science of the Kanto Collegiate Basketball Federation, the authors included data from 6 men’s basketball teams during the 2020-21 and 2021-22 seasons (11 team seasons). Injury rates per 1000 athlete-exposures (AEs) were calculated according to injury type, location, and frequency. Injury burden was estimated by multiplying the injury rate by the mean days lost. Injuries from the 2020-21 to 2021-22 seasons were compared with those before the pandemic (2013-14 to 2019-20 seasons) using injury rate ratios (IRRs), with significant differences indicated when the 95% CI did not include 1.0.
Results:
In total, 135 lower extremity injuries were reported during 27,249 AEs. The overall injury rate of the 2020-21 to 2021-22 seasons was significantly higher than that of the 2013-14 to 2019-20 seasons (IRR, 1.37; 95% CI, 1.12-1.67). Lateral ankle sprains (IRR, 1.37; 95% CI, 1.02-1.86), hamstring strains (IRR, 2.86; 95% CI, 1.34-6.12), jumper’s knee (IRR, 2.68; 95% CI, 1.13-6.37), and stress fractures of the proximal fifth metatarsal (IRR, 7.16; 95% CI, 1.31-39.08) were significantly higher during the 2020-21 to 2021-22 seasons compared with the 2013-14 to 2019-20 seasons.
Conclusion:
The rate of lower extremity injuries increased significantly in Japanese collegiate men’s basketball players during the COVID-19 pandemic. The results of this study emphasize the importance of optimal screening and specific loads for injury prevention when detraining periods are anticipated.
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2, restricted people’s lives for >2 years. In Japan, the government declared a state of emergency with various restrictions on behavior and activities 4 times (from April to May 2020, January to March 2021, April to June 2021, and July to September 2021). The impact on sports events was significant. The Tokyo Olympics and Paralympics scheduled for the summer of 2020 were postponed until the summer of 2021, and for the first time in history, the games were held without spectators. Japanese collegiate athletes were forced to suspend their activities, practices, and competitions. In particular, under the state of emergency declaration, many collegiate athletes experienced home confinement, had no access to athletic facilities, and were forced to take remote classes. Currently, with the wide distribution of vaccines, expansion of the testing system, mutation of major epidemic strains with less severe ones, and basic infection control measures that have become routine practice, both daily life and infection control have progressed. Collegiate sports have resumed gradually because these changes in the environment.
Previous research on Japanese collegiate men’s basketball players for 7 seasons (2013-14 to 2019-20) indicated that injury rates are higher in Japan than in men’s basketball players from the National Collegiate Athletic Association (NCAA) in the United States. 17,20,26 In a previous study, 20 we found that the rate of ankle sprains was 2.1 times higher in Japan. These results highlight the importance of making medical support (ie, injury prevention strategies and appropriate recovery process by medical personnel) available for Japanese collegiate athletes. 20
The Department of Medicine and Science of the Kanto Collegiate Basketball Federation (KCBF) was established in 2004 to prevent injury and illness and to improve the athletic performance of Japanese collegiate basketball players. This department conducts an injury surveillance project aimed at further improving medical support systems to protect basketball players. Information from this database has been utilized to monitor players’ conditions, including frequency of activity and injury trends.
Athletes were likely exposed to some level of detraining (loss of training-induced morphological and physiological adaptation) because of insufficient and/or inappropriate training stimuli during the COVID-19 pandemic. 19 Several studies have reported the effects of the COVID-19 pandemic on lower extremity injuries. 4,15,16,19 Demir et al 4 showed the risk for muscle injuries due to long-term detraining by COVID-19 confinement in professional soccer players. A retrospective review of new patients in the city of Chicago reported a significantly higher proportion of ankle fractures and stress fractures than those during the same months before the COVID-19 pandemic. 15
As there are no epidemiological studies available on Japanese collegiate men’s basketball players during the COVID-19 pandemic, the purpose of the current study was to describe the incidence of lower extremity injuries in this population during 2 seasons affected by the pandemic (2020-21 and 2021-22). Lower extremity injuries were chosen, as they have been reported as the most frequent in basketball. 5,20,26 In addition, we compared injury patterns during the pandemic with prepandemic injury data. We hypothesized that the incidence of lower extremity injuries would increase during the study period owing to the limitations or restrictions related to the pandemic.
