
Abstract
Purpose:
In this study, we aimed to reveal the individual differences regarding the size of the coracoid and their effects on the classical and modified Latarjet procedures.
Methods:
Computed tomography images of 120 patients (mean age: 41.18 ± 12.01 years) without shoulder complaints or shoulder instability were evaluated retrospectively. The glenoid width, the surgical graft length, and the coracoid total length, width, and thickness were measured using the multiplanar reconstruction method on the Sectra Picture Archiving and Communications System (PACS) system. Age, gender, side, the dominant hand, and the height of the patients were recorded and the correlations between them were investigated. On the created hypothetical model, the current size of the coracoid was evaluated to determine what size of glenoid defects it could repair by employing the classical and the modified Latarjet techniques.
Results:
There was no significant difference between the right-hand-dominant group and the left-hand-dominant group in terms of coracoid measurement results (p > 0.05). Again, there was no statistically significant difference between the right and the left side regarding the coracoid size (p > 0.05). A positive correlation could be detected only between age and the coracoid width and thickness (p < 0.05). A positive correlation was also found between the glenoid width and the coracoid width and thickness in both shoulders (p < 0.001). Coracoid thickness could fill in the defects that amounted to 40% of the glenoid width, while the coracoid width could fill in for the defects that were 50% of the glenoid width in both genders.
Conclusion:
Our study showed that hand dominance and side were not effective on the coracoid dimensions. In addition, it has been shown that the coracoid dimensions did not have a significant effect in the choice of Latarjet technique in terms of defect repair and that repair rates of up to 40% could be achieved in glenoid defects with both techniques.
Introduction
Soft tissue procedures are often insufficient in cases of glenohumeral instability with significant bone loss, which usually refers to the defects that cover more than 20% of the glenoid width. 1 –3 In the classical technique used today, the inferior surface of the coracoid is fixed to the glenoid, whereas in the modified technique the coracoid is first rotated 90° and then its medial surface is fixed to the glenoid. 4,5 Thus, in the classical technique, the glenoid defect is repaired by the thickness of the coracoid, while in the arc modification technique the width of the coracoid is utilized. 6 –8
It is seen that the size of the coracoid bone exhibits individual differences in the context of races and genders; the presence of a smaller bone morphology, as is the case in Asians, is a source of concern for surgical procedures. 9 –11 In Latarjet operations, knowing the dimensions of the coracoid bone is of utmost importance both in obtaining glenohumeral stability and in complications such as fracture development or nonunion after coracoid transfer. 12 –14
We hypothesized that hand dominance and side differences would not affect the coracoid dimensions and that the coracoid dimensions would not have a significant effect on the classical and modified Latarjet procedures.
Materials and methods
Patient population
Our study was approved by the Ethics Committee of the Faculty of Medicine at a State University in Turkey. A total of 140 patients were evaluated for the study. Both shoulders of the subjects were evaluated retrospectively on the thoracic computed tomography (CT) images in the picture archiving and communication system (PACS) of our hospital. The patients were interviewed on the phone and a total of 120 patients (65 males and 55 females) who were between the ages of 18 and 60 years, who had no degenerative, traumatic, or congenital shoulder problems that could affect the bone anatomy, and who had not undergone a surgery of the shoulder region were included in the study. None of the cases had shoulder complaints or a history of shoulder instability. Twenty cases who did not meet the inclusion were excluded from the study; the study was conducted with the inclusion of 120 cases (Figure 1).
Flowchart of the inclusion criteria for the study.
CT acquisition and protocol
The CT scans were performed using a multidetector CT scanner (Aquilion™ PRIME; Canon Medical Systems, Tokyo, Japan). Thoracic CT examination was performed by lifting the patient’s arms above the head. The thorax CT parameters were as follows: kV: 120, mAs: 80, collimation: 1.25 × 1.25 mm2, pitch: 1, FOV: 20 × 20 cm2, matrix: 512 × 512, and slice thickness: 1 mm.
Imaging assessment
Raw data were processed by a radiologist with 8 years of experience on the Sectra PACS system (Sectra AB, Linköping, Sweden), and multiplanar reconstruction (MPR) images were obtained. The measurements were made collectively by an orthopedist and a radiologist using the axial and oblique sagittal planes on CT images that included both shoulders. These planes were created by using MPR technique, by obtaining oblique sagittal view, it provided the measurement of the Coracoid process (CP) length. The length from the coracoid tip to the base was considered as the “total length,” and the length from the tip to the knee, where the horizontal and vertical parts of the coracoid bone meet, was accepted as the “surgical graft length” (Figure 2).

