
Abstract
Background:
Whether the extent of glenoid bone loss (GBL) affects clinical outcome after coracoid process transfer (CPT) is still unclear.
Purpose:
To evaluate postoperative outcomes after CPT combined with open Bankart repair in young rugby players in terms of the extent of GBL and between the Bristow and Latarjet techniques.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The authors investigated 101 shoulders in 91 competitive rugby players who underwent CPT combined with open Bankart repair by the Bristow (group B; 66 shoulders) or Latarjet (group L; 35 shoulders) procedure between 2007 and 2017. The extent of GBL was calculated from the en face view of the glenoid on preoperative 3-dimensional computed tomography scans and was used to categorize shoulders into 4 grades (grade 0, 0%; grade 1, >0% and ≤10%; grade 2, >10% and ≤20%; grade 3, >20%). At the minimum 2-year follow-up, the authors analyzed the relationship between GBL or GBL grade and postoperative outcome scores (American Shoulder and Elbow Surgeons score, Rowe score, Western Ontario Shoulder Instability Index, and patient satisfaction), return-to-play (RTP) times, graft failure (insufficient union or translocation), and recurrence.
Results:
The mean GBL in all shoulders was 10.9% ± 9.2% and was not significantly different between the 2 groups. There were no significant correlations between GBL and any outcome measure in either group. The mean RTP time was significantly shorter in group L versus group B (4.8 ± 1.1 vs 5.8 ± 1.8 months, respectively; P = .002), but it was not associated with GBL. In group B, the rate of graft failure was not significantly higher in shoulders with grade 0 or 1 GBL versus grade 2 or 3 GBL (8 [25.0%] vs 4 [11.8%], respectively; P = .21). In group B, graft failure was confirmed in 12 shoulders (18.2%), compared with 1 shoulder (2.9%) in group L. Postoperative recurrence occurred in significantly fewer shoulders in group B than in group L (2 [3.0%] vs 5 [14.3%], respectively; P = .047).
Conclusion:
The extent of GBL did not affect outcome scores after CPT, regardless of operative procedure.
Arthroscopic Bankart repair (ABR) is the gold standard in the surgical treatment of traumatic anterior shoulder instability. However, bone loss, 5,8,24,40 younger age, 24,36,40 and playing a collision or contact sport 12,24,36 are recognized as risk factors for recurrence after ABR. Glenoid bone loss (GBL) is considered to be the most critical element in recurrence after ABR, and significant reduction of anterior stability is known to occur when GBL is 20% or more. 14,38 In addition, a GBL of 13.5% has been suggested to be a threshold value for the occurrence of shoulder dysfunction after ABR alone and is considered by some to represent subcritical bone loss. 30
GBL is the one of the factors that can be addressed by orthopaedic surgeons through the choice of surgical technique, and reconstruction of the bone defect by coracoid process transfer (CPT), autologous bone grafting (iliac bone, 1,35 distal clavicle, 3,34 or scapular spine 22 ), or artificial bone grafting 13 is recommended in shoulders with a large degree of GBL. However, because younger age and playing a contact or collision sport are considered to be strong risk factors for recurrence after ABR alone, performing only capsulolabral complex repair is often not sufficient in these patients regardless of the extent of GBL. 17,19
In competitive rugby players, the recurrence rates after ABR are known to be much higher than in players of other collision sports because of the particular characteristics of rugby 24 ; thus, at our hospital we perform CPT combined with Bankart repair for traumatic anterior shoulder instability in young rugby athletes regardless of preoperative GBL. Tanaka et al 32 previously demonstrated high return-to-play (RTP) rates and good clinical results after this combined procedure. They also found earlier and higher bone union in the Latarjet procedure but higher bone resorption and more frequent subluxations and need for injection for pain after the Latarjet procedure compared with the Bristow procedure.