Methods
Data managed by the Department of Medicine and Science of the KCBF were used in this study. The investigation concerned data during the academic year (April 1–March 31) in Japan from 2020-21 and 2021-22. Six teams from the KCBF Division I League participated in the investigation. This study was conducted in accordance with the tenets of the Declaration of Helsinki, and the protocol received ethics committee approval.
Most definitions in the present study were based on our previous study on Japanese collegiate men’s basketball players from the 2013-14 to 2019-20 seasons. 20 An injury was defined as any event that (1) occurred because of participation in regular practice or competition in sports, (2) caused the player to seek medical care from physicians or alternative medical personnel, or (3) resulted in the restriction of student-athlete participation or performance for 1 or more calendar days since the day of injury. Injury rates were calculated per 1000 athlete-exposures (AEs), in which an AE was defined as participation in a practice or official competition organized by the KCBF and the All-Japan University Basketball Federation wherein the player was exposed to the possibility of athletic injury, regardless of the time of participation. Participation in prematch warm-up was not considered. A lower extremity injury was classified as occurring in the hip/groin, thigh, knee, lower leg/Achilles tendon, ankle, or foot. Injury type was classified according to the International Olympic Committee consensus statement. 1 Injury burden (days’ absence per 1000 AEs) was estimated by multiplying the injury rate by the mean days lost before return to practice and competition. 6
Prepandemic data from our previous study (2013-14 to 2019-20) 20 were recalculated and analyzed with data from the present study (2020-21 to 2021-22). We calculated injury rate ratios (IRRs) between the data before and during the COVID-19 pandemic, with significant differences indicated when the 95% CI did not include 1.0. To evaluate the effect of the pandemic on the opportunity to play basketball, AEs per team season were compared using the independent t test after recognizing normal distribution (Shapiro-Wilk test). All statistical analyses were performed using SPSS Version 28.0 software (IBM).
Results
During the 2020-21 to 2021-22 seasons, 27,249 AEs were recorded: 25,062 in practice and 2187 in competition. The numbers of practice, competition, and overall AEs per team season during the 2 pandemic years were significantly lower than those in the 2013-14 to 2019-20 seasons (P < .001; d = 1.61-1.82) (Figure 1). A total of 135 lower extremity injuries were reported across 11 team seasons, of which 121 (89.6%) occurred during practice and 14 (10.4%) during competition (Table 1). The injury rate in the 2020-21 to 2021-22 seasons was higher than that in the 2013-14 to 2019-20 seasons (overall IRR, 1.37 [95% CI, 1.12-1.67]; practice IRR, 1.64 [95% CI, 1.33-2.04]). There was no significant difference in the injury rate during competitions. The injury burdens for the 2-year surveillance period were as follows: overall injuries, 115.9 days’ absence per 1000 AEs; practice, 107.2 days’ absence per 1000 AEs; and competition, 219.1 days’ absence per 1000 AEs. The injury burden overall and during practice was higher in the 2020-21 to 2021-22 seasons (115.9 and 107.2 days’ absence per 1000 AEs, respectively) than in the 2013-14 to 2019-20 seasons (66.3 and 47.3 days’ absence per 1000 AEs, respectively).

Difference in athlete-exposures per team season between the 2013-14 to 2019-20 and 2020-21 to 2021-22 seasons.
Comparison of Injury Counts, Rates, and Burden by Body Part and Injury Type Between the 2020-21 to 2021-22 and the 2013-14 to 2019-20 Seasons a

a Bolded text indicates values that were significantly higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons. IQR, interquartile range; IR, injury rate (per 1000 athlete-exposures); IRR, injury rate ratio.
b Reported as days’ absence per 1000 athlete-exposures.
c The number of overall injuries does not equal the sum of practice and competition injuries, as event information was missing for 2 injuries.
d IQR was not indicated, as days lost was not recorded for 1 of the 2 cases.
