
Abstract
Background:
Patients with anterior cruciate ligament–deficient (ACLD) knees with medial meniscal posterior horn tears (MMPHTs) have been reported to demonstrate a combined stiffening and pivot-shift gait pattern compared with healthy controls. Movement asymmetries are implicated in the development and progression of osteoarthritis.
Purpose:
To investigate the knee kinematics and kinetic asymmetries in ACLD patients with (ACLD + MMPHT group) and without (ACLD group) MMPHTs while walking on level ground.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 15 patients with isolated unilateral ACL ruptures, 10 with unilateral ACL ruptures and MMPHTs, and 22 healthy controls underwent gait testing between January 2014 and December 2016. Between-leg differences (BLDs) in knee kinematics and kinetics were compared among participants in all groups.
Results:
The ACLD + MMPHT group demonstrated significantly greater BLDs in knee moments in the sagittal plane during the loading response phase than the ACLD and control groups. Compared with the control group, the ACLD and ACLD + MMPHT groups demonstrated significantly greater BLDs in knee angles in the sagittal plane during the midstance and terminal stance phases. Compared with the control group, significantly greater BLDs in knee rotation moments were found throughout the stance phase in both the ACLD and the ACLD + MMPHT groups. BLDs in lateral ground-reaction forces (GRFs) in the ACLD + MMPHT and ACLD groups were both significantly greater than the control group during the loading response phase. BLDs in anterior GRFs in the ACLD + MMPHT and ACLD groups were both significantly greater than the control group during the loading response phase. Only the ACLD + MMPHT group demonstrated greater BLDs in vertical GRFs than the control group during the loading response phase, while no significant differences were observed between the ACLD and control groups.
Conclusion:
The ACLD + MMPHT group demonstrated significantly more knee flexion moment asymmetries than the ACLD and control groups during the loading response phase. Both the ACLD + MMPHT and the ACLD groups demonstrated significant knee angle and moment asymmetries in the sagittal plane during the terminal stance phase than the control group. Both the ACLD + MMPHT and the ACLD groups demonstrated knee rotation moment asymmetries during the midstance and terminal stance phases compared with the control group. A rehabilitation program for ACLD patients both with and without MMPHTs should take into consideration these asymmetric gait patterns.
Keywords
Anterior cruciate ligament (ACL) rupture is a common injury, accounting for 20% of sports injuries to the knees. 17 An ACL rupture could cause abnormal knee kinematics and kinetics, 14 and lower limb asymmetries have been observed 19 in patients with ACL-deficient (ACLD) knees.
The incidence of osteoarthritis after ACL rupture has been reported to be over 50% in 10 years. 16 A medial meniscal posterior horn tear (MMPHT), which often occurs after ACL rupture, 29 influences stability in ACLD knees 1 and further increases the risk of posttraumatic osteoarthritis. Moreover, movement asymmetries are implicated in the development of osteoarthritis. 6 Asymmetrical lower limb loading alters chondrocyte synthesis and catabolic activities and makes the biochemical composition of articular cartilage inferior, 4,25 which is considered the mechanism of posttraumatic osteoarthritis. 4
However, limited information is available on knee asymmetries while walking in ACLD patients with and without MMPHTs. As far as we are aware, only 1 study has investigated gait alterations in knees with ACL ruptures and MMPHTs. 21 In that study, no significant differences in gait parameters between patients with ACL ruptures and those with both ACL ruptures and MMPHTs were observed. 21 The authors focused on only the injured legs and did not study the asymmetries between the injured and uninjured legs. 21 An assessment of asymmetry during walking will help evaluate dynamic instability and provide suggestions for a rehabilitation program and time for surgery in patients with ACL rupture.
The purpose of this study was to evaluate dynamic movement asymmetries during walking in ACLD patients with and without MMPHTs. The hypotheses were that (1) the ACLD + MMPHT group would demonstrate more movement asymmetries than the ACLD group, (2) gait asymmetries in the sagittal plane in the ACLD + MMPHT and ACLD groups would be significantly greater than those in the healthy controls, and (3) gait asymmetries in the axial plane in the ACLD + MMPHT and ACLD groups would be significantly greater than those among controls.
