
Abstract
Background:
Arthroscopic osteocapsular arthroplasty (OCA) shows promising short-term outcomes for primary elbow osteoarthritis (OA). However, serial changes in clinical outcomes for medium-term follow-up are not well known.
Purpose:
To evaluate clinical outcomes after arthroscopic OCA in primary elbow OA from preoperative to short- and medium-term follow-up and to analyze the correlation between the time from short- to medium-term follow-up and the changes in clinical outcomes between the periods.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients with primary elbow OA who were treated with arthroscopic OCA between January 2010 and April 2020 were evaluated. Elbow range of motion (ROM), visual analog scale (VAS) for pain, and Mayo Elbow Performance Score (MEPS) were assessed preoperatively and at short-term (3-12 months) and medium-term (≥2 years) follow-up. The correlation between the time from short- to medium-term follow-up and the changes in clinical outcomes was analyzed using the Pearson correlation coefficient.
Results:
Included were 56 patients who underwent short-term follow-up (mean [range], 5.9 [3-12] months) and medium-term follow-up (62.2 [24-129] months) after arthroscopic OCA. When compared with preoperative values, significant improvements were seen at short-term follow-up: ROM (from 89.4° to 111.7°; P < .001), VAS for pain (from 4.9 to 2.0; P < .001), and MEPS (from 62.3 to 83.7; P < .001). From short- to medium-term follow-up, ROM decreased (from 111.7° to 105.4°; P = .001) while VAS for pain (from 2.0 to 1.4; P = .031) and MEPS (from 83.7 to 87.8; P = .016) improved. All outcomes improved significantly at medium-term follow-up as compared with preoperative values (P < .001 for all). The time between short- and medium-term follow-up had a significant positive correlation with decreased ROM (r = 0.290; P = .030) and a significant negative correlation with improvement in MEPS (r = –0.274; P = .041).
Conclusion:
Serial assessment of patients with primary elbow OA who underwent arthroscopic OCA showed that the clinical outcomes improved from preoperative assessment to short- and medium-term follow-up, although ROM decreased between short- and medium-term follow-up. VAS for pain and MEPS showed continued improvement until medium-term follow-up.
Primary elbow osteoarthritis (OA) affects up to 2% of the general population, with men being 4 times more likely to be affected than women. 26 The high-risk population for primary elbow OA includes manual laborers, overhead-throwing athletes, and individuals dependent on crutches who experience greater joint reactive forces at the elbow. 3,10,26 Common clinical manifestations of primary elbow OA are pain at the terminal range of motion (ROM) and decreased ROM as the result of the formation of marginal osteophytes and loose bodies, which leads to functional limitations in activities of daily life. 6,22
Arthroscopic osteocapsular arthroplasty (OCA) is a reliable treatment option for primary elbow OA, which reshapes the arthritic elbow and releases the contracted capsule to improve pain and ROM. 11,25 When compared with open OCA, which requires a large incision and results in extensive soft tissue injury, the major advantage of arthroscopic OCA is its minimal invasiveness, which leads to less soft tissue injury, postoperative pain, and intraoperative bleeding as well as earlier rehabilitation. 5,21 Arthroscopic elbow surgery, however, requires a thorough understanding of the anatomy and pathologic structures, as well as surgical experience and familiarity, to enable successful outcomes while avoiding neurovascular structures. 8,20
Although arthroscopic OCA has shown promising short-term outcomes in patients with primary elbow OA, operated elbows may undergo significant arthritic changes over time because primary elbow OA is a progressive degenerative disease. However, only a few studies to date have assessed the serial postoperative results for medium- and long-term follow-up, and little is known about the natural course of primary elbow OA after surgery. 1,4,9,14,16,17,24
The purpose of this study was (1) to assess clinical outcomes serially from preoperative assessment to short- and medium-term follow-up after arthroscopic OCA in primary elbow OA and (2) to analyze the correlation between the time from short- to medium-term follow-up and the changes in clinical outcomes between the periods. We expected that while all clinical outcomes would improve at short-term follow-up, ROM would decrease and pain and functional scores would further improve at medium-term follow-up. Moreover, we assumed that as the time from short- to medium-term follow-up lengthened, the improvement in pain and function scores would lessen and ROM would decrease.
