
Abstract
Background:
The optimal graft choice and fixation technique remain a topic of ongoing debate in both primary and revision anterior cruciate ligament (ACL) reconstruction (ACLR). Cortical tibial press-fit fixation offers known advantages such as eliminating the need for hardware, thereby reducing cost and avoiding complications related to implants, while also potentially minimizing bone tunnel enlargement.
Purpose:
To investigate the time-zero biomechanical properties (cyclic displacement, stiffness, and load to failure) of cortical tibial press-fit technique using bone–patellar tendon (BPT) graft for ACLR and compare with metal interference screw fixation to determine the potential clinical benefit of this technique.
Study Design:
Controlled laboratory study.
Methods:
A total of 24 skeletally mature porcine knees were used. After determining the bone mineral density (BMD) of each specimen, the specimens were randomly assigned to their respective groups. One group underwent interference screw (9 mm–diameter × 25 mm–length) fixation using a BPT autograft, while the other group underwent implant-free cortical tibial press-fit fixation. Biomechanical testing included 3 loading phases: (1) preconditioning (10-50 N for 10 cycles); (2) submaximal cyclic loading (50-200 N for 1500 cycles); and (3) load to failure testing at a 20 mm/min loading rate. Groups were compared for stiffness, cyclic displacement and ultimate load to failure using Mann-Whitney U tests and for failure mode using a Fisher exact test.
Results:
Both groups of specimens showed similar BMD characteristics (P = .59). There was no significant difference in cyclic displacement (interference screw group, 5.73 ± 1.71 mm; press-fit group, 5.03 ± 1.70 mm; P = .38), or total displacement (interference screw group, 11.02 ± 3.37 mm; press-fit group, 10.33 ± 3.70 mm; P = .76). The mean cyclic displacement of the bone plugs was not significantly different between groups (interference screw group, 0.06 ± 0.05 mm; press-fit group, 0.03 ± 0.05 mm; P = .19). Stiffness at the last submaximal loading cycle was comparable between the groups (interference screw group, 65.32 ± 11.16 N/mm; press-fit group, 70.27 ± 13.39 N/mm; P = .76). Mean ultimate load at failure was 586.4 ± 75.9 N (range, 467.9-745.9 N) for the interference screw fixation group and 639.0 ± 149.2 N (range, 485.1-1050.5 N) for the press-fit group and (P = .51). All specimens failed due to tendon avulsion at the tendon-bone junction or tendon rupture at the midsubstance.
Conclusion:
In this porcine patellar tendon ACLR tibial fixation model, cortical tibial press-fit fixation provided adequate primary stability, demonstrating similar cyclic displacement, construct stiffness, and ultimate load characteristics compared with interference screw fixation.
Clinical Relevance:
Cortical tibial press-fit technique may represent an effective method for ACLR.
Keywords
Despite advancements in surgical techniques and evidence-based rehabilitation protocols, high reinjury rates remain a concern after anterior cruciate ligament (ACL) reconstruction (ACLR). 9 A graft failure rate of 6.2% and an overall failure rate of 11.9% at 10 years have been reported, leading to an increase in the frequency of revision ACL surgeries. 8 A recent systematic review evaluating the outcomes of revision ACLR reported that 39.2% of patients required a 2-stage revision. 7 Tunnel malpositioning and widening were identified as the most common reasons for the need for a 2-stage revision. 12
Bone tunnel widening is considered a significant concern after ACLR, with reported degrees of enlargement ranging from 23% to 121%, regardless of graft types and fixation methods used.14,16,31 Several factors have been suggested as causes of tunnel widening, including graft fixation, graft motion, the influx of synovial fluid into the tunnel, poor bone quality, and the degradation of resorbable implants. 24 While the clinical effect of tunnel widening remains unclear, it is well-established that large tunnels significantly complicate revision ACL surgery, especially in the tibial tunnel.6,23 Although many attempts have been made to reduce tunnel enlargement, no universally accepted solution has been established to date. 21
