
Abstract
Background:
Arthroscopic repair of longitudinal tears in the medial meniscal posterior horn (MMPH) has been reported to result in high rates of meniscal healing when performed alongside anterior cruciate ligament reconstruction (ACLR). However, studies that have focused on longitudinal tears and their impact on clinical outcomes after arthroscopic repair are insufficient.
Purpose:
To investigate the clinical outcome and healing status after concomitant arthroscopic ACLR and repair of MMPH peripheral longitudinal tears, with respect to the tear length.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 263 patients who underwent concurrent arthroscopic suture repair of longitudinal tears of the MMPH and ACLR were enrolled. All patients had 2-year postoperative magnetic resonance imaging (MRI) evaluations, and 61% of patients underwent a second-look arthroscopy. The exclusion criteria were partial meniscectomies and multiligament injuries. Patients were assessed pre- and postoperatively for clinical scores, amount of anterior translation, grade of pivot shift, and presence of meniscal tear extension. According to the length of longitudinal tears, patients were classified into 2 groups: (1) patients with tears that were located in the posterior compartment and (2) patients with tears that extended to the midbody of the meniscus. Binary stepwise logistic regression analysis was used to evaluate the risk factors for unhealed menisci as identified by MRI.
Results:
A total of 83 patients were included in this study—52 patients (group 1) had MMPH tears without tear extension and 31 patients (group 2) had MMPH tears with tear extension. There were no differences in outcomes between the groups, including the healing rate after meniscal repair (P > .05). Based on postoperative MRI scans, 67 patients (80.7%) were categorized as completely healed and 16 patients (19.3%) as unhealed. There were no significant differences between the completely healed and unhealed groups in outcomes or the rate of preoperative midbody tear extension. Higher body mass index and lower preoperative Lysholm scores were identified as risk factors for unhealed menisci.
Conclusion:
Overall, the rate of complete healing of MMPH tears repaired concomitantly with ACLR was 80.7% (67/83), and midbody tear extension did not affect the healing rate of the repaired meniscus. Results indicate that suture repair for unstable MMPH tears should be considered regardless of tear size.
Keywords
Peripheral longitudinal tears of the medial meniscal posterior horn (MMPH) are reported as the common meniscal lesions associated with anterior cruciate ligament (ACL) injuries. 22,24,42,43 The occurrence of MMPH peripheral longitudinal tears in ACL-deficient knees affects anterior and rotational laxity of the knee joint. 10,12,47 Thus, intraoperative diagnosis and appropriate treatment of MMPH peripheral longitudinal tears are important to restore knee biomechanics and improve the clinical outcomes of ACL surgery. 10,12,24,26,47,54 Furthermore, an increased healing rate of meniscal lesions has been reported when concomitant meniscal repair and ACL reconstruction (ACLR) are performed. Preoperative suspicion and aggressive treatment are important for an increased healing rate of meniscal lesions. 13,29,50
It has previously been reported that the healing potential of meniscal lesions with ACLR was higher than that without ACLR 18,30 ; however, there is currently no consensus on the appropriate treatment of MMPH peripheral longitudinal tears. 1,34,39 Several studies have reported similar outcomes with stable lesions left in situ without repair at the time of ACLR 28,38,39 ; however, other reports have shown a higher healing rate with the repair of MMPH peripheral longitudinal tears and the advantages of repair for the clinical outcomes. 1,2,34,49 The failure rates of meniscal healing were reported as 12.1% to 16.3% when only abrasion and trephination were performed 1,38 but as 2.3% to 11.7% when the all-inside repair using a suture hook was performed. 1,2 There might be differences in the healing rate according to the tear length or extension, location, type of tear, repair techniques, and follow-up periods. 1,16,19,33,34,38,49 However, there are still insufficient studies regarding the healing potential of MMPH peripheral longitudinal tears after repair with ACLR, with consideration to the degree of extension to the midbody of the meniscus.
The purpose of this study was to investigate the outcomes of patients who underwent concomitant ACLR and repair of MMPH peripheral longitudinal tears with consideration to the tear extension. We hypothesized that patients with tear extension to the midbody of an MMPH tear would have lower healing rates and clinical outcomes than patients without tear extension.
