
Abstract
Background:
Although surgical shoulder stabilization via coracoid transfer in collision athletes is effective and has a low reinjury rate, the factors affecting poor clinical results and the superiority of the 2 stabilization procedures (Bristow and Latarjet) remain unclear.
Purpose:
To explore the factor(s) affecting poor clinical results of coracoid transfer in a large cohort of rugby players and to compare postoperative function between the Bristow and Latarjet procedures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This study included 169 consecutive shoulders of 154 competitive male rugby players who underwent shoulder stabilization surgery (Bankart repair with coracoid transfer) between 2014 and 2018 and had a mean follow-up of 2.7 years (minimum follow-up, 2 years). The Bristow procedure was performed in the first 92 shoulders (84 players), and the Latarjet procedure was performed in the latter 77 shoulders (70 players). A poor clinical result was defined as a postoperative Rowe score of <70 and a postoperative Western Ontario Shoulder Instability Index (WOSI) score of >630. Multiple logistic regression analysis was conducted to identify the factors affecting postoperative functional failure. The postoperative scores and complication rates were also compared between the 2 procedures.
Results:
In total, 92.3% of the rugby players returned to their preinjury competition level at a mean of 5.9 months postoperatively. The Rowe and WOSI scores showed that shoulder function was improved postoperatively compared with preoperatively. The number of rugby players with a poor clinical result was 18 (10.7%). Multiple logistic regression analysis demonstrated that a poor clinical result was associated with a preoperative glenoid bone defect of >20% of the glenoid width (odds ratio, 9.8), whereas the clinical result was unaffected by the type of coracoid transfer. There were no differences between the 2 procedures in any of the postoperative scores or complication rates.
Conclusion:
The present study indicated that the most effective predictor of postoperative functional scores was the degree of the glenoid bone defect and not the type of coracoid transfer. This information may be useful for the strategic treatment of shoulder dislocations in collision athletes.
Keywords
For collision athletes, including rugby players, shoulder instability causes many missed training days, and a reinjury negatively affects player performance and long-term career success. 3,4,19 Coracoid transfer reportedly results in superior outcomes to arthroscopic Bankart repair in collision athletes, irrespective of the presence of an osseous lesion. 17 Coracoid transfer can be performed using either the Bristow procedure or the Latarjet procedure; these are nonanatomic reconstruction techniques that transfer the coracoid process to the anteroinferior portion of the glenoid rim to augment anatomic repair via their sling effect and bone coverage. 15,25,26,28,39 The main difference between the 2 procedures is that the coracoid is fixed perpendicular to the glenoid’s long axis using a single screw in the Bristow procedure, whereas it is fixed parallel to the glenoid’s long axis using 2 screws in the Latarjet procedure. Cadaveric studies have demonstrated that the Latarjet procedure achieves better biomechanical results than does the Bristow procedure 13,36 ; however, both procedures have equivalent stabilizing effects on unstable shoulders with a preserved glenoid osseous anatomy. 13 Recent systematic reviews have demonstrated that the clinical outcome does not significantly differ between the 2 procedures 7,10 ; however, a comparison of clinical outcomes in a cohort of rugby players has not been reported. In addition, several studies have demonstrated that Bankart repair combined with coracoid transfer yields excellent results in most cases, 23,27,31,34 but the factors affecting postoperative shoulder outcomes remain unknown. Although studies have demonstrated that large glenoid bone defects affect clinical outcomes after arthroscopic Bankart repair, 8,32 it remains unclear if large glenoid bone defects affect clinical outcomes after coracoid transfer.
The purpose of the present study was to identify the factor(s) affecting postoperative functional failure in a cohort of rugby players with shoulder instability and to compare postoperative function between the Bristow and Latarjet procedures. We hypothesized that large bone defects of the glenoid may be a specific factor affecting poor clinical outcomes and that the clinical outcome would be equivalent after both procedures.