Methods
Ethical approval was obtained from the university’s ethics committee, and written informed consent was obtained from all participants. Patients diagnosed with an ACL rupture and scheduled for ACL reconstruction at our institute were selected for gait analysis. A total of 15 patients with a unilateral ACL rupture, cartilage defects less than grade II (according to the Outerbridge classification system 20 ), and no meniscal injuries were included in the isolated ACLD group. A total of 10 patients with a unilateral ACL rupture, cartilage defects less than grade II, and concomitant MMPHTs were included in the ACLD + MMPHT group. Among them, 6, 2, and 2 patients showed longitudinal, horizontal, and complex tears, respectively. Patients with injuries to the lateral meniscal or medial meniscal anterior horn were excluded from the ACLD + MMPHT group. The control group consisted of 22 participants with no history of musculoskeletal injuries or surgery in the lower extremities. Furthermore, no measurable ligamentous instability on clinical examination was noted.
Subjective knee function was evaluated using the International Knee Documentation Committee (IKDC) score, Lysholm score, and Tegner activity scale. 11 In addition, isokinetic strength of the knee extensor and flexor muscles was measured using an isokinetic dynamometer (Con-Trex MJ; Physiomed) at 60 and 180 deg/s.
All participants had a set of markers attached to their lower limbs to track segmental motion while walking. The detailed marker set was described in a previous study. 21 Anatomic markers were optimized based on a validated Plug-in-Gait model (Vicon) and taped to the following locations: anterior and posterior superior iliac spines; medial and lateral femoral epicondyles; malleoli; medial and lateral sides of the calcaneus; frontal and lateral aspects of the thigh and the shank; posterior part of the calcaneus; heads of the first, second, and fifth metatarsal bones; base of the first metatarsal bone; navicular; and hallux. 21 Then, 3-dimensional coordinate data were collected using an 8-camera motion capture system (Vicon MX; Oxford Metrics) at a sampling rate of 100 Hz. Ground-reaction forces (GRFs) were obtained using 2 embedded force plates (AMTI) at a sampling rate of 1000 Hz. Each participant was asked to undergo 5 successful trials. The mean value of 5 trials was used for analysis. None of the participants complained about pain during walking. Time-series data for the kinematic and kinetic variables were calculated using Visual3D software (C-Motion). Joint angles were calculated as Cardan angles between adjacent local segments in the order of flexion-extension, adduction-abduction, and internal rotation–external rotation. Joint moments, expressed as external moments, were calculated using an inverse dynamics approach and referenced to the proximal segment. Moments were normalized to body weight and standing height. For each of the kinematic and kinetic components, 101 discrete points corresponding to 0% to 100% of the stance phase at 1% intervals were normalized using a cubic spline.
The between-leg difference (BLD) was used to evaluate dynamic gait asymmetries. The BLD of each discrete kinematic and kinetic point in the ACLD and ACLD + MMPHT groups was calculated as follows:

where Yuninjured leg and Yinjured leg are magnitudes of the given kinematics or kinetics of the uninjured and injured legs, respectively.
The BLD of each discrete kinematic and kinetic point in the control group was calculated as follows:

where Ydominant leg and Ynondominant leg are magnitudes of the given kinematics or kinetics of the dominant and nondominant legs, respectively.
Paired t tests were used to compare peak isokinetic knee extensor and flexor strength between the injured and uninjured legs or between the dominant and nondominant legs. The BLD of each discrete kinematic and kinetic point was compared among the control, ACLD, and ACLD + MMPHT groups using 1-way analysis of covariance, with walking speed as a covariate, to eliminate the effects of walking speed on gait parameters. Post hoc analysis of covariance with the Bonferroni correction was performed between 2 groups. In this analysis of covariance study with a .05 significance level, sample sizes of 22, 15, and 10 were obtained from the control, ACLD, and ACLD + MMPHT groups, whose means were compared. Using post hoc power analysis, the total cohort of 47 patients achieved 99% power to detect differences among the means. All statistical analyses were performed using MATLAB (Version 2016b; MathWorks). A type I error rate ≤.05 was considered to indicate statistical significance.