To address these issues, the press-fit fixation technique has been described and utilized over the past 20 years.2,32 Originally developed for femoral-sided press-fit fixation of the bone–patellar tendon–bone graft, this technique was expanded to include tibial-sided press-fit fixation, and several modifications have been described since then.4,13,15,30 Implant-free press-fit techniques promote undisturbed bone-to-bone healing and eliminate issues associated with hardware fixation, including graft laceration, biocompatibility concerns, and local reactions leading to tunnel widening. 10 Biomechanical strength testing of press-fit techniques has been conducted by several researchers, yielding varying results. In their biomechanical studies, Boszotta and Anderl 5 showed that tibial press-fit fixation provided high primary stability, while Seil et al 29 found that press-fit fixation did not ensure secure fixation. On the other hand, while press-fit fixation using autologous bone in the tibial canal has been shown to result in less bone tunnel enlargement, inadequate fixation and potential graft failure remain a concern, particularly in cases involving osteoporotic bones and revision ACL procedures complicated by tunnel enlargement.2,5,29
Recently, Kocabey et al18-20 described cortical tibial press-fit technique using periosteum–patellar tendon–bone autograft for ACLR (Figure 1). They proposed that utilizing a trapezoidal tibial bone autograft would completely fill the tibial tunnel, offer absolute stability through cortical press-fit fixation, and be utilized as a single-stage procedure during revision ACL surgery, even in the presence of significant tunnel widening. 18 The current study was conducted to determine whether cortical tibial press-fit fixation achieves time-zero stability of the graft construct. The objective of this biomechanical study on porcine bone was to evaluate the initial fixation strength and the failure modes of a bone–patellar tendon (BPT) autograft with cortical tibial press-fit fixation technique compared with a titanium interference screw. Our hypothesis was that the cortical tibial press-fit fixation would demonstrate comparable biomechanical characteristics to interference screw fixation.

Schematic representation of the cortical tibial press-fit technique.
Methods
Specimen Preparation
A total of 24 adult porcine knees were used in this study. A porcine model was selected for this study because of previously reported similarities in morphology to adult humans. 1 The specimens were received precut and with soft tissue. The tibial bone mineral density (BMD) for each specimen was determined with a dual-energy x-ray absorptiometry scanner. The samples were stored at −22°C before thawing for ACLR and biomechanical testing. The porcine samples were divided into 2 groups; (1) interference screw fixation, (2) implant-free cortical tibial press-fit fixation which consisted of 12 porcine knees in each group.
BPT With Interference Screw Group Preparation
After identification of the 10-mm central patellar tendon, a surgical pen and ruler were used to mark the incision line. A No. 9 scalpel was then used to free the central patellar tendon autograft. Using an oscillating bone saw with a 1.2 mm–thick blade, osteotome, and mallet, a 9 mm–wide × 30 mm–long proximal bone component was removed from the tibial tubercle. Because the study focused solely on the biomechanical performance of tibial fixation, the patellar bone was removed. After this, a 10 mm–diameter drill was used to create a 30 mm–deep tibial tunnel at a 45° angle. Next, the BPT autograft was inserted into the tibial tunnel and the bone plug was fixed with a 9 mm–diameter × 25 mm–long titanium interference screw (Doratek Medical Inc), leaving 5 mm of the bone plug outside the tunnel for the determination of the bone plug displacement. The proximal BPT autograft was looped around a 5.5 mm–diameter stainless steel pin and stitched onto itself using No. 2 FiberWire (Arthrex) with a whipstitch technique for biomechanical testing.