Methods
Patients
Between 2014 and 2018, a total of 252 collision athletes (ie, athletes involved in football, rugby, judo, and sumo) with unstable shoulders underwent coracoid transfer via Bankart repair for shoulder stabilization by a single surgeon (T.Kawasaki). After performing many Bristow procedures and evaluating the results, 18 we changed the technique to investigate the therapeutic effects of the Latarjet procedure from late 2016 onward. Thus, shoulder stabilization was achieved via the Bristow procedure in the first 143 shoulders of 132 collision athletes, while the Latarjet procedure was performed in the subsequent 127 shoulders of 120 collision athletes. Of this cohort, we included 169 shoulders in 154 rugby players who met the following study inclusion criteria: (1) had at least 1 episode of a shoulder dislocation or subluxation, (2) were competitive male rugby players who wanted to return to play, (3) had a minimum 24-month follow-up period, and (4) had clinical data available from medical records. Recreational rugby players, collision athletes who played a sport other than rugby, and rugby players who had undergone any previous shoulder surgery were excluded from the present study.
All patients provided informed consent for study participation. This study was approved by the institutional review board of our hospital.
Preoperative Planning
The indications for coracoid transfer in addition to Bankart repair were rugby players with a history of shoulder instability (subluxation or dislocation) and objective evidence on computed tomography (CT) of a Bankart lesion and/or Hill-Sachs lesion. Coracoid transfer was also performed when an engaging Hill-Sachs lesion was observed arthroscopically. Patients with no subjective instability, no CT findings suggestive of Hill-Sachs lesions, and no obvious shoulder dislocation during an arthroscopic evaluation underwent arthroscopic Bankart repair; such patients were excluded from this study.
Surgical Procedures
The Bristow and Latarjet procedures were performed as described previously. 15,24,25,28,39 A deltopectoral approach was used with a 3- to 4-cm incision. After separation of the soft tissues, osteotomy of the coracoid process was performed at <1 cm from its tip for the Bristow procedure or at the junction between its horizontal and vertical regions for the Latarjet procedure. The subscapularis muscle and anterior capsule were horizontally divided to expose the anterior region of the glenoid and the Bankart lesion, including the labrum and anterior periosteal sleeve. The anteroinferior cortex of the glenoid was deepened by approximately 3 to 5 mm to provide an indented bed of cancellous bone adjacent to the glenoid rim for placement of the coracoid graft; this cancellous bone bed was rectangular and approximately 8 mm long for the Bristow procedure and 20 mm long for the Latarjet procedure. For the Bristow procedure, the osteotomized surface of the coracoid was fixed to the anterior surface of the glenoid using a single cannulated cancellous screw. For the Latarjet procedure, the inferior surface of the coracoid was fixed to the anterior surface of the glenoid using 2 cannulated cancellous screws. The coracoid was fixed so that it lay flush with the glenoid face. In most cases, 4.0 mm–diameter cannulated cancellous screws (Meira) were used. After fixation of the coracoid, anatomic Bankart repair was performed using 2 to 3 anchors (1.5 mm–diameter JuggerKnot; Zimmer Biomet), and the joint capsule was attached near the transferred coracoid process to restore appropriate tension. When necessary, other intra-articular lesions, including humeral avulsions of the glenohumeral ligament and superior labral anterior-to-posterior lesions, were treated before shoulder stabilization was performed.
The shoulder was immobilized in a sling in internal rotation for 4 weeks postoperatively. Passive rehabilitation was immediately started under the guidance of a physical therapist. Active exercises were started at 4 weeks postoperatively, and normal activities of daily living were allowed thereafter. CT was conducted to ensure bone healing of the coracoid graft at 12 weeks postoperatively (Figure 1). A strengthening program followed by rugby practice was then begun, and full return to play was allowed at 5 months postoperatively. If bone healing was not evident at 12 weeks postoperatively, CT was repeated at 16 weeks postoperatively, and a strengthening program was initiated, regardless of the presence of bone union.

Three-dimensional computed tomography reconstruction of the glenoid after the (A) Bristow procedure and (B) Latarjet procedure.