Methods
The study was approved by the institutional review board and performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. As this was a retrospective study the need for patient informed consent was waived. This was a retrospective cohort study of 263 patients who underwent primary single bundle ACLR between 2012 and 2019 by a single senior surgeon using hamstring autografts or hybrid grafts with tibialis allografts according to the size of the hamstring autograft, using a hybrid graft in case of an autograft with <8 mm diameter. Confirmative diagnosis of MMPH peripheral longitudinal tears was determined by a peripheral longitudinal tear within 5 mm of the meniscocapsular junction during arthroscopic ACLR. 24,26
The study inclusion criteria were MMPH tears with arthroscopic suture repair with a minimum 2-year follow-up after surgery, including magnetic resonance imaging (MRI) evaluations or second-look arthroscopy. The exclusion criteria were as follows: (1) fractures that needed open reduction and internal fixation (n = 11 cases); (2) previous history of surgery on the knee (n = 11 cases); (3) other combined surgical procedures such as osteotomy and ACL revision (n = 30 cases); (4) multiligament injuries (n = 36 cases); (5) partial ACL rupture (n = 14 cases); (6) partial meniscectomy cases, such as a central-third tear of the medial meniscus (MM) (white-white zone), bucket-handle tears, or stable lesions, defined as those <1.5 cm in length with no excessive anterior translation 4,28 by probing (n = 29 cases); and (7) incomplete clinical data, such as grade of laxity or preoperative MRI (n = 49 cases). After applying these criteria, 83 patients (n = 73 men; n = 10 women) remained and were enrolled in this study. The groups were categorized according to the tear extension of MMPH tears found during arthroscopy—tears that were located only at the MMPH (group 1) and tears that extended to the midbody of the MM as well as MMPH tears component (group 2) (Figures 1 and 2).

Arthroscopic image of a tear only at the medial meniscal posterior horn.

Arthroscopic images showing (A) a medial meniscal posterior horn tear and (B) an extended tear to the midbody of the medial meniscus.
Arthroscopic Procedure and Rehabilitation
All arthroscopic procedures were performed by a single senior author (S.H.L.). 24 Systematic arthroscopic evaluations were performed using 30° and 70° arthroscopes during ACLR. To visualize the posteromedial compartment of the knee, a 30° arthroscope was advanced through the intercondylar notch space after a routine examination from the anterolateral and anteromedial portals. Then, a 70° arthroscope was changed in situ for full visualization of MMPH, including the posteromedial corner. 24 The location of the meniscal tear was represented by 3 different zones—anterior horn; midbody; and posterior horn. A tear involving >1 zone from the MMPH was defined as an extended tear; however, bucket-handle tears—involving the 3 zones—were excluded. Arthroscopic suture repair was indicated for unstable longitudinal tears in the red and white zones of the MM. Under the visualization of the posteromedial compartment of the knee by the 70° arthroscope through the intercondylar notch, the suture hook was passed and repaired through the posteromedial portal with absorbable sutures (No. 0 polydioxanone suture; Ethicon Inc). The repair was performed vertically with 3 to 5 mm space between sutures using a suture hook by the all-inside and modified inside-out techniques according to the extent of the tear 3,24 (Figure 3).

Arthroscopic images (A) during and (B) after all-inside repair with a modified inside-out technique performed on a tear that extended to the midbody.
After surgery, weightbearing was not allowed until 4 weeks and partial weightbearing was allowed at 4 weeks after surgery with a hinged knee brace worn for the full 8 weeks. Range of motion was allowed from 0° to 90° until 4 weeks then gradually increased after 4 weeks. The postoperative protocol required patients to avoid deep flexion (flexion beyond 100°) for the first 6 weeks.
