
Abstract
Background:
The optimal tibial fixation of anterior cruciate ligament (ACL) reconstruction (ACLR) grafts remains controversial.
Purpose/Hypothesis:
The purpose of this study was to compare the biomechanical characteristics of the TensionLoc (TL) cortical fixation device with the Double Spike Plate (DSP) fixation device for ACL tibial fixation using both bone–patellar tendon–bone (BTB) and quadriceps grafts. It was hypothesized that there would be no differences in biomechanical characteristics between the fixation devices regardless of graft type.
Study Design:
Controlled laboratory study.
Methods:
ACLR was performed on 14 matched-pair cadaveric knee specimens—7 pairs using quadriceps grafts (n = 3 male cadaveric knee specimens; n = 4 female cadaveric knee specimens; age, 51 ± 8 years) and 7 pairs using BTB grafts (n = 3 male cadaveric knee specimens; n = 4 female cadaveric knee specimens; age, 50 ± 7 years). One side of each pair was randomized to receive DSP fixation, and the contralateral side received TL fixation. Specimens underwent cyclic ramp loading (10 cycles each at 50-100 N, 50-250 N, and 50-400 N), followed by load-to-failure testing, with the tensile force in line with the tibial tunnel. Results between the 2 fixation types were compared with a paired t test.
Results:
For the quadriceps graft, there were no significant differences in cyclic loading or load-to-failure characteristics between fixation types (P≥ .092 for all parameters). For the BTB graft, TL fixation resulted in higher stiffness than DSP at all cyclic testing cycles except for cycle 1 during 100-N loading and had lower displacement at 250-N loading (3.4 ± 0.1 vs 5.4 ± 0.3 mm; P = .045). For load to failure, TL fixation resulted in higher stiffness than DSP fixation (232 ± 3.1 vs 188.4 ± 6.4 N/mm; P = .046); however, all other load-to-failure parameters were not statistically different (P≥ .135 for all parameters).
Conclusion:
With the quadriceps tendon graft, there were no significant differences in biomechanical characteristics between TL and DSP ACL tibial fixations; however, with BTB grafts, the TL tibial fixation demonstrated greater biomechanical integrity than the DSP tibial fixation.
Clinical Relevance:
The TL fixation device may provide an alternative ACL tibial fixation option for BTB and soft tissue grafts.
Keywords
There are a variety of options for tibial graft fixation in anterior cruciate ligament (ACL) reconstruction (ACLR), including interference screws, suspensory cortical buttons, and extracortical spiked washers and screws. Despite numerous clinical and biomechanical studies on the topic,2,4,5,7 there is no clear consensus as to which method of fixation is most favorable.
Successful ACLR requires stability of the graft within the anatomic tunnel, particularly in the immediate postoperative period.3,6,30 This is especially true in the tibia, which has been described as a comparatively weak link1,14,24 in ACL fixation due to inferior quality of bone at the tibial metaphysis compared with the femur, as well as a line of force on the graft that is directly in line with the tibial tunnel in the weightbearing position of extension, as opposed to an oblique orientation in the femur. 3
Rodeo et al 23 and Shino et al 25 demonstrated that the integration of graft-tunnel fibrous in-growth takes ≥12 weeks and up to 1 year. Current techniques of soft tissue ACLR require some degree of tendon-to-bone healing. With an emphasis on early physical therapy and return to sports, minimizing ACL graft laxity and maintaining sufficient stability is essential in the early postoperative period.
Suspensory fixation devices are commonly used to provide graft fixation on the tibia, particularly when an all-inside technique is utilized, or if the lack of graft length precludes interference screw fixation. These devices provide predictable, rigid graft fixation; however, there remains the potential for construct lengthening and tunnel widening.10,15,20
Tying sutures around a screw post or over a button is commonly used as a stand-alone fixation or as an augmentation for interference screw fixation into a tibial bone tunnel. As the step of tensioning cannot be separated from that of fixation, controlling the tension of the graft can be difficult. To address these problems, a fixation device, the Double Spike Plate (DSP) (Smith & Nephew), is typically used to separate the step of tensioning from that of fixation. 18 A cortical suspensory fixation device that accomplishes separating the step of tensioning from that of fixation is the TensionLoc (TL) (Arthrex). These 2 devices represent an alternative to standard suture buttons.