Results
The characteristics of the participants were not significantly different among the 3 groups in terms of age (control, 29.95 ± 4.84 years; ACLD, 26.87 ± 4.65 years; ACLD + MMPHT, 27.10 ± 3.67 years), body mass index (control, 24.35 ± 3.36 kg/m2; ACLD, 25.32 ± 4.39 kg/m2; ACLD + MMPHT, 25.47 ± 2.90 kg/m2), and time since injury (ACLD, 9.47 ± 11.05 months; ACLD + MMPHT, 16.60 ± 21.10 months). Peak isokinetic strength values are shown in Table 1. The ACLD group walked with a significantly lower speed than the control group (ACLD, 1.16 ± 0.12 m/s; ACLD + MMPHT, 1.20 ± 0.12 m/s; control, 1.27 ± 0.11 m/s; P = .02).
Peak Isokinetic Strength a
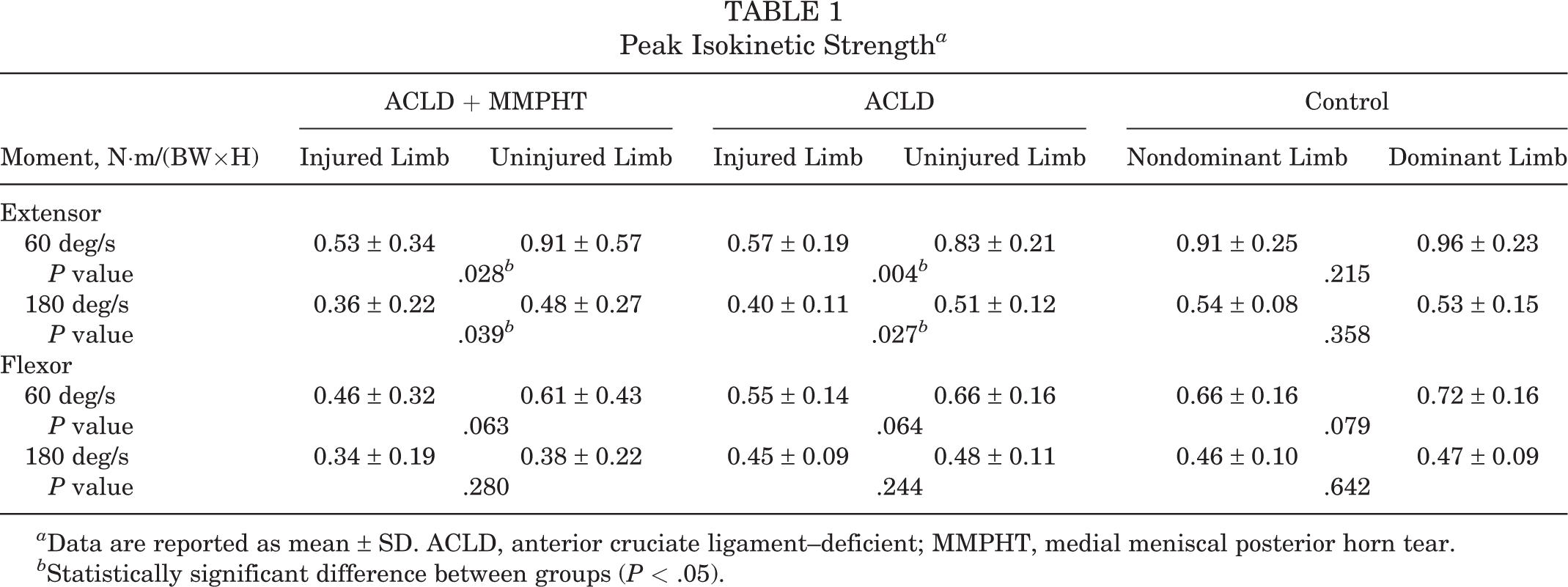
a Data are reported as mean ± SD. ACLD, anterior cruciate ligament–deficient; MMPHT, medial meniscal posterior horn tear.
b Statistically significant difference between groups (P < .05).