Data Collection
After the usual postoperative follow-up period of 12 months, the participants were monitored via annual follow-up examinations, with additional examinations if there were any problems. Annual follow-up examinations included outcome measures including the Rowe score 30 and the Western Ontario Shoulder Instability Index (WOSI). 14,20 To evaluate the current condition of the affected shoulders, the participants were also asked to complete a questionnaire containing these functional measures at the beginning of 2020. All postoperative data were collected and evaluated by a single senior author (T.Kawasaki).
The age at first injury and at surgery, number of shoulder dislocations and subluxations before surgery, competition level, degree of glenoid bone defects, 33 competition level after surgery, time to full return to play after surgery, and postoperative complications were obtained from the medical records and questionnaire results. The presence and size of Hill-Sachs lesions were noted before surgery, but we did not change the procedure based on the size of the lesion. Shoulder hyperlaxity was defined as external rotation of >90° with the arms at the side (reaching the frontal plane) in the unaffected shoulder. 2 A reinjury after surgery was defined as an injury with a clear onset, followed by a clinical diagnosis of shoulder instability. Competition levels were classified as either Division I (the highest division league in each category, including international players) or Division II (lower-grade competition levels).
Statistical Analysis
In the analysis, age at first injury and at surgery, body mass index, and preoperative and follow-up scores were treated as continuous quantitative data, while the incidences of shoulder dislocations and subluxations were divided into 3 ordinal categories. Preoperative bone defects of the glenoid 33 were also divided into 5 ordinal categories (≤6.0%, 6.1%-10.7%, 10.8%-14.3%, 14.4%-20.1%, and ≥20.2%), while other variables were simply defined as being positive or negative. In accordance with a previous study, 18 shoulders defined as having “functional failure” had both a Rowe score of <70 and a WOSI score of >630. Complications were determined from the medical records and responses to the study questionnaire and included reinjuries after surgery, severe joint contracture, surgical site infections, coracoid detachment, and nerve palsy. Nonunion of the transferred coracoid process was also documented, although this condition was usually asymptomatic. For all analyses, normally distributed numeric variables were expressed as means and 95% CIs, other numeric variables were expressed as medians and interquartile ranges, and binominal variables were expressed as ratios.
For the main analysis, data from the entire cohort were entered into multiple logistic regression analysis to determine the odds ratios (ORs) for multivariate factor(s) affecting postoperative “functional failure” as defined earlier. Confounders were selected as appropriate, and the multicollinearity of each independent variable was checked by calculating each correlation before analysis. The independent variables were age, body mass index, competitive level, total number of instability events, level of sport (high school/collegiate/professional), player’s position (forward/back), presence of hyperlaxity, and whether the affected shoulder was on the dominant or nondominant side. The goodness of fit for each final estimate was assessed using the omnibus and Hosmer-Lemeshow tests. 16 In addition, receiver operating characteristic curves were constructed to ascertain the sensitivity and specificity for the threshold of the glenoid bone defect size that predicted postoperative functional failure.
For the subanalysis, the postoperative Rowe and WOSI scores were compared using the Mann-Whitney U test. A statistical power analysis was performed, and the estimated effect size (d) of the comparison was 0.60 when the error probability (α) was .05 and the power (1 – β) was 0.95. 6 The complication and reinjury rates after each procedure were also compared using the chi-square test. All analyses were conducted using SPSS for Mac (Version 21; IBM Corp). Differences were considered statistically significant at P < .05.
Results
Descriptive data are presented in Table 1. A total of 169 shoulders in 154 competitive rugby players with a mean follow-up of 2.7 years were included in the analyses. Of these, 18 (10.7%) belonged to international rugby players. Overall, 92.3% of the rugby players returned to their preinjury competition level at a mean of 5.9 months after surgery. Ultimately, 92 shoulders were treated using the Bristow procedure, and 77 shoulders were treated using the Latarjet procedure. There were no significant differences in patient characteristics between the procedures (Table 1).
Descriptive Data

a Data are reported as mean (95% CI) or mean (95% CI) [median] unless otherwise indicated. P values were calculated using the t test unless otherwise indicated.
b Chi-square test.