Since both the DSP and the TL can be used for both bone–patellar tendon–bone (BTB) and soft tissue ACL graft tibial fixation, evaluating the strength of these devices with different graft types is of high importance. The quadriceps tendon has been increasing in popularity as a graft choice for ACLR. Clinical studies have demonstrated comparable clinical results with traditional autografts,11,21,27 with potentially less donor-site morbidity and decreased residual functional deficit.17,22
The purpose of this study was to quantify and compare the biomechanical fixation characteristics of the TL with the DSP for ACL tibial fixation using both the quadriceps tendon and BTB grafts. It was hypothesized that there would be no differences in biomechanical characteristics between TL and DSP tibial fixation types with either the BTB or quadriceps grafts.
Methods
Specimens
A total of 14 matched-pair cadaveric knee specimens were used for the study. Institutional review board approval was not needed, as this was a basic science cadaveric study. Seven matched pairs were allocated to receive a quadriceps graft (n = 3 male cadaveric knees; 4 female cadaveric knees; age, 51 ± 8 years) and 7 matched pairs were allocated for a BTB graft (n = 3 male cadaveric knees; n = 4 female cadaveric knees; age, 50 ± 7 years). Within each matched pair, 1 side was randomly assigned to receive TL fixation, and the contralateral side received DSP fixation.
Quadriceps Soft Tissue Graft Preparation
Specimens were dissected of soft tissue overlying the quadriceps tendon and patella. A 9-mm parallel graft knife blade was used to incise the tendon, starting just proximal to the superior pole of the patella and advancing proximally toward the musculotendinous junction of the rectus femoris. The tendon was incised to a minimum length of 6 cm and a depth of approximately 5 mm. The tendon was subperiosteally dissected off the patella with a No. 10 blade. Proximal dissection continued and the graft was amputated proximally at the musculotendinous junction with a scalpel. The diameter of each graft end was then measured and modified, if needed, to ensure graft passage through a 9-mm tunnel using a graft sizing block. The distal portion of the graft was used for fixation into the tibia for biomechanical testing. A total of 4 No. 2 FiberWire sutures (Arthrex) were sutured into the distal 2 cm of the graft using a Bunnell technique for graft shuttling purposes (Figure 1A). The diameter of each graft end was measured once again, ensuring graft passage through a 9-mm tunnel using a graft sizing block.
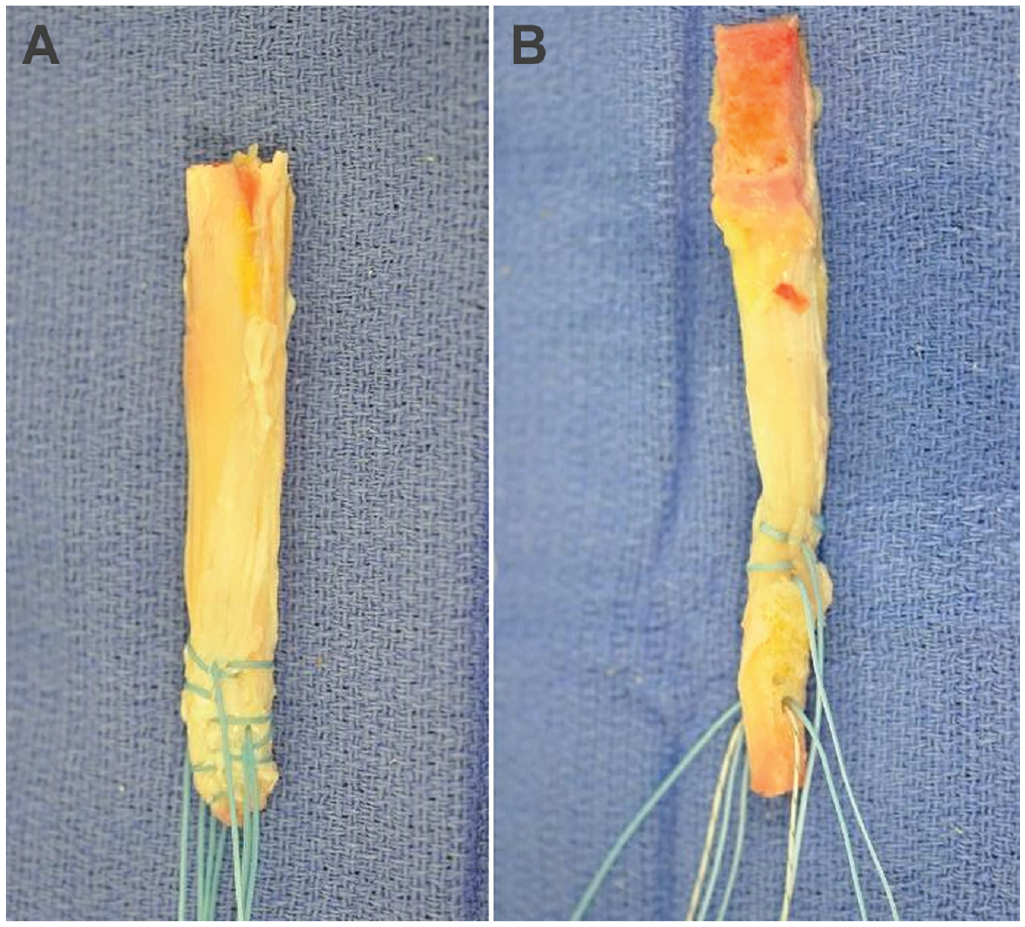
(A) A prepared quadriceps graft. (B) A prepared bone–patellar tendon–bone graft.
BTB Graft Preparation