Subjective knee function according to IKDC score (ACLD, 64.32 ± 7.84; ACLD + MMPHT, 65.19 ± 9.14; P = .84), Lysholm score (ACLD, 66.33 ± 12.41; ACLD + MMPHT, 76.56 ± 13.06; P = .10), and Tegner activity scale 11 (ACLD, 3.85 ± 1.17; ACLD + MMPHT, 4.00 ± 1.66; P = .90) demonstrated no significant differences.
Compared with the control group, the ACLD and ACLD + MMPHT groups demonstrated a significantly greater BLD in knee angles in the sagittal plane during the midstance and terminal stance phases (Figure 1A). No significant differences in BLD in knee angles in the sagittal plane were observed between the ACLD and ACLD + MMPHT groups. The ACLD + MMPHT group demonstrated a significantly greater BLD in knee moments in the sagittal plane during the loading response phase than the ACLD and control groups (Figure 1B). Compared with the control group, the ACLD and ACLD + MMPHT groups demonstrated a significantly greater BLD in knee moments in the sagittal plane during the terminal stance phase (Figure 1B).
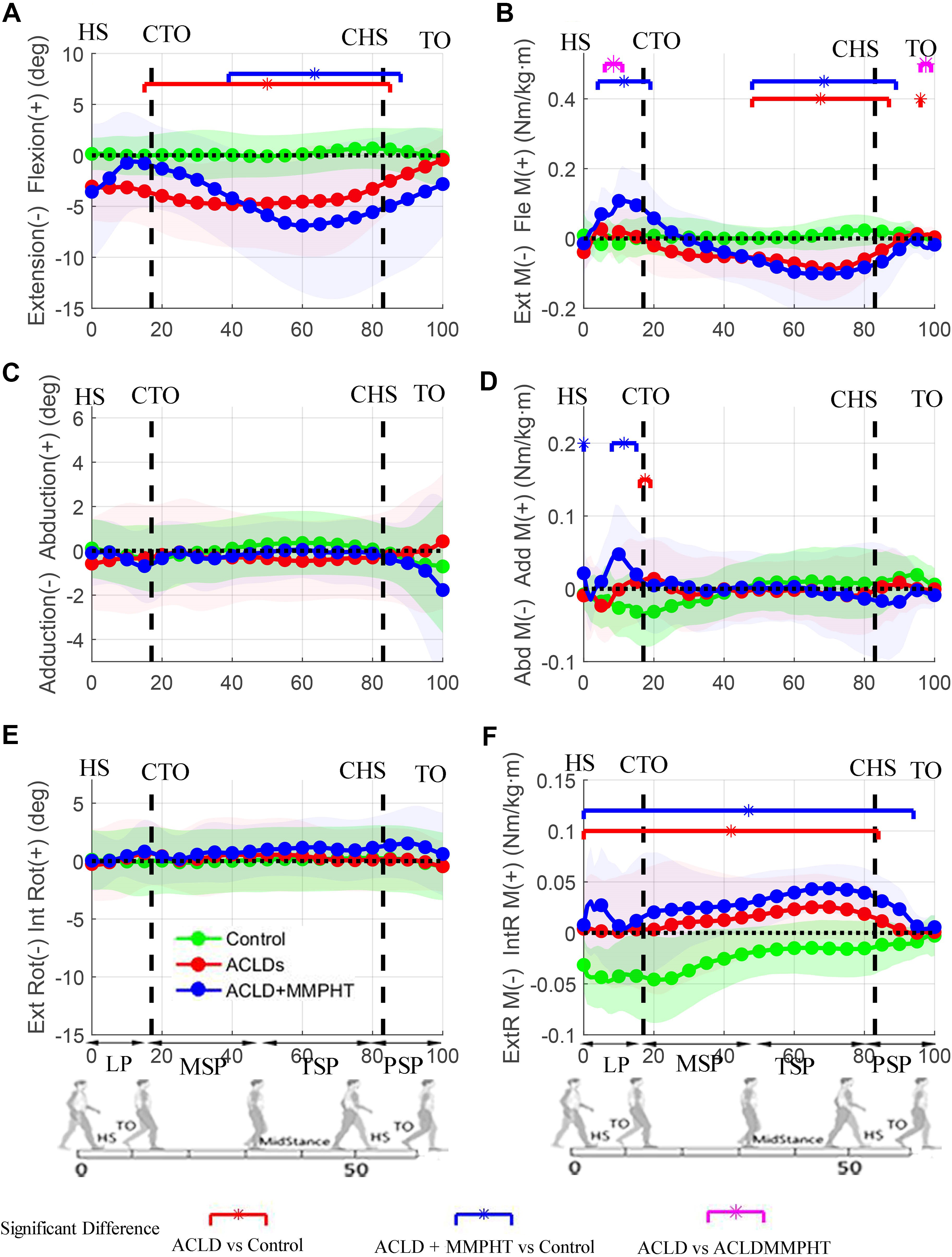
Difference between uninjured and injured knees of the anterior cruciate ligament–deficient (ACLD) and ACLD + medial meniscal posterior horn tear (MMPHT) groups versus the difference between dominant and nondominant knees of the control group in 3-dimensional kinematics and kinetics. Segments with significant statistical differences between the ACLD, ACLD + MMPHT, and control groups are marked with asterisks. The green shaded area represents the mean ± SD of the control group. CHS, contralateral heel strike; CTO, contralateral toe-off; HS, heel strike; LP, loading phase; MSP, midstance phase; PSP, preswing phase; TO, toe-off; TSP, terminal stance phase.