Implant-Free BPT Cortical Tibial Press-Fit Group Preparation
A 10 mm–wide section of the central patellar tendon was marked from the inferior aspect of the patella to the tibial tubercle, similar to the control group samples. The tibial tubercle was outlined in a trapezoidal shape measuring approximately 35 mm in length, with a narrow superior base of 10 mm and a wider inferior base of 12 mm. An oscillating bone saw with a 1.2 mm–thick blade was used to cut the tibial tubercle. After careful extraction with a mallet and osteotome, the construct was pulled upward. A scalpel was then used to detach the patellar tendon from the patellar bone. Subsequently, a 30 mm–long tibial tunnel was drilled at a 45° angle using a 10 mm–diameter reamer. Then, the distal 10 mm of the tunnel was further reamed to 11 mm in diameter to allow press-fit engagement. The graft was then passed through the tibial tunnel, and a mallet was employed to tap the bone plug into place, leaving the last 5 mm of the bone plug outside the tunnel for accurate measurement of the bone plug displacement. After the successful passage of the BPT graft through the tibial tunnel, the proximal BPT graft was also looped around a 5.5 mm–diameter stainless steel pin and stitched onto itself using No. 2 FiberWire with a whipstitch technique for biomechanical testing.
All biomechanical tests were performed at room temperature (approximately 22°C). To maintain tissue hydration throughout the testing protocol, specimens were kept moist with gauze soaked in 0.9% NaCl solution, which was rehydrated as necessary during the testing process.
Fixation of the Specimen in the Testing Machine
For biomechanical testing, each tibia was cemented into a custom-made fixation device. The base of each potted specimen was secured in the electromechanical actuator (5-kN AG-X; Shimadzu) using T-type mold clamps. To simulate a "worst-case" tensile-loading scenario, the tibiae were positioned so that the 45° tibial tunnels were precisely aligned with the direction of the applied loading force. During specimen preparation, each sample was kept moist with gauze soaked in 0.9% NaCl physiological saline solution before biomechanical testing.
Testing Protocol
The biomechanical testing protocol consisted of 3 loading phases: (1) preconditioning, involving 10 cycles at forces ranging from 10 to 50 N at 1 Hz; (2) submaximal cyclic loading, where specimens underwent 1500 cycles at 50 to 200 N at 1 Hz; and (3) ultimate load-to-failure testing, conducted at a loading rate of 20 mm/min (Figure 2). Key metrics, including ultimate load-to-failure (N), stiffness at the submaximal loading cycles (N/mm), displacement (mm), and cyclic displacement (mm), were calculated from the raw data. Overall displacement was measured from the 2nd cycle to the point of failure for each specimen, while cyclic displacement reflected the changes in displacement between the 2nd and the 50th, 100th, 200th, 500th, and 1500th cycles, using the peak load in each cycle as the reference point. The intermediate points were used for curve validation and internal consistency control, but only the 2nd to 1500th interval was used for quantitative comparison. Bone plug displacement was determined using a high-resolution camera (EOS 750D; Canon) placed 1 m from the testing apparatus, in combination with AutoCAD 2020 software (Autodesk). This was defined as the vertical distance between the lower end of the bone plug outside the distal tibial tunnel and the upper edge of the distal tibial tunnel at both the start and the end of the cyclic loading phase (Figure 3). In addition to these quantitative measures, specimens were assessed for failure modes and the specific phase during which failure occurred. The load (N) and displacement (mm) values obtained during the tests were simultaneously recorded by the tester's own software (Trapezium X; Shimadzu).