All overlying soft tissue was cleared from the patella distally to the tibial tubercle. A ruler was used to identify the middle one-third of the patellar tendon for ultimate harvest. A 9-mm parallel graft knife blade was used to incise the tendon longitudinally from proximal to distal. Next, the tibial plug from the tibial tubercle was harvested aiming for a bone plug approximately 9 mm wide and 20 mm long. An oscillating saw was used and inserted to a depth of approximately 8 to 9 mm along each side of the plug to create a trapezoidal-shaped tibial bone plug. A thin osteotome was then used to lift the tibial plug out from the tibia.
A patellar plug approximately 9 mm wide and 20 mm long was then harvested. An oscillating saw was used and inserted to a depth of approximately 8 to 9 mm along each side of the plug to create a trapezoidal-shaped patellar bone plug. A thin osteotome was then used to lift the tibial plug out from the patella. The bone plugs were trimmed to the appropriate size using a rongeur and Metzenbaum scissors. A graft sizing block was used to confirm that the tibial plug would pass through a 9-mm bone tunnel.
A 2-mm drill pin was used to drill a hole 10 mm from the end of the tibial bone block, perpendicular to the cortical bone. Two No. 2 FiberWire sutures were shuttled through the hole to use for graft passage, and 2 additional No. 2 FiberWire sutures were passed in a Bunnell fashion at the bone-tendon junction of the tibial bone plug to aid in graft passage (Figure 1B).
After graft preparation, all graft cross-sectional areas were measured using an area micrometer. The area was measured at the proximal, middle, and distal ends of the graft and averaged. All soft tissues were removed from the specimen and the femur and fibula were dissected free from the tibia.
Specimen Preparation
TL Fixation
The TL is designed for simple, reproducible tensioning and accommodates both the BTB and soft tissue grafts. The outer piece serves as a protective collar and is inserted into the tibial tunnel entrance against the outer tibial cortex, and the inner piece serves as a press-fit plug that secures sutures against the outer collar inner wall. The TL is nonmetallic, accommodates shorter grafts (60-70 mm), and allows for shorter BTB bone plugs. For the TL application, a 2.4-mm guide pin was inserted into the tibia using a standard Arthrex ACL drill guide set to 60°. The pin was directed into the center of the ACL footprint on the tibia. A 10-mm cannulated drill (cigar reamer) was drilled over the pin to a depth of about 5 mm to accommodate the eventual implantation of a 10-mm TL collar. At this point, the aperture was cleared of all soft tissue with a rongeur. Preparation of the entire tibial tunnel was completed by reaming over the guide pin with a 9-mm low profile reamer to allow passage of a 9-mm graft.