Because CPT is generally performed in patients with a large degree of GBL, few studies have evaluated the association between postoperative healing of the transferred coracoid and smaller degrees of GBL (≤10%) or no GBL. In addition, it is unclear whether this association is different between CPT with the Bristow versus Latarjet procedures. As the size of the bone contact surface on the graft side is smaller in the Bristow versus the Latarjet procedure 10 and as the extent of GBL affects the bone shape of the graft recipient site around the anterior glenoid neck, the effect of GBL on graft healing may differ between the 2 techniques.
The aim of the present study was to evaluate postoperative outcomes after CPT combined with open Bankart repair in young rugby players in terms of the extent of GBL and between the Bristow and Latarjet techniques. We hypothesized that the extent of GBL would not affect clinical outcomes after CPT.
Methods
Patients
Between 2007 and 2017, 151 consecutive shoulders in 137 competitive rugby players underwent surgical treatment for traumatic anterior shoulder instability at our hospital. Shoulders were included that were treated by CPT by the Bristow or Latarjet procedure combined with a Bankart repair. Exclusion criteria were as follows: isolated Bankart repair or Bankart repair combined with a procedure other than CPT, capsular repair, revision surgery, rotator interval closure, and follow-up <2 years. At our hospital, CPT was performed only by the Bristow procedure until December 2014 and by the Latarjet procedure thereafter because the Latarjet procedure was assumed to show a higher graft union rate, which could provide better clinical results.
The study protocol received institutional review board approval from our hospital. At the initial consultation, an opt-out method was applied for patient agreement with the anonymous use of their clinical data, so documented informed consent was not required from all patients.
Surgical Procedure and Rehabilitation
All operations were performed by the same orthopaedic surgeon (M.T.) in accordance with previously reported methods. 6,32 A standard deltopectoral approach was used to expose the coracoid process and cut the coracoid using an L-shaped bone saw. Subsequently, the lower one-third of the subscapularis muscle was split to reach the anterior capsule and a horizontal capsulotomy was performed to expose the anterior glenoid neck. In the Bristow method, a guide pin was inserted from the tip of the coracoid process to the center of the osteotomy surface and overdrilled with a 3.0-mm cannulated drill. Next, the anterior capsulolabral complex was completely detached until as inferiorly as possible (until the 6-o’clock position of the glenoid). If the patient had a bony Bankart lesion, the lesion was completely removed. A guide pin was then inserted at the 4-o’clock position, 5 to 8 mm medial to the articular surface of the glenoid, and overdrilled with a 3.0-mm cannulated drill. Then, the soft anchors were inserted into the edge of glenoid, and their sutures were passed through the fully detached capsulolabral complex by using the mattress suture technique. At least 3 single-loaded suture anchors were inserted with care taken to avoid the tunnel. Then, the coracoid graft was fixed by placing a 4.0 mm–diameter cannulated screw and washer over the guide pin. Finally, the sutures were tied with sufficient tension so that the capsulolabral complex was reattached at least 1 hour above its detached position in clock positioning under 20° of flexion and neutral rotation.
In the Latarjet procedure, the proximal drill hole was created in the proximal part of the coracoid graft in the graft-lying position, and the position of the proximal drill hole on the glenoid side was set at 3:30 o’clock and drilled through a guide pin 5 to 8 mm medial to the glenoid surface. After preparation for screw fixation, the capsulolabral complex was repaired using suture anchors similar to the Bristow technique. Two cannulated screws, 4.0 mm and 3.5 mm in diameter and each with a washer, were used for the proximal and distal parts of the graft fixation, respectively. After graft fixation using the first screw (4.0 mm), another drill hole for the second screw (3.5 mm) was created in the graft and glenoid neck, and the screw was inserted. Then, sutures were tied as in the Bristow procedure.
In both procedures, the cortical bone of the anterior glenoid neck was thinly cut, and lattice slits were created with a chisel to facilitate bleeding from the bone marrow. In all cases, the aim was to achieve bicortical screw fixation, and sufficient fixation of both screws was confirmed with postoperative radiography. The operated shoulder was immobilized in the internal rotated position with a brace.