Ankle (48.1%) and knee (20%) injuries were the most reported during the pandemic, and their injury rates were significantly higher than those in the 2013-14 to 2019-20 seasons (IRR for ankle injury, 1.35 [95% CI, 1.02-1.80]; IRR for knee injury, 1.97 [95% CI, 1.23-3.15]). Knee injuries were the most severe according to injury burden (50.8 days’ absence per 1000 AEs; median, 30.5 days [interquartile range [IQR], 5.8-58 days]). The rates of muscle strain/rupture in the thigh (IRR, 2.58 [95% CI, 1.27-5.27]), joint sprain/ligament tears in the ankle (IRR, 1.36 [95% CI, 1.02-1.82]), tendinopathy in the knee (IRR, 2.24 [95% CI, 1.01-4.93]), and bone stress injury in the foot (IRR, 4.77 [95% CI, 1.07-21.32]) were significantly higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons.
Lateral ankle sprains (LAS) were the most common injuries in this study (n = 58; 43%). The incidence of the following injuries also increased: hamstring strains (n = 12; 8.9%), jumper’s knee (patellar and quadriceps tendinopathy 21 ; n = 9; 6.7%), medial collateral ligament (MCL) injuries (n = 5; 3.7%), and proximal fifth metatarsal (MT5) stress fractures (n = 4; 3%) (Table 2). The rates of LAS (IRR, 1.37 [95% CI, 1.02-1.86]) and hamstring strains (IRR, 2.86 [95% CI, 1.34-6.12]) in the 2020-21 to 2021-22 seasons were higher than those in the 2013-14 to 2019-20 seasons. The rates of jumper’s knee (IRR, 2.68 [95% CI, 1.13-6.37]) and MT5 stress fractures (IRR, 7.16 [95% CI, 1.31-39.08]), which are chronic injuries, were also higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons. Although not statistically significant, the rate of MCL injuries tended to be higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons. The injury burden for all injuries having increased incidence in the 2020-21 to 2021-22 seasons was higher than that in the 2013-14 to 2019-20 seasons.
Common Injuries Between the 2020-21 to 2021-22 Seasons and 2013-14 to 2019-20 Seasons a
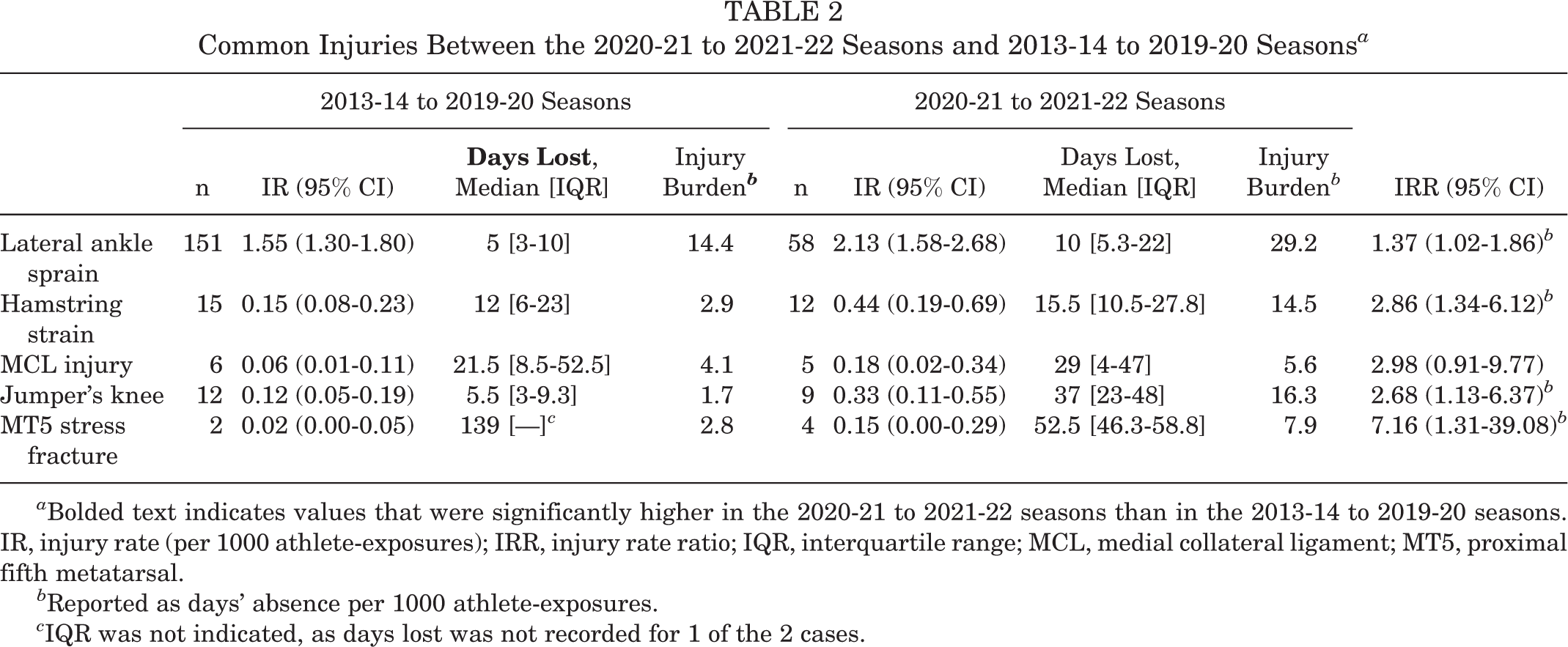
a Bolded text indicates values that were significantly higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons. IR, injury rate (per 1000 athlete-exposures); IRR, injury rate ratio; IQR, interquartile range; MCL, medial collateral ligament; MT5, proximal fifth metatarsal.