The graft was then passed retrograde into the tibia to a depth of 30 mm. The sutures were then threaded through the collar and the collar was inserted into the tibia using the impactor. The plug was then inserted into the impactor, ensuring to orient half of the sutures at the 12 o’clock position and the other half of the sutures at the 6 o’clock position (Figure 2A). The sutures were tensioned and the plug was inserted until the plug was flush with the surrounding collar. The free ends of the suture were tied over the button using an orthopaedic surgeon’s knot to achieve final tibial fixation (Figure 2B).

(A) TL plug insertion. (B) Final TL construct. (C) DSP screw insertion. (D) Final DSP construct. DSP, Double Spike Plate; TL, TensionLoc.
DSP Fixation
A standard ACL drill guide was used to insert a 2.4-mm guide pin from a point approximately 3 cm medial to the medial border of the tibial tubercle to the center of the ACL footprint at an angle of 60° in the sagittal plane. A 9-mm cannulated low-profile reamer was used to overdrill the guide pin and penetrate through the superficial tibial cortex. Using the 3-mm drill, a unicortical hole 2 cm distal to the tibial tunnel was drilled for the eventual cancellous screw.
The graft was then passed retrograde into the tibia to a depth of 30 mm. The sutures were then threaded through each of the 2 holes in the DSP plate (5 sutures through the larger hole and 3 through the smaller hole). The plate was then seated with the screw (Figure 2C). The sutures were manually tensioned, and then the free ends were tied over the plate using an orthopaedic surgeon’s knot to achieve final tibial fixation (Figure 2D).
Biomechanical Setup and Testing
The tibia was potted in a polyvinyl chloride pipe with plaster of paris and placed in an aluminum pot and transfixed with a threaded bolt. The aluminum pot was secured on the Instron machine (Model 3365; Instron) such that the tensile force was in line with the tibial tunnel in the coronal and sagittal planes (Figure 3). The proximal free end of the tendon graft was clamped in a soft tissue, liquid nitrogen, freeze clamp to leave a working length of 30 mm between the articular surface of the tibia plateau and the soft tissue clamp.

Tibia mounted on the baseplate of the Instron testing machine with the graft clamped in the freeze clamp attached to the crosshead.
All fixation methods were tested in cyclic loading and load to failure under tensile force in line with the tibial tunnel. This simulates the worst-case scenario and eliminates the stress shielding that would result from friction between the graft and edge of the intra-articular surface of the tibial tunnel if the tensile force is not parallel to the tibial tunnel. A preload of 50 N was applied, followed by cyclic ramp loading (10 cycles each: 50-100 N, 50-250 N, and 50-400 N) and load-to-failure testing at a rate of 180 mm/min. The method of failure was recorded for each specimen. For cyclic testing, linear stiffness, hysteresis, and deformation were measured for cycles 1 and 10. For load-to-failure testing, a load-deformation graph was used to calculate and determine linear stiffness, yield load, displacement at yield load, ultimate load, displacement at ultimate load, and energy absorbed (Figure 4).

Biomechanical parameters measured for cyclic loading and load to failure.
The paired t test was used for statistical analysis to compare the TS and DSP fixation types of the matched-pair specimens for both the quadriceps graft and BTB graft groups. Significance was set at P < .05.
Results
Quadriceps Graft
The quadriceps graft cross-sectional areas (mean ± SD) were 46.7 ± 4.9 mm2 for the DSP specimens and 48.1 ± 5 mm2 for the TL specimens (P = .536). There were no significant differences in linear stiffness for cyclic loading or load-to-failure stiffness between TL and DSP fixations for the quadriceps graft (P≥ .092 for all comparisons), and there were no significant differences in hysteresis for cyclic loading or energy absorbed to yield load or ultimate load between fixation types (P≥ .144 for all comparisons). The displacement with cyclic loading, as well as the amount of displacement at yield load and ultimate load, was not significantly different between DSP and TL fixation (P≥ .296 for all comparisons) (Table 1), nor were the yield load and ultimate load (P = .538 and P = .344, respectively) (Table 2).