Methods
This single-center study included patients with primary elbow OA who underwent arthroscopic OCA between January 2010 and April 2020. The study protocol was approved by the institutional review board of our institution. Primary elbow OA was diagnosed by clinical assessment, including determinations of pain and ROM limitations, and confirmed by plain radiograph. Patients who did not show improvements for ≥6 months after nonoperative treatment were indicated for surgery. A computed tomography scan was performed for preoperative evaluation of the severity of OA and surgical planning. Radiologic staging of OA was performed according the classification of Kwak et al, 15 in which grades 0 and 1 were classified as mild, 2 as moderate, and 3 as severe. All patients underwent clinical evaluation, electromyography, and nerve conduction assay to identify the occurrence of peripheral ulnar nerve neuropathy. All patients were diagnosed and surgically treated by a single senior surgeon (I.-H.J.).
Inclusion and Exclusion Criteria
Patients were included if they were ≥18 years old, had been diagnosed with primary elbow OA and treated by arthroscopic OCA, and had ≥2 years of follow-up data. Patients were excluded if they had previously undergone surgery on the same elbow, had undergone concurrent surgery on the same elbow (other than mini-open ulnar nerve release during arthroscopic OCA), or had insufficient clinical outcome data.
Clinical Outcomes
From review of the patient records, the following clinical outcomes were evaluated: ROM (overall ROM, amount of extension contracture, amount of flexion), visual analog scale for pain (VAS pain) in which scores ranged from 0 (no pain) to 10 (worst pain), and Mayo Elbow Performance Score (MEPS). Complications and the need for revision procedures were determined according to chart review. Passive ROM was measured using a goniometer by a clinical nurse specialist who had 10 years of experience in elbow care, and the measurements were rounded to the nearest 5°. The clinical outcomes were measured at 3 time points with serial analysis: preoperatively, at short-term follow-up (3-12 months postoperatively), and at medium-term follow-up (≥2 years postoperatively). Short-term follow-up at 3 months after surgery was assessed because in our experience, most patients reach relatively stable ROM around that time and are asked to perform ROM exercises until then.
We evaluated the correlation between the time from short- to medium-term follow-up and changes in clinical outcomes during that time. Changes in ROM were assessed with 2 methods: simple subtraction (ROM subtraction) and as a percentage (ROM ratio), calculated as follows:

The ROM ratio was used because as poorer preoperative ROM is related to more severe OA, it is more difficult to achieve the same degree of improvement as elbows with better preoperative ROM.
Surgical Procedure
Patients were placed in the lateral decubitus position, and an intraoperative tourniquet was inflated. A mini-open ulnar nerve release was performed before the arthroscopic procedure if patients showed any further flexion <90° or positive ulnar nerve symptoms with positive electromyography/nerve conduction assay findings. A skin incision of approximately 2 cm was made between the medial epicondyle and olecranon along the ulnar nerve. After careful dissection of subcutaneous tissue, the ulnar nerve was identified and protected using a nerve sling. An arthroscopic camera was then introduced to visualize and dissect the proximal and distal ends of the deeper portion of the ulnar nerve that were not in contact with the skin. Using arthroscopic camera guidance, we confirmed whether the arcade of Struthers and the fascia between the heads of the flexor carpi ulnaris were fully released and whether the ulnar nerve was freely mobilized. Additional procedures for the ulnar nerve (eg, anterior transposition) were not performed.
After the mini-open ulnar nerve release and ulnar nerve protection were performed, posterior and posterolateral portals were created to access the posterior compartment. Osteophytes at the olecranon fossa and olecranon tip were first removed. To improve the range of flexion, the posterior capsule (including the triceps), posteromedial corner (including the posterior band of the medial collateral ligament), and posterolateral corner were released. After the procedure in the posterior compartment, proximal anteromedial, proximal anterolateral, and anterolateral portals were created to access the anterior compartment. A freer was used to elevate the muscles of the anterior compartment to improve visualization. Spurs at the coronoid fossa and tip, radial head, and radial fossa were removed, and the anterior capsule was released to improve the range of extension.
A compressive dressing was applied after surgery. At day 1 postsurgery, the compressive dressing was changed to a simple dressing, and patients were educated to perform active-assisted ROM exercises without any kind of immobilization under the guidance of the clinical nurse specialist. After discharge, patients were allowed to use their elbows in the range without reaching pain and were educated to perform ROM exercises at home for 3 months, 6 times a day, reaching full extension and flexion 10 times with 10 seconds of interval at each cycle.
Statistical Analysis
Continuous variables are reported as mean and standard deviation and ordinal and nominal variables as number and percentage. Repeated measures analysis of variance with post hoc analysis was used to compare the values measured at the preoperative assessment and short- and medium-term follow-ups. Post hoc analysis was performed using Bonferroni correction. The Pearson correlation coefficient (r) was used to assess the association between the time from short- to medium-term follow-up and changes in clinical outcomes. A Kaplan-Meier survival curve was generated to determine revision-free survival. All statistical analyses were performed using SPSS Statistics for Windows Version 21 (IBM), with P < .05 defined as statistically significant.