MPR of the CT image is obtained by manipulating the axial (a) and oblique coronal (b) views of the right shoulder in order to consist a true sagittal view of CP (c). The lengths of CP (arrows) are shown on oblique sagittal view. Black arrow indicates surgical length and white arrow indicates total length. MPR: multiplanar reconstruction; CT: computed tomography.
Again, by using MPR function, in order to measure the mediolateral width and craniocaudal thickness of CP, a true oblique coronal image perpendicular to the axis of CP was obtained. The coronal sections were matched with the axial sections and the superior and inferior widths were measured at 1 cm intervals on the graft. The thickness was measured at the midpoint between the knee and the tip of the coracoid (Figure 3). The glenoid width measured on the axial sequences was accepted as the highest measurement (Figure 4).

A true oblique coronal plane was consisted in MPR of oblique axial (a) and sagittal (b) views of the right shoulder. The medial–lateral width (black arrow) and superior–inferior thickness (white arrow) of CP were measured on true oblique coronal view (c). In the same MPR setting at oblique sagittal view, the width was measured by determining the superior and inferior points and the thickness was measured by determining the midpoint (b). MPR: multiplanar reconstruction.

CT axial image shows the glenoid width. CT: computed tomography.
The side, age, gender, hand dominance, and length data were recorded for comparison. On the created hypothetical model, the current size of the coracoid was evaluated to determine what size of glenoid defects it could repair by employing the classical and the modified Latarjet techniques. Inter- and intraobserver reliabilities were evaluated.
Statistical analyses
Statistical analyses were performed using the SPSS version 17.0 software. The accordance of the variables with normal distribution was examined by histograms and the Kolmogorov–Smirnov test. The mean, standard deviation, and median values were used in descriptive analyses. Comparisons were made in 2 × 2 grids using the Pearson’s χ 2 and Fisher’s exact tests. Intergroup comparison of the variables that showed normal distribution (parametric variables) was performed using independent samples t-test, while the Mann–Whitney U test was used for the variables that didn’t show normal distribution (nonparametric variables). Spearman’s correlation was used to analyze the measured data with each other. Cases where the p value was less than 0.05 were evaluated as statistically significant.
Results
Of the 120 subjects in our study, 65 were males (54.2%) and 55 were females (45.8%), with a mean age of 41.2 ± 12.0 years. Ninety patients (75%) were right-hand dominant and 30 were left-hand dominant (25%).
The coracoid length, width, and thickness were significantly higher in males (p < 0.001) (Table 1). There was no significant difference between the right-hand-dominant group and the left-hand-dominant group in terms of coracoid measurement results (p > 0.05). Again, there was no statistically significant difference between the right and the left side regarding the coracoid size (p > 0.05).
Dimensional measurements of the coracoid and the glenoid.a

GW: glenoid width; IW: inferior width; L: left side; R: right side; SD: standard deviation; SL: surgical length; SW: superior width; T: thickness; TL: total length.
a Significant p values are given in bold.
b Independent samples t-test.
c Mann–Whitney U test.
While there was a positive correlation between the patients’ height and all dimensions of the coracoid (r: 0.452–0.652) (p < 0.001), a positive correlation was detected only between age and the coracoid width and thickness (r: 0.298–0.406) (p < 0.05) (Table 2).