Regarding modes of failure with quadriceps grafts, with TL fixation, the TL broke through the tibia in 4 specimens, 2 specimens failed at the graft-suture interface, and 1 specimen failed because of knot/suture slippage through the TL. With DSP fixation, 4 specimens failed because of suture breakage and 3 specimens failed at the graft-suture interface.
Cyclic Loading Biomechanical Parameters for Quadriceps Graft ACL Tibial Fixation Using Either DSP or TL a

Data are presented as mean (SEM). ACL, anterior cruciate ligament; DSP, Double Spike Plate; NA, not applicable; TL, TensionLoc.
Load-to-Failure Biomechanical Parameters for Quadriceps Graft ACL Tibial Fixation Using Either DSP or TL a

Data are presented as mean (SEM). ACL, anterior cruciate ligament; DSP, Double Spike Plate; TL, TensionLoc.
BTB Graft
The BTB graft cross-sectional areas (mean ± SD) were 41.8 ± 7.5 mm2 for the DSP specimens and 43.6 ± 7.3 mm2 for the TL specimens (P = .137). ACL tibial fixation with TL fixation resulted in significantly higher stiffness compared with DSP fixation for cycle 10 during 100-N loading, cycles 1 and 10 during 250-N loading, cycle 1 during 400-N loading, and linear stiffness to failure (P≤ .046 for all comparisons) (Tables 3 and 4). BTB tibial fixation with DSP fixation had significantly higher hysteresis for cycle 1 during loading to 250 N compared with TL fixation (P = .049). There were no statistically significant differences regarding hysteresis at other cyclic loading conditions or at energy to yield load and ultimate load (P≥ .112 for all comparisons). Displacement at cycle 10 during cyclic loading to 250 N was significantly lower with TL fixation (P = .045). There were no significant differences in displacement between fixation types regarding other cyclic loadings or at load to failure (P≥ .058 for all comparisons). There were also no significant differences in yield load or ultimate load (P = .135 and P = .727, respectively).
Cyclic Loading Biomechanical Parameters for BTB Graft ACL Tibial Fixation Using Either DSP or TL a

Data are presented as mean (SEM). Bold P values indicate statistically significant differences between fixation types (P < .05). ACL, anterior cruciate ligament; BTB, bone–patellar tendon–bone; DSP, Double Spike Plate; NA, not applicable; TL, TensionLoc.
Load-to-Failure Biomechanical Parameters for BTB Graft ACL Tibial Fixation Using Either DSP or TL a

Data are presented as mean (SEM). The bold P value indicates a statistically significant difference between fixation types (P < .05). ACL, anterior cruciate ligament; BTB, bone–patellar tendon–bone; DSP, Double Spike Plate; TL, TensionLoc.
Modes of failure with the BTB graft were as follows: with TL fixation, the TL broke through the tibia in 3 specimens, the suture pulled through the BTB graft bone block in 3 specimens, and 1 specimen failed because of suture breakage at the TL; with DSP fixation, the suture pulled through the BTB graft bone block in 3 specimens, 3 specimens failed because of suture breakage, and 1 specimen failed because of the screw breaking through tibial bone.
Discussion
In this biomechanical study, both TL and DSP fixations showed graft type–dependent behavior for ACL tibial fixation. With the quadriceps tendon soft tissue graft, similar biomechanical characteristics were observed for all biomechanical parameters when comparing the TL and the DSP for ACL tibial fixation. With the BTB grafts, the TL fixation device demonstrated greater cyclic loading stiffness and ultimate load to failure. However, yield load, and energy absorbed between the TL and the DSP ACL tibial fixation did not demonstrate statistically significant differences. These findings suggest that the TL for ACL tibial fixation compares favorably with the DSP, a device that has been biomechanically regarded as reliable.13,18,26
The graft type–dependent behavior for ACL tibial fixation can be attributable to the differences in fixation types between the soft tissue quadriceps tendon graft construct and the BTB graft construct. For quadriceps tendon ACL tibial fixation, there were no differences in structural integrity between the TL and the DSP. For BTB graft ACL tibial fixation, the stiffness and the ultimate load were higher for the TL compared with DSP ACL tibial fixation.