Results
Of the 77 patients with primary elbow OA who underwent arthroscopic OCA, 21 were excluded for a history of other surgery on the same elbow (n = 16), concurrent surgery on the same elbow (n = 4), and insufficient data (n = 1). Ultimately, 56 patients with a mean medium-term follow-up of 62.2 months (range, 24-129) were included in the study. The detailed demographic data of the patients are summarized in Table 1.
Preoperative Characteristics of the Study Patients (N = 56)

Table 2 and Figure 1 show the clinical outcomes measured preoperatively, at short-term follow-up, and at medium-term follow-up. When compared with the preoperative measurements, significant improvements were seen at short-term follow-up in ROM (from 89.4° ± 20.2° to 111.7° ± 17.6°), amount of extension contracture (from 18.3° ± 10.3° to 9.5° ± 8.5°), amount of flexion (from 107.5° ± 13.6° to 121.1° ± 11.6°), VAS pain (from 4.9 ± 2.3 to 2.0 ± 1.7), and MEPS (from 62.3 ± 10.6 to 83.7 ± 13.1) (P < .001 for all). At medium-term follow-up, ROM (105.4° ± 20.4°; P = .001) and amount of flexion (118.2° ± 12.9°; P = .018) decreased significantly and amount of extension contracture (12.9° ± 11.1°; P = .003) increased significantly as compared with short-term follow-up, and VAS pain (1.4 ± 1.8; P = .031) and MEPS (87.8 ± 12.1; P = .016) improved significantly. All clinical outcomes improved significantly between preoperative assessment and medium-term follow-up (P < .001 for all).
Clinical Outcomes at Preoperative Assessment and Short- and Medium-term Follow-up a
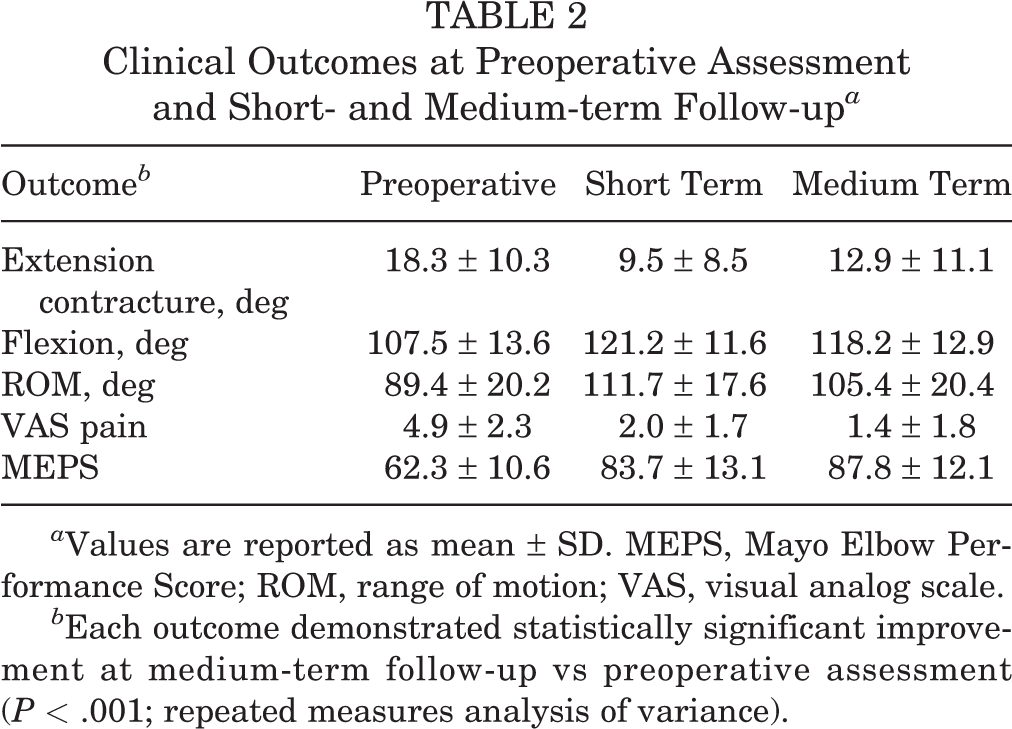
a Values are reported as mean ± SD. MEPS, Mayo Elbow Performance Score; ROM, range of motion; VAS, visual analog scale.
b Each outcome demonstrated statistically significant improvement at medium-term follow-up vs preoperative assessment (P < .001; repeated measures analysis of variance).