b Reported as days’ absence per 1000 athlete-exposures.
c IQR was not indicated, as days lost was not recorded for 1 of the 2 cases.
Discussion
This study is the first to describe the incidence of lower extremity injuries in Japanese collegiate men’s basketball players during 2 seasons affected by the COVID-19 pandemic (2020-21 and 2021-22) and the typical injury patterns observed during the pandemic compared with before the pandemic (2013-14 to 2019-20). The overall lower extremity injury rate was 1.37 times higher in the 2020-21 to 2021-22 seasons compared with the 2013-14 to 2019-20 seasons.
Injury is regulated by a complex mechanical interplay between tissue stress, strain, and loading. Since muscle strength, architecture, and tendon structures are factors that influence injury risk, athletes may be more susceptible to injury through an alteration of the tissue-specific mechanical properties related to the limitation of activity caused by the COVID-19 pandemic. 11,19 A previous study that evaluated the mechanical stress and intensities measured by a triaxial accelerometer in Japanese men’s collegiate basketball games reported that basketball players spend considerable energy on deceleration, landing, and physical contact. 12 Our results showed a significant decrease in AEs compared with those before the COVID-19 pandemic (see Figure 1), indicating that the mechanical load on a player’s lower extremity derived from playing basketball decreased.
In Japan, collegiate activities were implemented carefully (eg, remote learning) during the pandemic, and the resumption of college sports was a low priority. During and after confinement due to the COVID-19 pandemic, players did not have access to athletic facilities or training resources and had limited activity time. Thus, the conditions related to the injury (physiological and mechanical characteristics of the human body 11 ) could have been difficult to manage. A significant decrease in basketball opportunity, which caused a lack of playing-induced specific and optimal load, might have contributed to the increased injury rates in the 2020-21 to 2021-22 seasons seen in the current study.