Compared with the control group, a significantly greater BLD in knee rotation moments was found throughout the stance phase for both the ACLD and ACLD + MMPHT groups (Figure 1F). No significant differences in BLD in knee rotation moments were observed throughout the stance phase between the ACLD and ACLD + MMPHT groups (Figure 1F). No significant differences in BLD in knee rotation angles were observed throughout the stance phase among the control, ACLD, and ACLD + MMPHT groups (Figure 1E).
The BLD in angles and moments in the coronal plane in the ACLD + MMPHT and ACLD groups showed no significant difference compared with that in the control group (Figure 1, C and D).
The BLD in lateral GRFs in the ACLD + MMPHT and ACLD groups was significantly greater than that in the control group during the loading response phase (Figure 2A). The BLD in anterior GRFs in the ACLD + MMPHT and ACLD groups was significantly greater than that in the control group during the loading response phase (Figure 2B). Only the ACLD + MMPHT group demonstrated a greater BLD in vertical GRFs than the control group during the loading response phase, while no significant differences were observed between the ACLD and control groups (Figure 2C). No significant differences in BLD in GRFs were observed between the ACLD and ACLD + MMPHT groups (Figure 2, A-C).
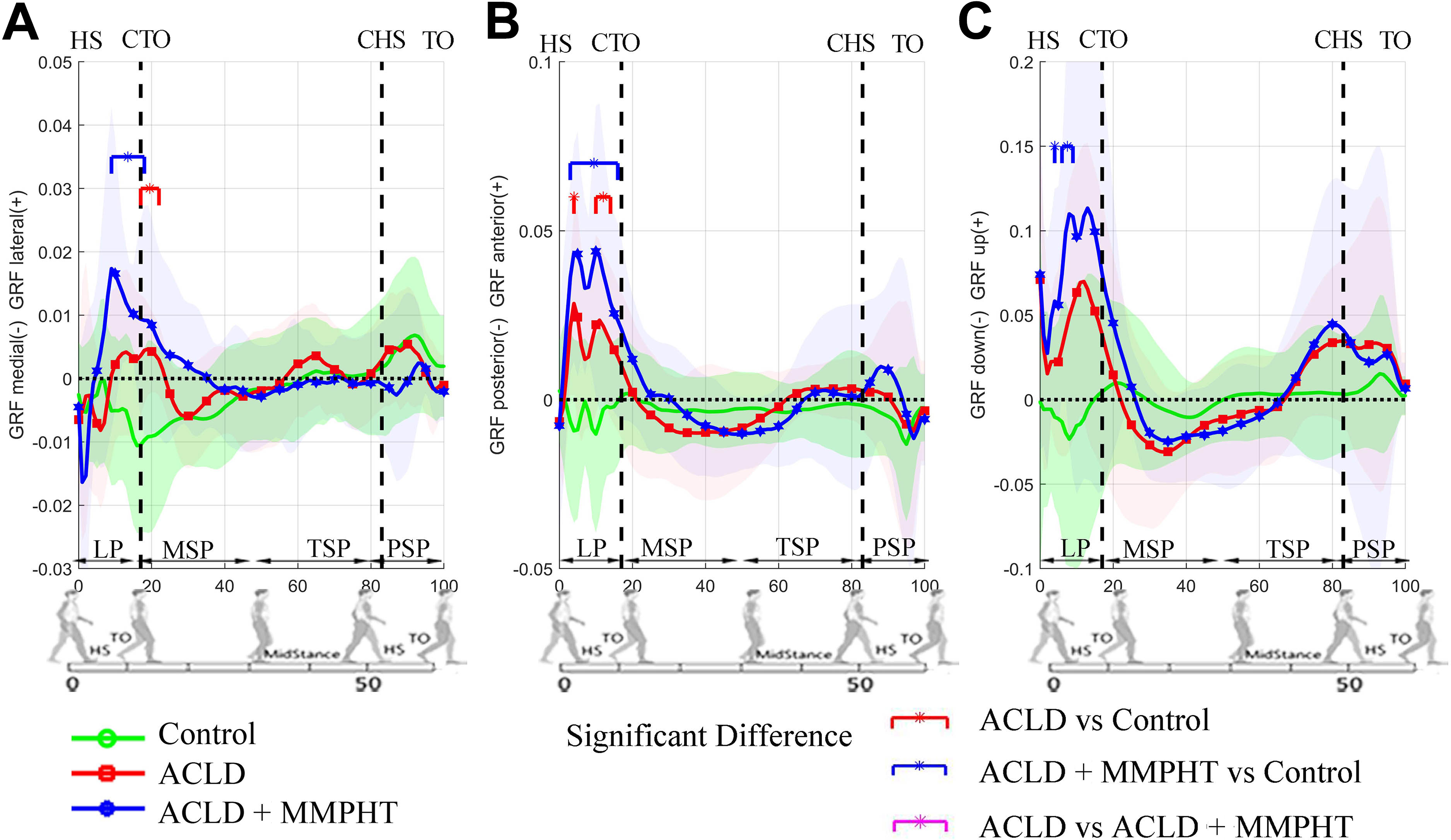
Ground-reaction force (GRF) asymmetries for the control, anterior cruciate ligament–deficient (ACLD), and ACLD + medial meniscal posterior horn tear (MMPHT) groups. CHS, contralateral heel strike; CTO, contralateral toe-off; HS, heel strike; LP, loading phase; MSP, midstance phase; PSP, preswing phase; TO, toe-off; TSP, terminal stance phase.