A potential explanation for the observed similarities in nondestructive biomechanical characteristics (hysteresis, stiffness, and yield) between TL and DSP fixations for quadriceps tendon soft tissue graft constructs can be attributed to the same suture and soft tissue graft interface, which is thought to be the least rigid link in the suspensory fixation construct. Furthermore, the similarity in the load-to-failure characteristics may be due to multiple failure modes being observed with both the TL and the DSP ACL tibial fixation. The failure modes for the quadriceps TL fixation included the TL implant breaking through the tibia in 4 specimens, 2 specimens failing at the graft-suture interface, and 1 specimen failing because of knot/suture slippage through the TL. For the quadriceps DSP fixation, 4 specimens failed because of suture breakage and 3 specimens failed at the graft-suture interface. For BTB graft ACL fixation, a potential explanation for the observed differences in stiffness and ultimate load to failure between TL and DSP fixations may be attributable to the working length of the graft construct. The TL fixation point is at the tibial tunnel, while the DSP has a fixation point distal to the tibial tunnel and therefore has a comparably longer working length of the graft construct. While previous studies demonstrated that shorter graft length results in stiffer constructs during range of motion,9,12 a more recent biomechanical study 16 suggested that both the inherent stiffness of the fixation method and the bone quality may equally play a role in the overall stability of a graft and its ability to restore stability to the knee.
Suspensory cortical fixation has several advantages: fixation is applied to relatively stronger cortical bone, there is the ability to re-tension with several devices, and as opposed to an interference screw, the larger area of the graft to the cancellous bone within the tibial tunnel promotes circumferential tunnel graft healing. On the other hand, cortical button loop devices may lengthen, and overall fixation relies heavily on the suture-graft interface. Spiked washers and screws also have the benefit of fixation into the strong cortical bone and have reasonably high loads to failure. Compared with cortical buttons, there are limited clinical studies, and because of soft tissue irritation, they may require hardware removal postoperatively.
Numerous biomechanical studies have evaluated the fixation strength of extracortical suspensory fixation devices in the tibia, with varying results. Magen et al 19 and Kousa et al 14 evaluated a variety of hamstring tendon graft tibial fixation devices in the human and porcine tibia, respectively. Tandem washers (Linvatec) and WasherLoc (Arthrotek) were shown to provide higher yield load values and significantly less displacement compared with interference screws. More recently, Fogel et al 8 concluded that interference screw fixation of hamstring grafts demonstrated superior biomechanical properties for cyclic testing compared with a cortical suspension button. Smith and DeBerardino 28 evaluated the tibial fixation properties of both a suspensory adjustable loop button and an interference screw using hamstring grafts in the porcine tibia. The continuous loop construct had a significantly higher load to failure compared with the use of an interference screw, and cyclic loading was comparable.
Limitations
The first limitation of this study was that the mean age of the cadaveric specimens was approximately 50 years, and the bone quality was occasionally poor, which is not atypical for cadaveric studies. The second limitation is that cyclic and load-to-failure testing was performed on the tibia, with the direction of the force aligned along the long axis of the graft. 29 The vector of force-loading of the graft likely concentrated the majority of stress at the fixation site, resulting in early catastrophic failure—a scenario not likely experienced during in vivo situations. A third limitation is that this was a time-zero biomechanical comparison of fixation strength and thus did not consider graft healing. Finally, the TL was compared with a similar suspensory fixation device and further testing should be performed to compare TL fixation with other fixation mechanisms.
Conclusion
With the quadriceps tendon graft, there were no significant differences in biomechanical characteristics between TL and DSP ACL tibial fixations; however, with BTB grafts, the TL tibial fixation demonstrated greater biomechanical integrity than the DSP tibial fixation.
Footnotes
Final revision submitted February 8, 2023; accepted February 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was provided by a research grant from Arthrex to Congress Medical Foundation. Arthrex also donated the medical devices used in this study. The funding source did not play a role in this investigation. M.J. has received education payments from Arthrex. P.S.B. has received education payments from Micromed, consulting fees from Arthrex, and royalties from Arthrex and Zimmer Biomet. G.J.A. has received hospitality payments from Arthrex. T.Q.L. has received consulting fees from Arthrex and royalties from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.