Postoperative rehabilitation consisted of passive forward elevation exercises in the supine position 2 weeks after surgery and active forward elevation and external rotation exercises at 6 weeks after surgery. Muscle strengthening exercises were permitted from 3 months. Patients returned to rugby practice about 4 months after the operation, and full RTP was allowed depending on range of motion, muscle strength, and graft healing evaluated using computed tomography (CT).
Evaluations
CT Imaging Analysis
All patients underwent CT with an Aquilion scanner (Canon Medical Systems Corporation) to analyze glenoid morphology preoperatively and to evaluate the transferred coracoid graft postoperatively. Imaging data were obtained at a slice thickness of 0.5 mm and reconstructed into 3-dimensional models of the glenoid. The preoperative GBL (in percentage) was calculated from the en face view of the glenoid by using the assumed circle method, 23 and the GBL value was used to assign each shoulder to 1 of 4 grades (grade 0, 0%; grade 1, >0% and ≤10%; grade 2, >10% and ≤20%; grade 3, >20%). Postoperative CT was performed on the day after surgery and after 3, 6, and 12 months, depending on patient consent. Coracoid graft conditions were diagnosed according to Tanaka et al 32 as union, insufficient union, or translocation (including graft fracture). In brief, the absence or presence of a radiolucent zone between the coracoid process and glenoid was used to distinguish between union and insufficient union, and translocation was defined as dislocation of the graft from the screw (including bone fragment fracture) or backing out of the screw.
Postoperative Outcomes and Recurrence
Clinical outcomes were evaluated by the American Shoulder and Elbow Surgeons (ASES) 28 and Rowe 29 scores at the preoperative examination and final follow-up and also by the Western Ontario Shoulder Instability Index (WOSI) 16 and patient satisfaction rating at the final follow-up. Time to RTP, postoperative recurrence, and complications other than recurrence were also investigated. Recurrence was defined as any report of dislocation or subluxation; the latter was defined as an episode of shoulder instability that did not require manual reduction by a health care provider. 25
Statistical Analysis
Comparisons between patients who underwent the Bristow versus Latarjet procedure were performed with the Mann-Whitney U test or chi-square test, and the pre- and postoperative data of each operative technique were compared with the paired t test. We evaluated the association between preoperative GBL and each outcome measure using correlation analysis. In addition, we evaluated graft condition on final postoperative CT according to both preoperative GBL grade and postoperative outcomes. Statistical analysis was performed with JMP software (Version 16.0.0; SAS Institute Inc). Statistical significance was assumed at P < .05.
Regarding sample size calculation, it was determined that 26 shoulders would be required for the detection of a 0.5 effect size with 80% power at the 5% level of significance. Thus, the sample sizes of 66 and 35 shoulders in the Bristow (group B) and Latarjet (group L) groups, respectively, were considered acceptable.
Results
Patient Characteristics
Of the 151 candidate shoulders, 50 were excluded from evaluation for the following reasons: isolated Bankart repair (n = 37), Bankart repair with a remplissage (n = 8), isolated capsular repair (n = 2), revision after Latarjet (n = 1), rotator interval closure (n = 1), and loss to follow-up within 2 years (n = 1). Thus, 101 shoulders of 91 patients were included in the study. The Bristow procedure was performed in 66 shoulders (group B) and the Latarjet procedure in 35 shoulders (group L). There were no significant differences between the groups in age at surgery, preoperative diagnosis, GBL, or GBL grade (Table 1). The mean overall follow-up time was 70.0 ± 22.5 months (group B, 73.5 ± 2.7 months; group L, 63.5 ± 3.7 months; P = .34).
Patient Characteristics a

a Data are reported as mean ± SD [95% CI] or n (%). GBL, glenoid bone loss.