The Rowe and WOSI scores showed that shoulder function improved postoperatively (Table 2). CT performed at 3 months postoperatively revealed nonunion of the transferred coracoid process in 9.5% (16/169) of the shoulders, comprising 10 of the 92 (10.9%) shoulders treated via the Bristow procedure and 6 of the 77 (7.8%) shoulders treated via the Latarjet procedure; however, none of the affected patients experienced problems. A postoperative reinjury occurred in 2 of 169 shoulders (1.2%; all subluxations), both of which had undergone the Bristow procedure; none of the shoulders treated via the Latarjet procedure were reinjured. Additionally, 3 shoulders (1.8%) developed surgical site infections, which required a single surgical debridement procedure, followed by at least 3 months of oral antibiotics. Further, 3 shoulders (1.8%) developed severe contracture, which required manipulation under local anesthesia, and 3 shoulders (1.8%) developed coracoid detachment, which required a reoperation within 1 month after the first surgical procedure (Table 2). The overall rate of complications (adverse events) was 6.5% for each procedure, as complications occurred in 6 of 92 shoulders treated via the Bristow procedure and 5 of 77 shoulders treated via the Latarjet procedure.
Postoperative Outcome Scores and Complications a

a Data are reported as mean (95% CI) [median] unless otherwise indicated. P values were calculated using the Mann-Whitney U test unless otherwise indicated. Rowe score (maximum, 100): stability (maximum, 50), range of motion (maximum, 20), and function (maximum, 30). WOSI score (maximum, 2100): physical symptoms (maximum, 1000), sports/recreation/work (maximum, 400), lifestyle (maximum, 400), and emotions (maximum, 300). WOSI, Western Ontario Shoulder Instability Index.
b Chi-square test.
In total, 18 (10.7%) players displayed postoperative functional failure as indicated by the Rowe and WOSI scores. The rate of functional failure in each category of glenoid bone defect size is shown in Figure 2. About 25% of patients with glenoid bone defects of >20% were considered functional failures. Multiple logistic regression analysis was performed to explore the factor(s) that affected postoperative functional failure. The final goodness-of-fit estimates showed that 90.4% of cases were correctly predicted. Multiple logistic regression analysis also showed that a glenoid bone defect of >20% of the glenoid width was associated with postoperative functional failure in the affected shoulder (OR, 9.8), whereas the outcome was not affected by the other variables tested including the type of surgical procedure (ie, Bristow or Latarjet) (Table 3). The receiver operating characteristic curve demonstrated the fraction of true-positive results (sensitivity) and false-positive results (1 – specificity) for various cutoff values of the glenoid bone defect (Figure 3). When the cutoff value of the glenoid bone defect was 20% of the glenoid width, the sensitivity and specificity were 33.3% and 88.7%, respectively (P = .02). The subanalysis demonstrated that there were no significant differences between the 2 procedures regarding postoperative shoulder function or the frequency of total complications (Table 2).
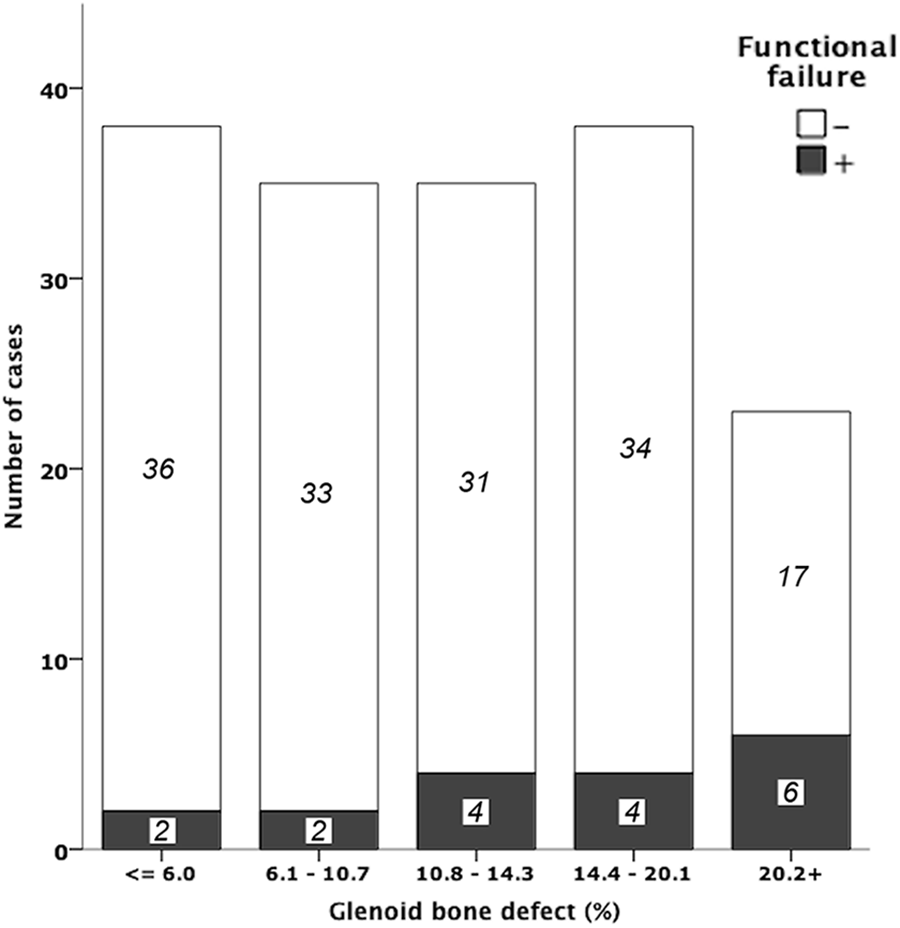