Spearman’s correlation of age and height with the coracoid dimensions.a
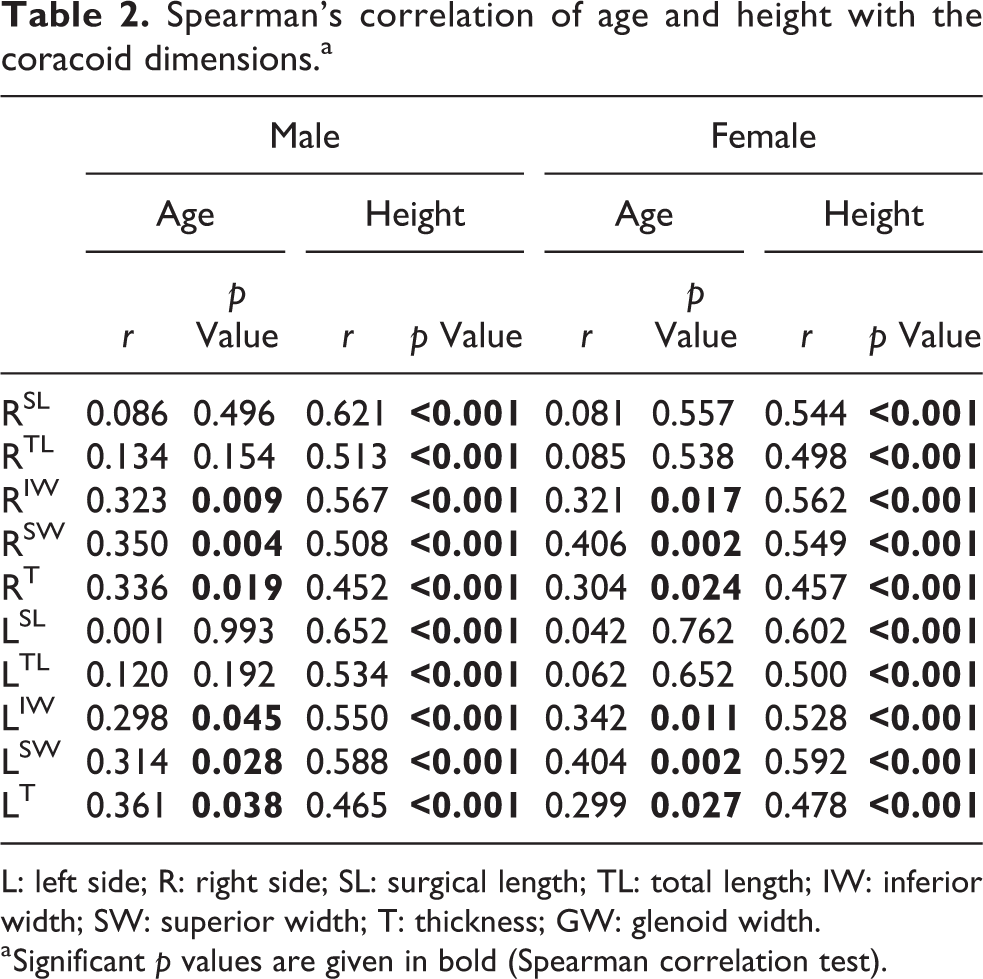
L: left side; R: right side; SL: surgical length; TL: total length; IW: inferior width; SW: superior width; T: thickness; GW: glenoid width.
a Significant p values are given in bold (Spearman correlation test).
A positive correlation was also found between the glenoid width and the coracoid width and thickness in both shoulders (p < 0.001) (Table 3).
Spearman’s correlation between glenoid dimensions and coracoid dimensions.a

R: right side; L: left side; IW: inferior width; SW: superior width; T: thickness; GW: glenoid width.
a Significant p values are given in bold.
When we used a hypothetical glenoid defect model, we concluded that the coracoid thickness could fill in the defects that amounted to 40% of the glenoid width, while the coracoid width could fill in for the defects that were 50% of the glenoid width in both genders. While the same techniques did not show a statistical difference between the genders (p > 0.05), a significant difference independent from gender was observed between the techniques (p < 0.001) (Table 4).
The glenoid width replaced with the coracoid width and thickness.a

CW: coracoid width; GW: glenoid width; CT: coracoid thickness; SD: standard deviation.
a Significant p values are given in bold (Mann–Whitney U test).
The correlation coefficient for intraobserver reliability was 0.98 (95% confidence interval (CI): 0.98–0.99) and 0.98 (95% CI: 0.98–0.99) for each observer, respectively. The correlation coefficient of interobserver reliability was 0.98 (95% CI: 0.98–0.99).
Discussion
As a result of our study, we presented the coracoid and glenoid dimensions on the 2D CT images in terms of gender, age, side, and hand dominance. We also found that hand dominance had no effect on the coracoid dimensions, a finding we have not previously encountered in the literature. Another main finding of ours was that the coracoid bone could be used as a graft in defects that reached 40% of the glenoid width with the classical Latarjet operation and in defects that reached 50% of the glenoid width with the modified technique.