Data Collection
Patients were assessed pre- and postoperatively using the following tools: Tegner activity scale; Lysholm knee score; Hospital for Special Surgery score; pivot shift/Lachman test; occurrence of a concomitant lateral meniscus (LM) tear; amount of anterior translation by stress radiography; injury mechanism (contact/noncontact); mechanical axis of the lower limb; posterior tibial slope 25 ; presence of tear extension to the midbody of the MMPH tears; and healing status (complete healing/partial healing/failure). The preoperative pivot shift and Lachman tests were classified according to the grade of laxity. 15
MRI examinations were performed pre- and postoperatively on a 3.0-T scanner (Aera; Siemens Medical Solutions) using an 8-channel knee coil (high definition (HD) time of repetition knee array) 2 years after surgery. Coronal and sagittal images were acquired using turbo spin-echo (TSE) proton density-weighted imaging, TSE fat-saturated T2-weighted imaging, T1-weighted sequence, axial imaging using TSE proton density-weighted imaging, and ACL oblique imaging using TSE fat-saturated T2-weighted imaging with a slice thickness of 1.5 mm and no space. MMPH longitudinal tears and their healing status were determined by an experienced musculoskeletal radiologist using an MRI scan for all patients included in the study. Signal changes on conventional MRIs were diagnosed according to the Stoller and Crues 3-stage classification, 31,48,53 where grade 0 was defined as a normal meniscus and where the meniscus demonstrated low signal intensity in the images; grade 1 was defined as an irregularly marginated intrameniscal signal that did not abut or communicate with the articular surface; grade 2 was defined as a linear signal that did not abut or communicate with the articular surface; and grade 3 was defined as a linear signal intensity abutting or communicating with the articular surface. Healing on postoperative MRI was categorized as follows: grade 0—complete healing; grade 1 or 2—partial healing; or grade 3—presence of additional tears or failure to heal (Figure 4). All MRI studies were reviewed by 2 musculoskeletal radiologists, with a 2-week interval between measurements.

Magnetic resonance images showing postoperative healing of the meniscus: (A) complete healing; (B) partial healing; and (C) failure.
Second-look arthroscopy was performed, along with MRI evaluation, if a patient required the removal of the tibial post-tie screw for ACLR. Meniscal healing was classified as follows 21 : (1) healed, full-thickness apposition of the original tear with <10% of the original tear remaining; (2) partially healed, ≥50% of the original tear was healed and stable, which was defined as no excessive anterior translation by probing; and (3) failed, >50% of the original tear was present or there were unstable meniscal fragments (Figure 5).

Second-look arthroscopic images showing (A) complete meniscal healing after repair and (B) a tear that failed to heal.
Statistical Analysis
Statistical analyses were performed using the SPSS software Version 21, (IBM). To compare the mean and categorical values, the data were analyzed using the Mann-Whitney U test, independent t test, paired t test, chi-square test, or Wilcoxon signed-rank test, depending on the results of the Shapiro-Wilk test, which was used to test the normality of the distribution. Binary stepwise logistic regression analysis was used to evaluate the risk factors for an unhealed meniscus (partially healed or additional/failed tear). The relevant factors were determined to be age, body mass index (BMI), sex, time from injury to surgery (>3 months), mechanism of injury (contact/noncontact), presence of varus alignment (>3° or <3°), posterior tibial slope, amount of anterior translation mechanical axis of the lower limb, presence of tear extension, and occurrence of a concomitant LM tear. Furthermore, the Tegner score, Lysholm score, Hospital for Special Surgery score, and pivot-shift grade, or Lachman score were also identified as risk factors. Statistical significance was set at P < .05.
The inter- and intraobserver reliabilities of the radiograph and MRI assessments were determined using the intraclass correlation coefficient, and the agreement between MRI and arthroscopic findings was determined using kappa values.
According to the post hoc power analysis for logistic regression analysis, the calculated power was 0.8, with a .05 α error, 0.5 of the assumed probability of healed MMPH tears with extension, and 0.8 of the assumed probability of healed MMPH tears without extension.
Results
A total of 83 patients were included in this study —52 patients (group 1) had MMPH peripheral longitudinal tears without tear extension, and 31 patients (group 2) had MMPH peripheral longitudinal tears with tear extension. The mean follow-up period was 24.7 months. There were no differences in pre- and postoperative results between groups (Tables 1 and 2). Most notably, there were no differences in the healing rate after meniscal repair (Table 2).
Preoperative Patient Characteristics a

a Data are reported as mean ± SD or n (%) unless otherwise indicated. Group 1, patients with tears located in the posterior compartment; group 2, patients with tears that extended to the midbody of the meniscus. BMI, body mass index; HKA, hip-knee-ankle; HSS, Hospital for Special Surgery; LM, lateral meniscus; SSD, side-to-side difference.