Discussion
We demonstrated in this in vivo study that MMPHTs increased asymmetries in flexion moments during the loading response phase of walking in patients with ACL ruptures. Compared with the control group, only the ACLD + MMPHT group demonstrated significant asymmetries in knee flexion moments (significantly lower flexion moments in the injured legs), while no significant difference in knee flexion moment asymmetries during the loading response phase was observed between the ACLD and control groups. In our study, extensor strength of the injured leg was significantly lower than that of the uninjured leg in both the ACLD and the ACLD + MMPHT groups. Therefore, one possible explanation for the asymmetries in knee flexion moments in the ACLD + MMPHT group may be weak quadriceps strength. Another possible explanation may be reduced neuromuscular control 10,18 caused by MMPHTs. A previous study found that neuromuscular control is related to interlimb asymmetry in patients undergoing ACL reconstruction, and a neuromuscular training program can significantly improve interlimb asymmetry. 23 As movement asymmetries could contribute to the development or progression of posttraumatic knee osteoarthritis, 4,25 more asymmetries during walking could cause a higher risk for posttraumatic osteoarthritis in the ACLD + MMPHT group than in the ACLD group. 16 Neuromuscular training in patients with ACL rupture and MMPHT could help to improve interlimb asymmetry to prevent or delay the initiation and development of osteoarthritis.