Hamstring strain is one of the most common injuries in Japanese collegiate men’s basketball players. 20 In this investigation, the incidence of hamstring strains increased significantly during the COVID-19 pandemic (IRR, 2.86 [95% CI, 1.34-6.12]). Generally, low strength and morphological features of the hamstrings have been reported as risk factors of hamstring strains. 18,22 The effects of the confinement duration on changes in eccentric hamstring muscle strength were expected at the beginning of the COVID-19 pandemic, 16 and long-term detraining because of COVID-19 confinement implied an association with muscle injuries. 4 After the significant decrease in opportunities to play basketball, it was inferred that the decline in mechanical stress and load was derived from inadequate basketball practice, conditioning, or training. These effects of the COVID-19 pandemic may influence the risk factors of hamstring strains.
Interestingly, although prior hamstring strain is an established risk factor for additional strains, 24 75% (n = 9) of hamstring strains that occurred in the 2020-21 to 2021-22 seasons occurred in players with no history of strain. Demir et al 4 studied the effects of the COVID-19 confinement on hip strength, flexibility, and muscle injury rate in professional soccer players and found that hamstring eccentric strength could not reach preconfinement strength values; in addition, 16.7% (5 of 30) of players with no history of muscle injuries were found to have hamstring and adductor injuries when they returned to play. We speculate that the increase in hamstring strain rates was likely related to the enforced detraining because of COVID-19 confinement. Furthermore, it is possible that COVID-19 confinement increased the risk for hamstring strain in players with no history.
The injury rates of ankle sprains in Japanese men’s collegiate basketball players, which have been reported to be significantly higher than those in NCAA men’s basketball players, 17,20,26 were further exacerbated by the COVID-19 pandemic. In the current study, LAS, which accounted for >90% of ankle sprains, occurred significantly more frequently than before the pandemic (IRR, 1.37 [95% CI, 1.02-1.86). Since 43% of overall injuries were LAS, an increased injury rate of LAS influenced the overall injury rates directly.
Several studies have reported that detraining influences a decline in ankle performance (kinematic, proprioceptive, and stabilometric performances). 3,25 McGuine et al 14 reported that a higher postural sway score during a single-leg stance measured during preseason corresponded to increased ankle sprain rates in basketball players. Dai et al 3 showed increased center of pressure sway area, standard deviation, and velocity measured by 2 eye-closed, single-leg stance tests after a mean of 30.2 ± 1.2 days of detraining (postseason break) in highly trained female volleyball players. In the most severe period during the 2 years of the COVID-19 pandemic, any team that recognized players who had been infected (confirmed via testing at a medical institution, and if the infection was diagnosed, it was reported to the local government office in their place of residence) was forced to stop any activity and follow quarantine (maximum 14 days) procedures, even though access to all athletic facilities and activities was permitted. In the most severe period (2020-2021), there was a 14-day quarantine period starting from the date of contact with someone who confirmed positive. In Japan, contact was defined as any interaction lasting more than 15 minutes within a close proximity of approximately 1 meter, without taking necessary precautions against infection. In the context of basketball practices and games, it was challenging to pinpoint the exact timing of contact. Therefore, in the event of a confirmed positive case, team activities were uniformly suspended, and new cases were monitored for at least 48 hours to detect any potential additional infections. These restrictions caused a decrease in opportunities to play basketball (shown by the decrease in AEs). Basketball playing is required to maintain ankle proprioceptive function and might influence the increase in rates of LAS in Japanese collegiate men’s basketball players.