Comparison of the Postoperative Results Between Groups a
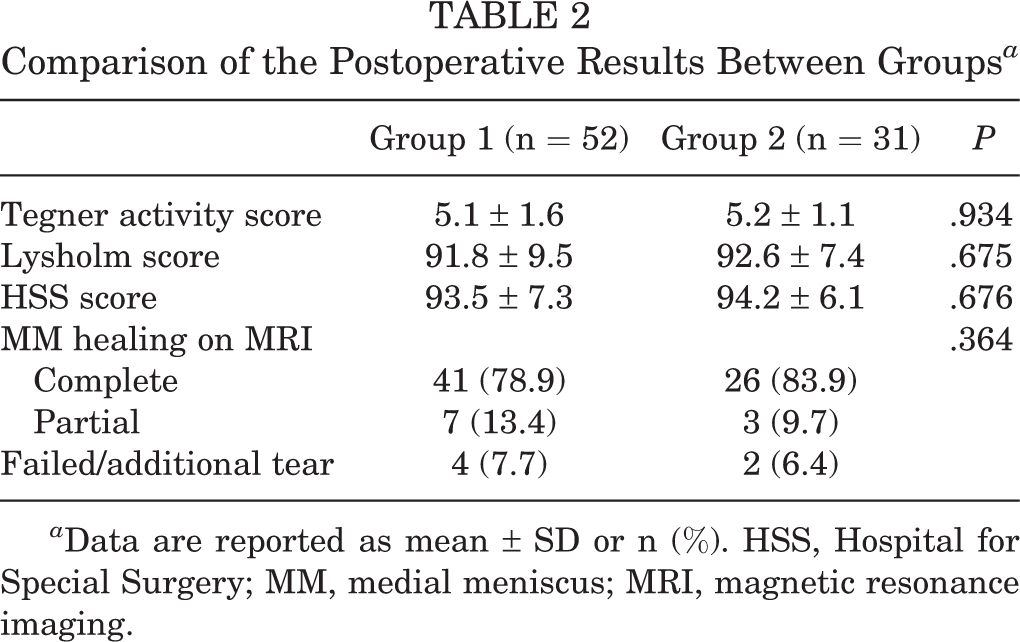
a Data are reported as mean ± SD or n (%). HSS, Hospital for Special Surgery; MM, medial meniscus; MRI, magnetic resonance imaging.
Based on postoperative MRI scans, 67 patients (80.7%) were classified into the completely healed group and 16 patients (19.3%) classified into the unhealed group (partially healed or failure/additional tears). There were no significant differences in postoperative outcomes or the rate of preoperative midbody tear extensions between the 2 groups (Table 3). The intraclass correlation coefficient values for the inter- and intraobserver reliability of the MRI findings were 0.753 and 0.813, respectively (P < .05), indicating good agreement.
Comparison of the Postoperative Results Between Healed Patients and Unhealed Patients a

a Data are reported as mean ± SD or n (%) unless otherwise indicated. HSS, Hospital for Special Surgery; SSD, side-to-side difference.
Second-look arthroscopy was performed in 51 patients (61.4%), and there were significant differences in the findings between MRI and arthroscopy results (P ≤ .001) (Table 4). The kappa value for the agreement was 0.559 (P ≤ .001), indicating a moderate agreement. Major differences between the MRI and arthroscopy findings were in partially healed patients; 6 of 10 (60%) patients who were determined to be partially healed based on MRI scans were categorized as completely healed based on arthroscopic findings (Table 4 and Figure 6).
Comparison of Postoperative Findings Between MRI and Second-look Arthroscopy a

a Data are reported as n or n (%). The bold P value indicates a statistically significant difference (P < .05). MM, medial meniscus; MRI, magnetic resonance imaging.

Images showing a knee with (A) partial healing finding on magnetic resonance imaging but (B) complete healing on arthroscopy.
In logistic regression analysis, which was used to identify the risk factors for unhealed menisci, higher BMI and lower preoperative Lysholm scores were identified as risk factors (Table 5).