The ACLD and ACLD + MMPHT groups demonstrated significantly more asymmetries in knee flexion angles during the terminal stance phase than the control group. This means that compared with the contralateral uninjured knees, the knees in the ACLD and ACLD + MMPHT groups demonstrated extension deficiency during the terminal stance phase. Similarly, a previous study reported that knees with ACL rupture as well as knees with ACL rupture and MMPHT demonstrated extension deficiency compared with healthy control knees. 21 Extension deficiency in ACLD knees compared with uninjured knees has also been observed in previous studies. 2,3,13 Knee extension deficiency may be a protective strategy to avoid excessive tibial anterior displacement in the absence of a functional ACL. 8,24
The ACLD and ACLD + MMPHT groups demonstrated significant asymmetries during walking in knee rotation moments throughout the stance phase compared with the control group. Interestingly, the control group presented with higher rotation moment asymmetries during the loading response phase than the ACLD and ACLD + MMPHT groups. The ACLD + MMPHT and ACLD groups showed significant asymmetries during the terminal stance phase, which meant that the injured legs in the ACLD + MMPHT and ACLD groups showed lower external and internal rotation moments because of an imbalance of moments caused by external rotation muscles. Higher activity and a longer duration of activity of the biceps femoris have been observed during walking in the injured legs of patients with ACL ruptures compared with those of controls, 7,22 which may explain the reduced rotation moments.
Vertical GRF asymmetries and knee flexion moment asymmetries were observed in the ACLD + MMPHT group during the loading response phase of walking in this study. Dai et al 5 found that vertical GRF asymmetries predicted knee flexion moment asymmetries in ACL-reconstructed knees. Therefore, knee flexion moment asymmetries in the ACLD + MMPHT group may be caused by vertical GRF asymmetries. Training to improve GRF symmetries may be beneficial to improve knee moment symmetries in the ACLD + MMPHT group.
Knee kinematic asymmetry while walking is a critical parameter to assess dynamic joint function in patients with ACL ruptures. Abnormal knee biomechanics are associated with cartilage degeneration in patients undergoing ACL reconstruction. 15,26 Kinematic limb symmetry indexes at peak values while walking have been used as objective assessment tools by rehabilitation specialists to modify phases of a rehabilitation program based on an individual patient’s progression. 9 However, limb symmetry indexes frequently overestimate knee function in patients undergoing ACL reconstruction and may be related to a risk of repeat ACL injuries. 12,27 Some researchers have suggested the minimal clinically important difference as a threshold for clinically meaningful asymmetries (knee angles ≥3°; knee moments ≥0.04 N m/kg m) according to the results of 10 uninjured athletes. 28 However, as walking is a dynamic process, significant kinematic alterations have been observed in ACLD knees during the terminal stance phase. 21 Therefore, to evaluate dynamic limb asymmetries while walking, it is necessary to comprehensively assess the dynamic defects.
There are some limitations of this study. First, this study has a limited sample size because of the strict inclusion criteria. Thus, the results may be related to individual differences. However, the sample size achieved 99% power. Second, the time since injury may have affected the asymmetries of the ACLD and ACLD + MMPHT groups. Further studies must include patients with a similar time since injury.
Conclusion
The ACLD + MMPHT group demonstrated significantly greater knee flexion moment asymmetries than the ACLD and control groups during the loading response phase. Both the ACLD + MMPHT and the ACLD groups demonstrated significant knee angle and moment asymmetries in the sagittal plane during the terminal stance phase compared with the control group. Both the ACLD + MMPHT and the ACLD groups demonstrated significant knee rotation moment asymmetries during the midstance and terminal stance phases compared with the control group.
Footnotes
Final revision submitted January 14, 2020; accepted January 29, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: Financial support was received from the National Key Research and Development Program of China (2018YFF0301104), National Natural Science Foundation of China (31900943, 31900961, 81871761, 81330040, 81601927), Clinical Key Projects of Peking University Third Hospital (BYSY2017012), Beijing Municipal Natural Science Fund (7202232, 7171014), Capital Public Health Project (Z161100000116072), and China Postdoctoral Science Foundation (2018M631279). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the medical ethics committee of Peking University Third Hospital.