Rate of functional failure in each category of the glenoid bone defect. Functional failure was defined as a Rowe score of <70 and a Western Ontario Shoulder Instability Index score of >630.

Receiver operating characteristic (ROC) curve for postoperative functional failure (area under the curve = 0.67).
Results of Multiple Logistic Regression Analysis to Identify Factors Influencing Functional Failure a

a OR, odds ratio.
b Adjusted for body mass index, age at surgery, and preoperative and postoperative period.
c Statistically significant.
Discussion
Factors Affecting Postoperative Function After Shoulder Stabilization in Rugby Players
Multiple logistic regression analysis revealed that a glenoid bone defect of >20% of the glenoid width negatively affected postoperative shoulder function (OR, 9.8). It is widely accepted that a large bone defect itself impairs shoulder stability. A previous biomechanical study demonstrated that reconstruction of the glenoid concavity is needed when an anterior glenoid defect approaches 25% of the glenoid width. 38 However, as found in cadaveric studies, several clinical studies have indicated that the degree of bone defect in the affected shoulder is a risk factor for recurrence and a worse condition after stabilization surgery. 5,8,32 Although coracoid transfer is a reasonable solution to correct a glenoid bone defect, the present study indicated that coracoid transfer did not achieve complete stability in the shoulders with a glenoid bone defect of >20% of the glenoid width, even with the Latarjet procedure. Therefore, the present results suggest that shoulder surgeons should recommend early surgery before extensive glenoid bone defects develop. The present study also revealed that the presence of a glenoid bone defect of >20% of the glenoid width had low sensitivity (33.3%) and high specificity (88.7%) for predicting functional failure after coracoid transfer. This implies that the negative effects of large glenoid bone defects were clinically significant, although some patients with large glenoid bone defects did not experience functional failure of the affected shoulder. Further research is needed to explore these issues.
The 2 coracoid transfer techniques used in the Latarjet procedure are the “classic” technique, in which the inferior surface of the coracoid is fixed to the anterior surface of the glenoid, and the “congruent arc” technique, in which the coracoid is rotated 90° so that the medial aspect of the coracoid is fixed to the glenoid and the inferior aspect of the coracoid becomes congruent with the articular surface of the glenoid. Biomechanical studies have demonstrated that the “classic” technique has a greater contact area and initial fixation whereas the “congruent arc” technique achieves larger restoration of the glenoid surface. 11,26 Considering that the “classic” technique was applied in the Latarjet procedure in all cases in the present series, the “congruent arc” technique of the Latarjet procedure may be preferable in shoulders with a glenoid bone defect of >20% of the glenoid width. Other alternatives for bone defects include an iliac crest graft, 35 distal clavicle graft, 21 or distal tibial allograft 29 ; however, simply fitting the bone in the en face view is probably not sufficient and would require the concavity of the joint to be matched.