Serial assessment of (A) ROM, (B) VAS pain, and (C) MEPS at the preoperative, short-term follow-up, and medium-term follow-up evaluations. The Xs represent the means, the horizontal lines represent the medians, the boxes represent interquartile ranges, and the whiskers represent maximum and minimum values. ROM, range of motion; VAS, visual analog scale; MEPS, Mayo Elbow Performance Score. *P < .05.
There was a significant positive correlation between the time from short- to medium-term follow-up and decreased ROM, as assessed by ROM subtraction (r = 0.290; P = .030) and ROM ratio (r = 0.302; P = .024), and there was a significant negative correlation between follow-up interval and improvement in MEPS (r = –0.274; P = .041) (Figure 2). There was no significant correlation between the follow-up interval and improvement in VAS pain (r = –0.250; P = .063).

Correlation between time from short- to medium-term follow-up and changes in clinical outcomes according to (A) ROM subtraction, (B) ROM ratio, (C) VAS pain, and (D) MEPS. ROM, range of motion; VAS, visual analog scale; MEPS, Mayo Elbow Performance Score. *P < .05.
Three (5.4%) patients had skin eruptions without signs of deep infection during the immediate postoperative period and were managed by routine dressing under close observation, which were all resolved within 2 months. Two (3.6%) patients underwent revision arthroscopic OCA: one for elbow pain and decreased ROM (95°; extension-flexion arc, 30°-125°) at 107 months after surgery and the other for functional discomfort from decreased ROM (70°; extension-flexion arc, 20°-90°) at 26 months after surgery. Both patients showed improvements in ROM (110° [extension-flexion arc, 20°-130°] and 95° [extension-flexion arc, 10°-105°], respectively), VAS pain, and MEPS with no other complications at 12 and 25 months. Survival from revision surgery was 98.1% at 60 months and 81.7% at 120 months (Figure 3).

Kaplan-Meier survival curve for revision-free survival after primary arthroscopic OCA in patients with primary elbow OA.
Discussion
Our study on patients with primary elbow OA showed that ROM, VAS pain, and MEPS improved significantly at medium-term follow-up after arthroscopic OCA when compared with preoperative values (P < .001 for all). The ROM decreased from short- to medium-term follow-up (P = .001), while VAS pain and MEPS showed serial improvements from the preoperative assessment to short-term follow-up (P < .001 for both) and from short- to medium-term follow-up (P = .031 and .016, respectively). The time from short- to medium-term follow-up had a significant positive correlation with decreased ROM and a significant negative correlation with improvement in MEPS.
Serial changes in clinical outcomes after arthroscopic OCA are not well known, while some studies have noted the progression of OA after open OCA. Oka 22 reported that all 20 study patients experienced some degree of recurrent OA at a minimum follow-up of 8 years, and Antuña et al 2 found that recurrent osteophytes were in more than half of the elbows at a mean follow-up of 80 months. Wada et al 28 reported that the mean extension was significantly worse at 121 months than at 12 months (26° vs 19°; P = .009) after open OCA. Kim et al 13 compared clinical outcomes after arthroscopic OCA between postoperative 6 months and final follow-up (mean [range], 55.4 [24-100] months) and noted improvements in VAS pain (from 2.1 to 0.8) and MEPS (from 86.8 to 89.5) at the final follow-up as opposed to a decrease in extension (from 9.9° to 11.2°) and flexion (from 126° to 115.3°). Even though Kim et al 13 did not perform statistical analysis for serial assessment, their results were consistent with those of our study.
In our study, ROM decreased at medium-term follow-up versus short-term follow-up, whereas VAS pain and MEPS showed serial improvements. In other words, ROM started to decrease at some point between the short- and medium-term follow-up, while VAS pain and MEPS continued to improve at the medium-term follow-up. Decreases in ROM at medium-term follow-up are considered a result of the progression of OA. Because OCA is a procedure for reshaping bony contours, osteophytes may form again. However, OA progression is a slow process, and its progression may not always be accompanied by the recurrence of symptoms or the need for revision surgery. 19
Serial improvements in VAS pain and MEPS can be interpreted in 2 aspects. First, as pain and functional score depend on the patient’s subjective feeling, adaptation to postoperative status over time might serially improve the VAS pain and MEPS regardless of OA progression. Second, the short-term follow-up was performed within a relatively wide window of postoperative 3 and 12 months, which means that treatment responses in the early short-term period without enough rehabilitation could have been included, which may be related to insufficient recovery and persistent pain. As a result, insufficient improvements in the short-term period may lead to seemingly serial improvements in the medium-term VAS pain and MEPS.