Relationship Between Clinical Outcomes and GBL
Preoperative ASES and Rowe scores were significantly worse in group B than group L (ASES score, 48.0 ± 14.6 vs 60.8 ± 9.0, respectively, P < .0001; Rowe score, 30.6 ± 14.7 vs 38.7 ± 6.2, respectively, P = .009); however, significant differences were not seen postoperatively (group B vs group L: 91.0 ± 10.2 vs 90.2 ± 13.4 for ASES [P = .82]; 88.5 ± 13.8 vs 86.4 ± 15.1 for Rowe score [P = .57]). All postoperative scores in both groups were significantly better compared with preoperative scores (P < .001 for all) and exceeded previously reported minimal clinically important differences. 20,26 In addition, the postoperative WOSI and patient satisfaction rate were similar in the 2 groups (group B vs group L: 402 ± 326 vs 402 ± 303 for WOSI [P = .87]; 92.0% ± 12.5% vs 94.3% ± 10.7% for patient satisfaction [P = .27]). Time to RTP was significantly shorter in group L than group B (4.8 ± 1.1 vs 5.8 ± 1.8 months, respectively; P = .002).
There were no significant correlations between the extent of GBL and postoperative outcomes (Table 2).
Correlation Between Preoperative Glenoid Bone Loss and Postoperative Outcomes a

a ASES, American Shoulder and Elbow Surgeons; RTP, return to play; WOSI, Western Ontario Shoulder Instability Index.
Graft Conditions at Final CT Examination
Table 3 shows the coracoid graft conditions at the final CT (mean time until final CT: group B, 10.4 ± 7.4 months; group L, 12.1 ± 4.4 months; P = .01). In group B, insufficient union and graft translocation were confirmed in 8 shoulders (12.1%) and 4 shoulders (6.1%), respectively, but in group L, no shoulders had insufficient union and only 1 shoulder (2.9%) had a translocation. In particular, among the cases with grade 0 or 1 GBL (group B, 32 shoulders; group L, 18 shoulders), 5 shoulders (15.6%) showed insufficient union and 3 shoulders (9.4%) had translocation in group B, but in group L, no shoulders had insufficient union or translocation. The rate of graft failure (insufficient union or translocation) in group B was not significantly higher among shoulders with grade 0 or 1 GBL than among those with grade 2 or 3 (25.0% vs 11.8%, respectively; P = .21). In the subanalysis of the final graft conditions, shoulders with insufficient union or translocation of the graft appeared to have a worse score or delayed RTP compared with those with graft union, although statistical comparisons could not be performed because of the small number of cases with graft failure (Table 4).
Final Postoperative Graft Condition by Preoperative GBL Grade a
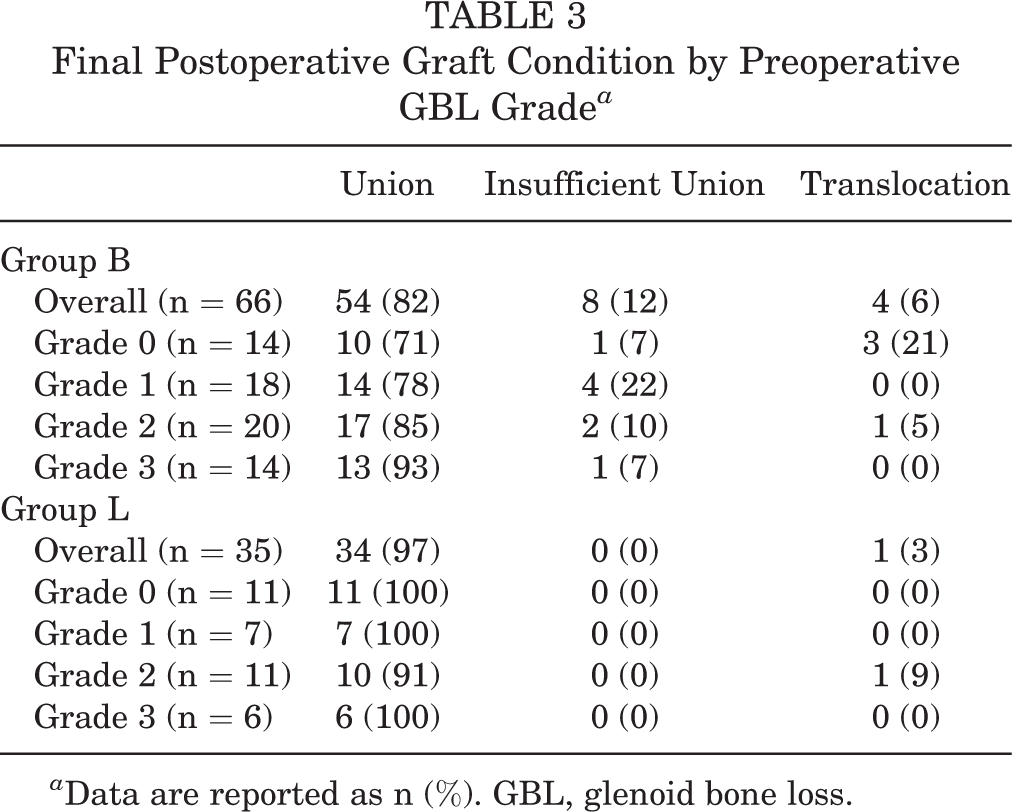
a Data are reported as n (%). GBL, glenoid bone loss.
Final Postoperative Graft Condition by Outcome Measure a

a Data are reported as mean ± SD except for the column of Translocation in Group L, which included only one shoulder. ASES, American Shoulder and Elbow Surgeons; N/A, not available; RTP, return to play; WOSI, Western Ontario Shoulder Instability Index.