Increased bone stress injuries in the foot, all of which were MT5 stress fractures, might be influenced by nutritional condition, restriction of activity, or their interactive effects. Mehta et al 15 found that during the COVID-19 pandemic, a significantly higher proportion of stress fractures than that in the same months of the previous year was reported. Those authors suggested the possibility of high-repetition exercises on unfamiliar surfaces, which would increase the risk for stress fractures. Additionally, COVID-19 confinement may affect bone metabolism. Adequate mechanical load and nutrients are required to maintain bone metabolism. In particular, vitamin D, which is necessary for sufficient bone health through upregulation of the expression of genes that enhance calcium absorption and bone deposition, is unique in that it is synthesized in the skin in the presence of ultraviolet B light from sunlight. 8,9 Potentially, indoor sports athletes had lower circulating vitamin D levels than outdoor sports athletes because of lower sun exposure. Thus, indoor sports athletes have been considered at an increased risk of vitamin D insufficiency and deficiency. 7 The interactions among the lower basketball-specific loads because of decreased AEs, mechanical load on the lower extremity by exercise on unfamiliar surfaces as an alternative to basketball-specific load and conditioning, change in nutritional conditions, and the intensity or volume of basketball after resumption might have influenced the findings of the present study.
Quadriceps strength is a proven risk factor for jumper’s knee, which includes patellar and quadriceps tendinopathy. 21,23 In particular, the onset of symptoms is related to high-level eccentric quadriceps loading, such as that occurring with knee flexion when landing from basketball rebounds. 21 Hortobágyi et al 10 investigated the effect of 14 days of detraining on power athletes and reported a decrease in isokinetic eccentric knee extension force, with a significant decrease in the type 2 muscle fiber cross-sectional area (CSA) of the vastus lateralis, levels of plasma hormones (growth hormone, testosterone, and cortisol), and serum creatine kinase enzyme levels. Another study, which investigated the adaptation of the mechanical and morphological properties of muscles and tendons for 3 months of isometric knee extension training and 3 months of detraining, showed that the increased knee extensor CSA and patellar tendon stiffness obtained by resistance training were significantly decreased toward the pretraining level during the detraining period. 13 From these detraining findings, the significant decrease in activity level during the COVID-19 pandemic might cause loss of the proper mechanical load generated and obtained by basketball movements, such as jumping, acceleration, and deceleration, and cause a decrease in eccentric knee extension strength with morphological changes.
The period for which an athlete is unable to train or play (time loss) is used to assess injury severity. 1 In the current study, the injury burden of most injuries tended to be higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons. Although these results were considered to be because of the significant increase in injury rates, similar trends were observed in the median days lost. Since the partial limitation of activity time retained after the resumption of college sports activity, we speculate that the opportunity for appropriate treatment, rehabilitation, or reconditioning for injured athletes had been reduced. Moreover, there was no rush to return to play after injury and treatment because there were fewer competitions in the 2020-21 and 2021-22 seasons. For these reasons, the timing of return to play was influenced not only by the individual injury or athlete, but also by the specific environment created by the COVID-19 pandemic. The unique disruptions to return to play during the COVID-19 pandemic make it difficult to assess injury severity according to time loss. 2
Limitations
Our study has some limitations. First, this was an observational epidemiological study that did not include morphological and physiological characteristics related to injury occurrence; thus, the injuries from the 2020-21 to 2021-22 seasons could not be fully evaluated. Second, there was potential for reporting bias because of the data being collected by different individuals over a long period. Finally, the inherent potential for cultural differences should be recognized, as the injury patterns investigated in this study were dependent on the countermeasures implemented in Japan against the COVID-19 pandemic.
Conclusion
Study findings indicated that the rate of lower extremity injuries was 1.37 times higher in the 2020-21 to 2021-22 seasons than in the 2013-14 to 2019-20 seasons in Japanese collegiate men’s basketball players. Our results emphasize the importance of optimal screening and specific loads for injury prevention when detraining periods are anticipated.
Footnotes
Acknowledgment
The authors offer their sincerest thanks to all the members of the Department of Medicine and Science of the Kanto Collegiate Basketball Federation and the team staff for their time, effort, and cooperation during this project.
Final revision submitted January 15, 2023; accepted February 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from the Japan Society for the Promotion of Science (KAKENHI; grant No. JP20K19514) and the Japan Sports Medicine Foundation (2021). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Teikyo Heisei University (No. R01-080-1).