Favorable short-term outcomes have been reported in primary elbow OA after arthroscopic OCA. 1,9,14,16 In contrast, medium-term follow-up studies are relatively lacking, and they showed inconsistent outcomes. MacLean et al 17 studied 21 elbows with a mean follow-up of 66 months and showed significant improvements in functional outcomes as assessed by the Disabilities of the Arm, Shoulder and Hand score (from 34.0 to 12.7; P = .001); however, fixed flexion deformity (from 11° to 8°; P = .21) and ROM flexion (136° to 135°; P = .79) did not show significant improvements. Rettig et al 24 reported a mean ROM gain of 30° in 17 patients with a mean follow-up of 65 months, albeit without statistical analysis. DeBernardis et al 7 noted improvements in extension (from 118.1° to 126.7°), flexion (from 26.2° to 11.3°), and VAS pain (from 6.1 to 1.7) in 36 patients with a mean follow-up of 7.9 years, albeit without statistical analysis of the primary elbow OA group. Kim et al 13 found significant improvements in extension (from 17.5° to 11.2°; P < .05), flexion (from 101.5° to 115.3°; P < .05), VAS pain (from 4.2 to 0.8; P = .009), and MEPS (from 55.8 to 89.5; P = .013) in 43 patients with primary elbow OA. In our current study, ROM, VAS pain, and MEPS improved significantly at a mean follow-up of 62.2 months. The rate of revision surgery in our study patients was 3.6%, and survival from revision surgery was 81.7% at 120 months after primary surgery, which is comparable with the rates in previous studies that assessed short- and medium-term outcomes of arthroscopic OCA. 1,2,9,13,16,18,23,27,28 These findings suggest that arthroscopic OCA is a reliable and safe treatment option in primary elbow OA at medium-term follow-up.
To better understand the changes in clinical outcomes after surgery, we assessed the correlation between the time from short- to medium-term follow-up and the changes in clinical outcomes. While previous studies showed that ROM decreased at final follow-up as compared with 6 months or 1 year, the correlation between the time interval and the amount of decrease has not been investigated. 13,28 In our study, there was a significant positive correlation between the time interval and decreased ROM (ROM subtraction and ROM ratio) between the follow-up intervals. In terms of improvement in MEPS, there was a significant negative correlation with the time interval. A negative correlation of improvement with time interval could be a potential sign of the start of aggravation, which suggests that even though MEPS showed significant serial improvement until medium-term follow-up, it may reach a plateau or start to decline at some point during long-term follow-up.
In this study, we used the concept of ROM ratio and ROM subtraction together while assessing the correlation between the time interval and changes in ROM. We did so because the extent of ROM improvement is different from the extent of OA improvement. Less preoperative ROM is usually related to more progressed OA, and it is more difficult to achieve the same extent of ROM improvement in patients with progressed OA. For example, a 40° improvement from 60° to 100° is thought to be more difficult to achieve than a 40° improvement from 100° to 140°. Therefore, we also used the concept of ROM ratio, which is the percentage change. Although we found significant correlations between the ROM ratio and time interval, a validation study of this definition has not been performed, and further study is required.
Limitations
This study had several limitations. First, as radiologic outcomes were not included in this study, we could not assess the degree of OA progression. Further studies analyzing serial radiologic changes would help assess the correlation between these clinical outcomes and radiologic progression. Second, this was a retrospective study with a relatively small study population. Third, ROM measurements in this study were accurate to only 5°, and the accuracy of the statistical analysis was limited. A correction formula for P values of the t tests was developed; however, we could not apply this because we used analysis of variance to compare the outcomes at the 3 time points. 29 Fourth, concomitant mini-open ulnar nerve release was performed for patients who met the criteria, and this additional procedure might have affected the postoperative clinical outcomes. Yet, a previous study compared outcomes after arthroscopic OCA between patients who underwent mini-open ulnar nerve release (according to the criteria also used in this study) and patients who did not and reported comparable postoperative ROM, VAS pain, and MEPS between the groups after 4 years of follow-up. 12 Despite limitations, this was the largest study that reported the medium-term follow-up of such patients and the first study to analyze the serial outcomes after arthroscopic OCA using statistical analysis. Furthermore, because a single surgeon performed all operations and provided postoperative care to all patients, the results are likely reliable.
Conclusion
Serial assessment of patients with primary elbow OA who underwent arthroscopic OCA showed that the clinical outcomes were improved from preoperative assessment to short- and medium-term follow-up. Specifically, ROM had decreased between short- and medium-term follow-up while VAS pain and MEPS showed continued improvement until medium-term follow-up.
Footnotes
Final revision submitted December 1, 2022; accepted January 19, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Asan Medical Center (No. 2022-0454).