Postoperative Recurrence
Postoperative recurrence occurred in significantly fewer shoulders in group B than in group L (2 [3.0%] vs 5 [14.3%], respectively; P = .047). One patient with graft failure in group B and 1 patient with a consolidated bone graft in group L required revision surgery. Four of the 5 cases of recurrence in group L were grade 0 GBL, and complete graft union had been achieved in all 5 shoulders. In group L, postoperative recurrence was not significantly different between shoulders with small and large GBL (grade 0 or 1, 22.2% vs grade 2 or 3, 5.9%; P = .34), which means GBL had no significant effect on recurrence.
Other Complications
Two shoulders in group B had superficial infection, another 2 developed postoperative hematomas, while there was 1 superficial infection in group L. In all cases, preoperative GBL was grade 0 or 1. All patients were treated nonoperatively. No cases of nerve palsy were observed in either group.
Discussion
The most important findings of this study were that, in competitive rugby players, CPT combined with a Bankart repair results in a favorable outcome regardless of the extent of preoperative GBL or CPT procedure and that the time to RTP is significantly shorter after the Latarjet procedure than after the Bristow procedure.
In general, CPT is used to reconstruct bone defects in the glenoid and achieves good postoperative results in cases of anterior shoulder instability with a large GBL. 2,21 Because the conventional indication for CPT is a GBL of 20% 39 or 25% or more, 18 the few previous studies on combining CPT with a Bankart repair included patients, only younger patients who were collision athletes without considering the extent of GBL. Kawasaki et al 15 reported an association between lower postoperative functional scores and the extent of GBL after Bristow procedures combined with a Bankart repair in competitive rugby players. Their colleagues, Shibuya et al, 31 reported on a similar study that included shoulders treated with either the Bristow or the Latarjet procedure and found an association between the simultaneous presence of a low Rowe score and a high WOSI, which they defined as “functional failure,” and the extent of GBL. On the other hand, Tasaki et al 33 compared postoperative outcomes in 2 groups, one with <10% GBL and the other with >10% GBL, and concluded that GBL does not influence postoperative outcomes. Therefore, the influence of the preoperative extent of GBL on outcome after CPT combined with a Bankart repair was still a controversial topic. Our data indicated that the extent of GBL does not influence postoperative clinical outcomes. In this study, even cases with a GBL >20% showed acceptable postoperative outcomes, indicating that CPT accompanied by a Bankart repair has an excellent stabilizing effect, regardless of the amount of GBL.