Coracoid transfer is thought to stabilize the shoulder via 3 distinct mechanisms: bone block, sling effect, and capsule re-establishment. 38 Although the dynamic sling effect of the subscapularis muscle and transferred conjoint tendon is considered a main contributor to shoulder stabilization, the natural action of the subscapularis muscle is lost. In addition, a biomechanical cadaveric study indicated that the sling effect has its maximum stabilizing effect at the end-range arm position but has less stabilizing action at the midrange position. 37 Another cadaveric study demonstrated that coracoid transfer stabilized the midrange shoulder position only when proper tension was applied during placement. 12 Although these findings have not been confirmed in comparative clinical studies, the cadaveric study findings suggest that coracoid transfer itself does not re-establish the natural joint structure and it might be important to strengthen the conjoint tendon and repair Bankart lesions to restore shoulder function and decrease postoperative problems.
Surgical Treatment of Collision Shoulder Injuries Using the Bristow or Latarjet Procedure
Multiple logistic regression analysis indicated that there were no significant differences in the clinical outcomes after coracoid transfer using the Bristow versus Latarjet procedure, even in high-activity collision athletes. These results are consistent with those of recent systematic reviews that reported no significant differences in the clinical outcomes after the Bristow versus Latarjet procedure. 7,10 In addition to finding no differences in the functional scores, we found no difference between the Bristow and Latarjet procedures in the complication rate (6.5% for each procedure). Reinjury occurred in 2 players (1.2%) who underwent the Bristow procedure and in whom the coracoid process broke and the screw bent, while there were no cases of reinjury after the Latarjet procedure. The present reinjury rate is similar to that reported in previous studies. 23,27,31,34 The rate of nonunion of the coracoid was 10.9% after the Bristow procedure and 7.8% after the Latarjet procedure. However, coracoid union was assessed on CT scans at 3 months postoperatively; it would be more accurate to evaluate nonunion on CT scans at 1 year postoperatively. These findings may be explained by the fact that the Latarjet procedure, in which the coracoid process is attached via 2 screws to a prepared area of at least 2 cm in length on the glenoid rim, provides a larger bone-to-bone contact area and more solid fixation than does the Bristow procedure. 22
Limitations
The present study has some limitations. First, all surgical procedures were performed by a single surgeon, who performed the Bristow procedure earlier in his career and subsequently changed to the Latarjet procedure. This may have resulted in a bias due to surgical experience (chronology bias). However, this bias may have been minimal because the surgeon had performed coracoid transfer in >100 shoulders before performing the surgical procedures in the present case series. Second, the follow-up period was insufficient to evaluate postoperative osteoarthritis. Long-term studies of shoulder stabilization outcomes in a cohort of collision athletes are needed in the future. Third, Hill-Sachs lesions were not assessed, although recent studies have indicated that both the glenoid bone defect and Hill-Sachs lesion should be assessed concomitantly in unstable shoulders. 1,9 Thus, repair of Hill-Sachs lesions might effectively restore shoulder function in unstable shoulders with a large glenoid bone defect; this issue requires further investigation. Fourth, our outcomes were based solely on subjective measures, and no objective measurements of range of motion or strength were performed, although both the Rowe score and WOSI that we used included subjective clinical assessments of strength and laxity.
Conclusion
The present results indicate that coracoid transfer (either using the Bristow or Latarjet procedure) with Bankart repair provided good midterm outcomes for competitive rugby players. Preoperative large glenoid bone defects of >20% negatively affected postoperative function of the affected shoulder, whereas the other variables investigated including the type of surgical procedure had no such influence. This information may be important for the strategic treatment of shoulder dislocations in rugby players.
Footnotes
Acknowledgment
Final revision submitted October 15, 2020; accepted November 21, 2020.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board of Juntendo University (No. 16-289).