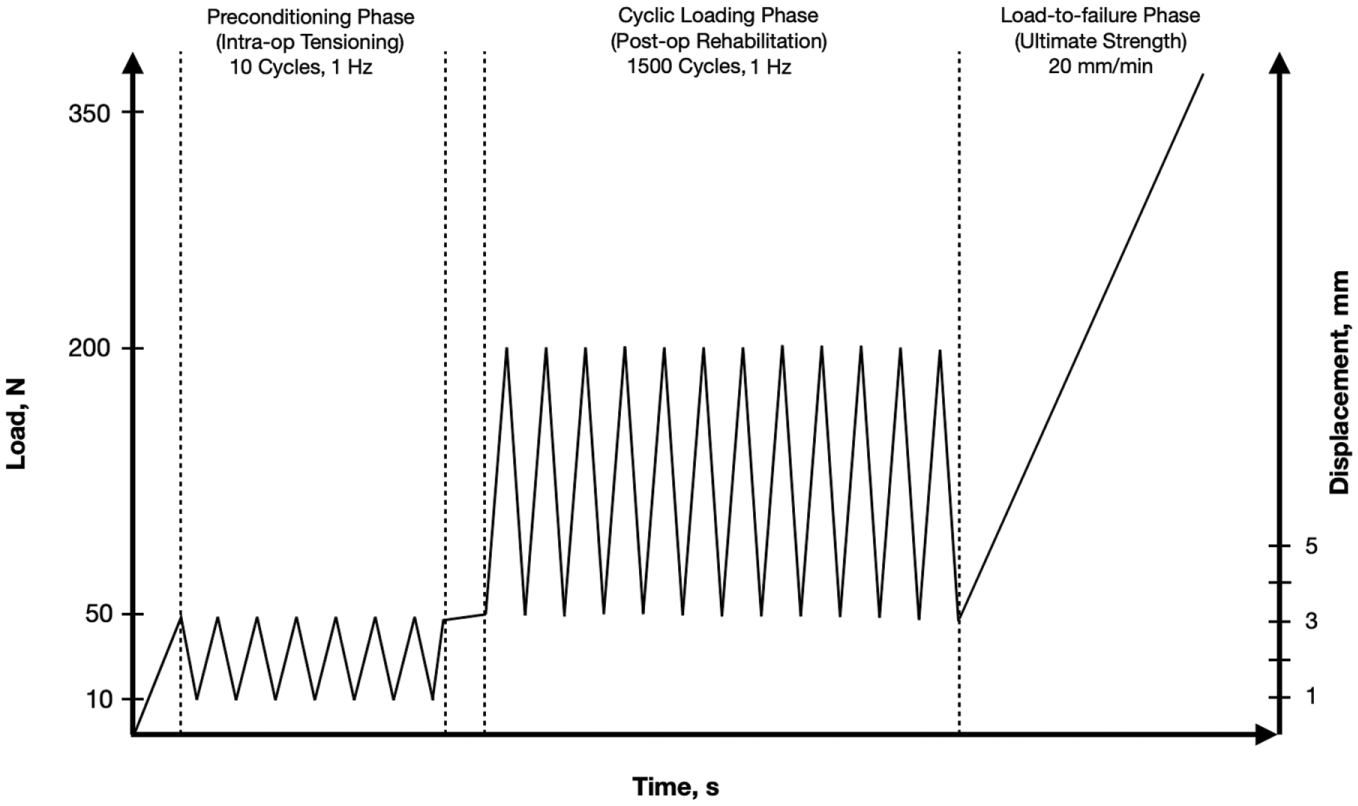
Biomechanical test loading phase configurations.
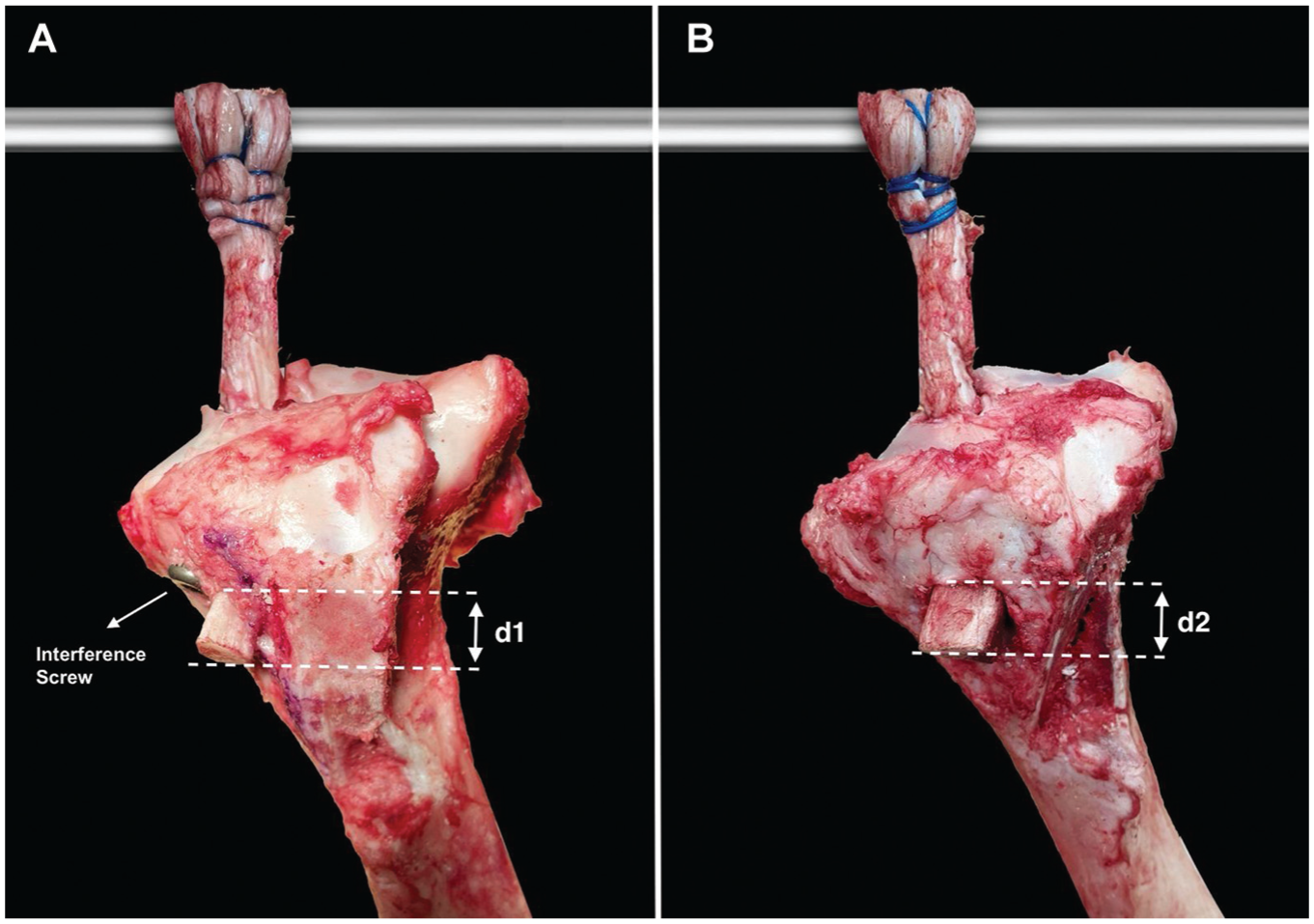
Final experimental setup and reference points for the measurement of the bone plug displacement: (A) interference screw group, (B) cortical tibial press-fit group. d1 and d2 indicate the distance between the most inferior aspect of the bone block and the aperture of the tibial tunnel.
Statistical Analysis
Quantitative and qualitative biomechanical test results were recorded. To assess the normality of outcome variables, the Shapiro-Wilk test was used. Group comparisons were conducted using a 2-tailed Student t test. A pilot study (n = 3) of both the interference screw and press-fit groups, focusing on cyclic displacement and load-at-failure metrics, indicated that a sample size of 12 specimens per group would achieve a statistical power of 0.8. Statistical analyses were performed using SPSS software (IBM SPSS Statistics), with a significance level set at P < .05.
Results
Both groups of specimens showed similar BMD characteristics (interference screw group, 0.704 ± 0.15; press-fit group, 0.663 ± 0.11; P = .59). All the specimens completed each loading phase. Quantitative biomechanical test results are displayed in Tables 1 and 2. Cyclic and total displacements of the construct were measured in the 2 experimental groups. There was no significant difference in cyclic displacement between the groups (interference screw group, 5.73 ± 1.71 mm; press-fit group, 5.03 ± 1.70 mm; P = .38). The displacement at failure—representing the total elongation of the graft construct from the second cycle to failure—was also comparable between groups (interference screw group, 11.02 ± 3.37 mm; press-fit group, 10.33 ± 3.70 mm; P = .76). Bone plug displacement was measured separately using high-resolution imaging and showed no significant difference between groups. (interference screw group, 0.06 ± 0.05 mm; press-fit group, 0.03 ± 0.05 mm; P = .19). Stiffness at the last submaximal loading cycle was comparable between the groups (interference screw group, 65.32 ± 11.16 N/mm; press-fit group, 70.27 ± 13.39 N/mm; P = .76). Mean ultimate load at failure was 586.4 ± 75.9 N (range, 467.9-745.9 N) for the interference screw fixation group and 639.0 ± 149.2 N (range, 485.1-1050.5 N) for the press-fit group (P = .51). None of the bone plugs in either group exhibited any signs of pullout. All specimens failed due to tendon avulsion at the tendon-bone junction or tendon rupture at the midsubstance.