Risk Factors for Unhealed Meniscus After Repair a
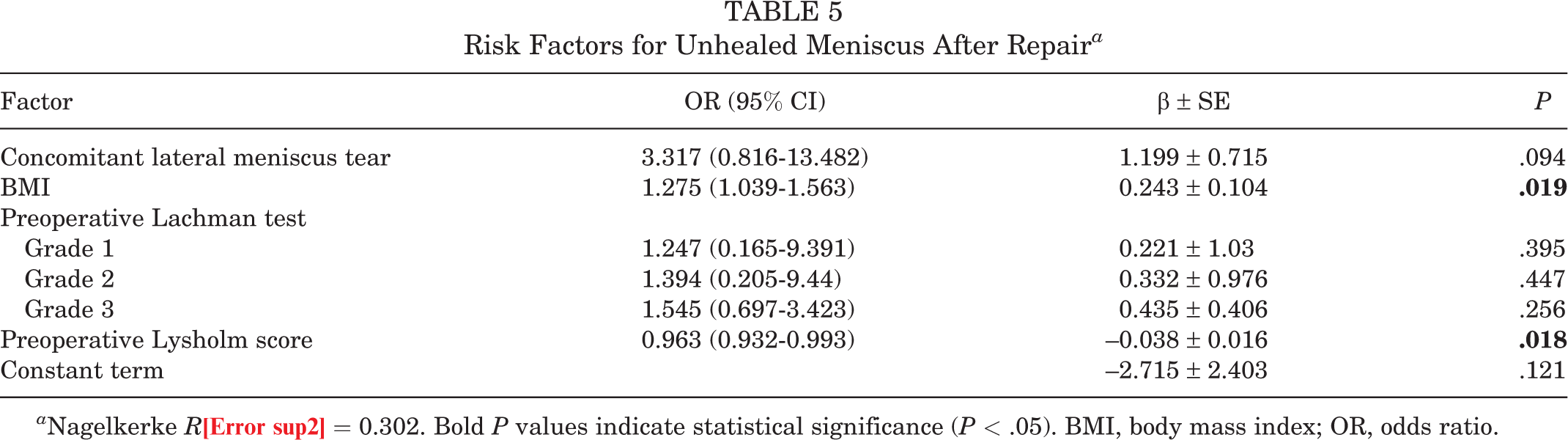
a Nagelkerke R2 = 0.302. Bold P values indicate statistical significance (P < .05). BMI, body mass index; OR, odds ratio.
Discussion
The most important findings in this study were that the complete healing rate of MMPH peripheral longitudinal tears after repair with ACLR was over 80% and that tear extension to the midbody of the MM did not affect the healing rate or clinical outcomes. Moreover, the risk factors associated with unhealed menisci were higher BMI and lower preoperative Lysholm scores. Patients with lower preoperative Lysholm scores may have more severe instability or dysfunction in the knee joints, which might not have been be assessed by clinical evaluation in this study; thus, it might affect the healing rate after repair.
The goal of meniscal repair during an ACLR is to protect the articular cartilage and restore meniscal function. Previous multicenter studies suggested that meniscal repair would be better than a meniscectomy in terms of protection of cartilage and clinical outcomes. 8,20 However, the clinical outcomes of MM repair were known to be less successful than those of LM repair. 21,54 Kim et al 21 reported that the healing rate was 80% with MM repair but 91.2% with LM repair. Recent systemic review studies reported that the overall healing rate ranged from 75.6% to 76.1% with MM repair but 80.5% to 87.4% with LM repair. 32,37 Moreover, several multicenter studies reported similar results, showing that MM repairs are associated with more frequent reoperations and worse patient outcomes compared with LM repair. 6,36,52 The MM is inherently less mobile and is known as the secondary restraint to anterior tibial translation; therefore, physiological and clinical healing might be more difficult than that of the LM. Furthermore, contraction of the semimembranosus muscle at its insertion along the posteromedial capsule may stress the peripheral part of the lesion, increasing meniscocapsular separation. 9,44 Thus, it is important to identify the risk factors that affect the healing rate of a repaired MM.
Many factors can affect the rate of meniscal healing, such as the stability or length of tears, 1,34,37,50 meniscal repair technique, 37,50,51 rehabilitation protocol, 37,50 chronicity, 1,30 or the stability of the ACL. 5,14,27 Although there is currently no consensus on the role of tear size in determining whether the MMPH peripheral longitudinal tears should be repaired or not, it is obvious that unstable MMPH peripheral longitudinal tears would be better repaired. 5,49,50 Furthermore, there was a lack of evidence regarding whether the tear size and extension would affect the clinical outcomes and healing rates after meniscal repair. In this study, there were no observed differences in the clinical outcomes and healing rates of MMPH peripheral longitudinal tears after repair, concerning the presence or lack of tear extension.
Only higher BMI and lower preoperative Lysholm scores were found to be risk factors for unhealed menisci on MRI scans (see Tables 2 and 5). There may be increased stress on meniscocapsular junctions of MMPH in patients with higher BMI, which could interrupt the healing of the repaired meniscus. 40 A lower preoperative Lysholm score may result in a severe preoperative disability in knee function, which could affect postoperative rehabilitation or stability, which might influence the healing potential of the repaired meniscus. However, other risk factors were not included in this study because of the low Nagelkerke R 2 value. In conclusion, this study suggests that repair of unstable MMPH peripheral longitudinal tears is worthwhile, with overall net positive outcomes, regardless of tear extension or tear size.