In the Latarjet operation, the joint curvature and concavity are restored, contact pressure is reduced, and joint stability is achieved with the transfer of the coracoid graft to the glenoid defect. 15 –17 At this point, the transferred bone sizes gain importance since a sufficiently large graft is needed to restore stability as well as to prevent a coracoid fracture and correctly position the screws during surgery. 18,19 In their study, Dumont et al. estimated the fixation surface area on the CT images to be 5.65 cm2 with the conventional Latarjet technique and 3.64 cm2 with the congruent arc Latarjet technique. 20 Failure of Latarjet operations due to small graft size has been reported in the literature. 21
It is known that the coracoid size shows racial differences. Knapik et al. found the width, thickness, and length of the coracoid to be 15.9 mm, 9.2 mm, and 46 mm in the Caucasian race and 15.3 mm, 9.4 mm, and 44.4 mm in Afro-Americans, respectively. 4 Verma et al. obtained 14.5 mm, 7.95 mm, and 35.54 mm with the measurement of the same parameters in the Indian population. 22 In Imma et al.’s study, the same parameters were measured as 13.34 mm, 10.18 mm, and 40.88 mm in males and 10.49 mm, 8.61 mm, and 35.98 mm in females in the Malaysian population. 11 In our study, we measured the width, thickness, and length of the coracoid as 14.22 mm, 11.12 mm, and 45 mm in males and 12.31 mm, 9.68 mm, and 40 mm in females. Accordingly, our findings, other than the thickness of the coracoid, can be placed between those of the Asian and the Caucasian populations. The thickness values in our study were above the values of both populations.
The coracoid measurements in our male subjects were 2 mm wider, 1.5 mm thicker, and 5 mm greater in total length than the female subjects, which showed similarity to previous studies. In their study, Salzmann et al. noted a 2 mm wider, 1.4 mm thicker, and 4 mm greater in total length coracoid in males. 9 Ljungquist et al. found that the surgical coracoid length was 5 mm longer in males. 23 In our study, the surgical lengths differed approximately 4 mm between genders. In Latarjet operations, an adequate graft length is important to allow sufficient bone distance between the screws, otherwise there may be a risk of iatrogenic fracture. 24
Although degenerative and osteophytic cases were not included in our study, a positive correlation was detected between age and the coracoid width and thickness. Dolan et al. used 10 fresh cadavers with an average age of 83.8 years and obtained one of the highest coracoid measurement results in the literature (tip width of 18.3 mm). 25 Similar studies exist in the literature, showing positive correlation between age and the coracoid length, width, and thickness. 4
It is known that the coracoid width is larger than its thickness in all cases. The width is the reason for a successful screw placement and fixation in the classical Latarjet operation and the reconstructability of larger glenoid defects in the modified Latarjet technique. 26,27 While Montgomery et al. 5 showed that glenoid defects up to 36% could be repaired by the conventional technique and 50% by the modified technique in a cadaver study, Armitage et al. 26 reported that defects up to 36% could be repaired with the classical technique and 53% with the modified technique. Although there is still no consensus about the coracoid transfer technique, 13 our study showed that up to 40% of the glenoid defects could be repaired by providing a safe fixation using the classical technique.
Similarly, size differences between genders can lead to difficulties and complications during the coracoid transfer. The coracoid dimensions in females pose potential challenges, particularly in the modified Latarjet technique. 5 In the presence of a smaller coracoid, it may be more appropriate to opt for the classical technique because of the risk of postoperative graft failure. In addition, although it has been reported that hand dominance has an effect on bone dimensions in the upper extremity, we found that it did not affect the coracoid dimensions in our study. 28
Some limitations of our study should be kept in mind. Our measurements were made on oblique sequences that allow for better bone size measurement by making MPRs. Thus, values close to real bone sizes were obtained. The average age of our study group could have been lower. Although a similar decortication procedure was applied in both techniques before the fixation of the graft to the glenoid surface, our study was not a cadaver or surgical study. Thus, we compared the two Latarjet techniques using the hypothetic model created by using the CT data. In our study, only the bone effect was taken into consideration, the dynamic effect of the soft tissues and muscles was not evaluated. Although the width values were calculated at the possible screw application spots, the thickness was measured only at the midpoint. While our study group does not represent the global population, it provides important information about individual coracoid differences and their impact on Latarjet operations.
Conclusion
Based on the results of our study, we can assert that hand dominance does not have an effect on the coracoid morphology. The individual differences observed in our study should be taken into consideration before Latarjet operation in order to avoid possible complications and the appropriate technique should be determined by taking the defect size and coracoid dimensions into consideration.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval was obtained from the Ethical Review Committee of Namık Kemal University with the following number: 24.09.2019–2019.171.09.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.