Displacement and Failure Data for Interference Screw Group a

BMD, bone mineral density.
Displacement and Failure Data for Cortical Tibial Press-Fit Group a

BMD, bone mineral density.
Discussion
The main finding of the current study is that implant-free cortical tibial press-fit fixation provides adequate primary stability, demonstrating similar cyclic displacement, construct stiffness, and ultimate load characteristics compared with interference screw fixation. These results suggest that the cortical tibial press-fit technique represents an effective method for ACLR.
There is a tendency toward the accelerated rehabilitation after ACLR to return to normal life activities as quickly as possible. 17 Cyclic displacement of time-zero biomechanics reflects the graft's ability to withstand early functional postoperative rehabilitation regimens, which increase the load on the graft fixation construct before biological integration in the tunnels occurs. In their study, Seil et al 29 compared the initial strength between interference screw and press-fit fixation in a porcine model and reported that half of the graft fixations failed under cyclic loads in the press-fit group. They suggested that press-fit fixation is not secure enough for accelerated rehabilitation. Similarly, Musahl et al 25 reported that 4 out of 10 specimens failed during the cyclic creep test in the press-fit group using a goat model. In contrast to other findings, the current study demonstrated that none of the specimens in any group exhibited slippage during the cyclic loading test, suggesting that there was no significant fixation failure. This difference may be explained by the cortical nature of the press-fit fixation used in the current study, compared with previously reported press-fit techniques.
Another crucial aspect, particularly in regard to loading allowances during rehabilitation, is the ultimate failure load. Although the native ACL's ultimate failure load is 2160 ± 157 N, previous studies have shown that in situ forces on the ACL can reach up to 445 N during daily activities, leading to the hypothesis that grafts used in ACLR must have failure loads of ≥445 N. 11 Previously reported studies on press-fit techniques have yielded a variety of results. Musahl et al 25 reported that the mean maximal load to failure for the press-fit fixations was 215 ± 75 N, which was significantly lower than that of the interference screw fixation group. On the other hand, Lee et al 22 sought to enhance the fixation strength of the press-fit technique by harvesting the bone plug into a fully circular shape and increasing the diameter difference between the bone plug and the femoral tunnel. In their porcine model, they observed a mean failure load of 605 N for the femoral press-fit fixation and suggested that the press-fit group demonstrated sufficient fixation strength for rehabilitation, comparable with that of the interference screw group. 22 Similarly, our results showed that cortical press-fit fixation in the tibial tunnel had a similar ultimate failure load compared with the interference screw group.
The importance of fixation strength has been emphasized in multiple studies, with the tibial side identified as the weakest point of the construct due to the weaker bone in the tibial metaphysis compared with the femur, and the tibial tunnel's orientation being more parallel to the physiologic traction on the graft. 27 For these reasons, hybrid fixation of the tibial-sided graft in ACLR is recommended. 3 Studies have also reported that hybrid methods of tibial-sided graft fixation in ACLR result in stronger initial fixation and reduced side-to-side laxity. 3 On the other hand, biomechanical studies have shown that previously reported press-fit techniques that used cancellous fixation primarily failed at the tibial insertion.5,25,29 In contrast, our results showed that cortical press-fit fixation in the tibial tunnel is at least equal to interference screw fixation. The most reasonable explanation is that cortical-based fixation has higher stiffness compared with cancellous fixation.