The repair techniques performed in this study were all-inside repair or modified inside-out repair techniques using a suture hook. In previous studies, repair techniques using suture devices were reported to have higher failure rates due to the incorrect deployment of the anchor of suture devices, especially in chronic cases. 42,47 Conversely, other authors have reported a high healing rate for MMPH peripheral longitudinal tears after suture repair with suture hooks, suggesting that vertically oriented sutures may be effective. 2,14,49 This suture technique can lift the peripheral meniscocapsular structure, which has been shifted distally, allowing for an anatomical repair. Similarly, a high healing rate of MMPH peripheral longitudinal tears after repair alongside a protective rehabilitation protocol was observed in this study, regardless of tear extension. Although there has been some debate over whether a protective rehabilitation protocol is necessary, especially regarding the weightbearing protocol, the failure rates were reported to be lower in strict nonweightbearing studies 45 (5.4%) than in partial weightbearing or full weightbearing studies 7,37 (11.5%-24.9%). Thus, the protective rehabilitation protocol was applied to patients after meniscal repair in our study.
Clinical symptoms or MRI findings are the most common method to evaluate the healing status after meniscal repair. 1,5,6,14,31,48,53 However, observation of failed healing after meniscal repair indicated that findings using an MRI scan may not entirely correlate with clinical failures or findings of second-look arthroscopy. 40,51,53,54 Several studies have noted that some incomplete or unhealed meniscal lesions identified on MRI scans were found to be completely healed at the time of second-look arthroscopy and healed clinically. 31,41 These MRI findings of incomplete or unhealed meniscal lesions could be found for many years after successful meniscal repair. 17,35 Thus, there are many other ways of improving the diagnostic accuracy of MRI scans, such as magnetic resonance arthrography, T2 mapping, and 3-dimensional MRI sequences with signal-to-noise ratio, and so forth. 14,41 The results of this study showed significant differences in findings between MRI scans and second-look arthroscopy, as well as moderate agreements (kappa = 0.559). Also, 6 of 10 (60%) patients identified as partially healed using MRI were categorized as being completely healed in arthroscopic findings, and this demonstrated clinical success, as shown similarly in previous studies. 17,35 This study presented differences in findings between MRI and arthroscopy, showing a higher success rate based on findings from arthroscopic evaluations, with a complete healing rate of 76.5% using MRI versus a complete healing rate of 88.2% using arthroscopy (see Table 4). The discrepancy may be due to the insensitivity of MRI to determine whether or not the residual signal in the body extended to the surface. 17,34,35 Steenbrugge et al 46 reported that these high signals in repaired meniscus corresponded to mucoid degeneration or scar tissue, which is difficult to distinguish from the healing meniscus.
Limitations
Our study had some limitations. First, we had a small sample size in each group and a short follow-up duration. Second, there were no comparisons between surgical techniques, such as the use of suture devices, abrasion, or trephination. Third, other factors that could affect the healing rate of the repaired menisci—such as anterolateral ligament injury, distance from the capsule to a meniscal tear, and methods of ACLR or rehabilitation—were not assessed. Last, second-look arthroscopy was not performed in all patients. In previous studies, the findings of MRI and arthroscopy were not correlated for the meniscal tears, especially for MMPH peripheral longitudinal tears. 11,23 Thus, it is unclear whether MRI findings correctly reflect the healing status of MMPH peripheral longitudinal tears and whether MRI evaluation has a significant risk of false-negative results. For this reason, there were no differences in clinical outcomes between completely healed and unhealed patients on MRI evaluation (see Table 3). Moreover, the stable lesions were not included in this study, which were left in situ without repair. Thus, it is difficult to conclude whether or not those stable lesions may be healed.
Conclusion
The overall complete healing rate of the repaired MMPH peripheral longitudinal tears with concomitant ACLR was 80.7% (67/83), and tear extension to the midbody did not affect the healing rate of the repaired meniscus. There were differences in the evaluation of healing of repaired menisci between MRI scans and arthroscopy surgery. The rate of complete healing as determined by arthroscopy—as supported by successful clinical outcomes—was higher than that by MRI. Suture repair for unstable MMPH peripheral longitudinal tears should be considered regardless of tear size.
Footnotes
Final revision submitted December 1, 2022; accepted January 17, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital at Gangdong (ref No. KHNMC 2019-08-003).