A previous review found a graft nonunion rate after CPT of almost 10%, 9 which is consistent with our current study. Di Giacomo et al 11 investigated the graft resorption rate after the Latarjet procedure and concluded that shoulders without GBL had significantly more graft resorption than those with >15% GBL. Although their report did not identify the difference in graft union rate, greater GBL appeared to be more advantageous for the prevention of graft resorption. On the other hand, the current study directly evaluated graft union and demonstrated that the Latarjet procedure is a reliable technique in terms of graft union regardless of the extent of GBL and can lead to an earlier RTP in rugby players. This difference was because of the faster bone union in the Latarjet procedure, as shown in a previous study. 32 However, in contrast, the Bristow procedure showed an inferior graft union rate compared with the Latarjet procedure. Previously, Willemot et al 37 summarized the cases that led to revision surgery after Bristow or Latarjet procedures. Their results implied that graft failures after the Bristow procedure occurred in cases without GBL or with only a small amount of GBL. Although screw length and insertion angle against the glenoid face have been reported as risk factors for graft failure after the Bristow procedure, 4 the present study is the first to evaluate an association between the amount of GBL and graft failure. We could not statistically determine the influence of GBL on graft failure in either group because of the underpowered analysis. However, if the GBL is absent or small, graft placement is likely to be poor in the Bristow procedure, as shown in Figure 1, which may cause graft failure. To avoid poor graft placement in cases with no GBL or a small GBL, the operative procedure may require some modification such as cutting the coracoid graft obliquely to fit the slope of the anterior glenoid neck before grafting.

Relationship of the grafted coracoid process to the glenoid before and immediately after the Bristow procedure in 2 representative cases. (A) Image obtained in a 19-year-old male patient without glenoid bone loss (GBL). Arrow indicates a gap between the graft and the glenoid. (B) Image obtained in an 18-year-old male patient with GBL accompanied by a bony Bankart lesion. Arrow indicates no gap.
The results of our subanalysis did not indicate a statistically significant difference in the relationship between graft failure and GBL or its clinical outcome. However, clinical scores in the graft failure group were relatively poor, and there was a tendency for graft failure in shoulders with a GBL ≤10% that underwent the Bristow procedure. This finding might be considered by surgeons in selecting surgical procedures for anterior shoulder instability in young collision athletes and should be proved in future studies with an adequate statistical power. However, the extent of GBL was not correlated with clinical scores in group B, indicating that this technique is reliable enough to treat patients with large glenoid defects.
Limitations
This study has several limitations. First, it was not a prospective randomized trial but a retrospective cohort case-control study. The comparison of preoperative clinical status in groups B and L showed worse status in patients who underwent the Bristow procedure. Although postoperative scores were not significantly different between groups, the preoperative differences might have affected these results. In addition, group L had fewer patients than group B, so the effects of the Latarjet procedure might have been underestimated. There was also a significant difference in time to the final CT scan between groups B and L, which may have affected the assessment of graft condition. Second, group L would have benefitted by having a more experienced surgeon perform their surgery, which might have contributed to the different clinical outcome from group B. Third, the study did not evaluate Hill-Sachs lesions (HSLs), although the location of a HSL might affect postoperative outcomes after surgical treatment of anterior shoulder instability. However, because CPT can change the glenoid track and convert an off-track HSL to an on-track one, 7,27 we believe that any potential negative effect of HSLs localization would have been very small or negligible. Fourth, we could not perform statistical comparisons in our subanalysis because of the quite small numbers of graft failures. The influence of graft failure itself on clinical outcomes should be evaluated in further studies.
Conclusion
The findings of this study indicated that the extent of GBL does not affect clinical scores after CPT, regardless of operative procedure.
Footnotes
Final revision submitted February 9, 2023; accepted February 26, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Daini Osaka Police Hospital (reference No. 1054).