Although the clinical effect of tunnel widening is not fully elucidated, it is widely recognized that large tunnels can significantly complicate revision ACL surgeries, particularly in the tibial region. 23 Studies have shown that regardless of whether soft tissue or bone-patellar tendon-bone grafts are used, significantly greater tunnel enlargement occurs on the tibial side compared with the femoral side.26,33 Weber et al 33 also investigated tunnel enlargement based on location, finding significant enlargement at both tunnel apertures and the tibial tunnel midsection, while the tunnel exit sites consistently showed a decrease in cross-sectional area over the time. Previously reported press-fit techniques have identified unstable tibial fixation as a potential perioperative complication in revision ACL surgery, and it has also been demonstrated that the primary stability of BPT grafts in press-fit ACLR is primarily influenced by bone plug length. 28 This suggests that cortical press-fit tibial fixation technique using long-bone plug can be effectively used in a single-stage procedure during revision ACL surgery, even in cases of significant tunnel widening.
Implant-free press-fit fixation techniques offer several appreciated advantages, including promoting undisturbed bone-to-bone healing through a biological approach, avoiding complications related to hardware fixation (such as graft laceration, biocompatibility concerns, and local reactions that may result in tunnel enlargement), and being cost-effective.10,30 On the other hand, inadequate fixation, particularly in revision cases, continues to be a significant concern. In addition to these, cortical press-fit fixation in the tibial tunnel, which is evaluated in the current study, has 2 theoretical advantages. 18 The first advantage is that it utilizes cortical-based fixation, which offers higher stiffness compared with cancellous press-fit fixation. The second advantage is that the long-bone block completely fills the tibial tunnel, which minimizes the risk of tunnel enlargement. Tunnel widening is affected not only by the hardware but also by the tendon graft within the tibial tunnel. 31 Further clinical studies to validate these advantages could be of interest and represent a logical next step in this area of research.
Limitations
There are limitations to the current study that should be acknowledged. First, because a porcine knee model was chosen, the transferability of these results to human ACLR in vivo may be limited. However, porcine knees have been validated as a comparative model for young adult human knees. 1 The mean BMD of our specimens (approximately 0.66-0.70 g/cm2) was somewhat lower than that reported for the proximal tibia of human adolescents and young adults (typically ranging from 0.9 to 1.2 g/cm2). This difference may limit the direct extrapolation of our results to human clinical scenarios. However, the fact that both fixation methods demonstrated sufficient mechanical strength in this context suggests that cortical press-fit fixation may still be a viable technique, particularly when bone quality is suboptimal, such as in revision surgery or in patients with reduced bone density. Second, this study used a porcine model to evaluate time-zero properties; therefore, it does not account for the in vivo conditions of the graft during the healing phases of ACLR. Third, the loads were applied longitudinally to the graft to simulate a worst-case scenario for ACL graft failure. However, this does not reflect the typical in vivo loading conditions that would be assessed in a kinematic study evaluating knee motion. Fourth, the current study could not evaluate the pull-out strength of the bone plugs because all specimens experienced tendon rupture. The suture-tendon interface appeared to be the likely point of structural weakness, as the suturing process led to graft weakening. Fifth, the results for this technique are expected to be even better, as would be desirable, if bone plug slippage and graft elongation could be measured separately, as the testing machine provided combined results for bone plug slippage and graft elongation. However, a high-resolution camera was used to measure the relative movement between the tibia and the bone plug. There was no significant difference between groups in terms of the mean cyclic displacement of the bone plugs. Furthermore, all samples exceeded the minimum required force threshold of 445 N. 11 Future clinical studies should assess the effectiveness of cortical press-fit fixation in the tibial tunnel during the healing phase of ACLR.
Conclusion
In this porcine patellar tendon ACLR tibial fixation model, cortical tibial press-fit fixation provided adequate primary stability, demonstrating similar cyclic displacement, construct stiffness, and ultimate load characteristics compared with interference screw fixation.
Footnotes
Final revision submitted May 12, 2025; accepted July 8, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.