
Abstract
Background:
Meniscal tear in older adults often accompanies knee osteoarthritis and is commonly treated with arthroscopic partial meniscectomy (APM) when patients have persistent pain after a trial of physical therapy. Cross-sectional evidence suggests that synovitis is associated with baseline pain in this patient population, but little is known about the relationship between synovitis and postoperative recovery or progression of knee osteoarthritis.
Purpose/Hypothesis:
Intra-articular extended-release triamcinolone may reduce inflammation and thereby improve outcomes and slow disease progression. This article presents the rationale behind the Corticosteroid Meniscectomy Trial (CoMeT) and describes its study design and implementation strategies.
Study Design:
Randomized controlled trial.
Methods:
CoMeT is a 2-arm, 3-center, randomized placebo-controlled trial designed to establish the clinical efficacy of extended-release triamcinolone administered via intra-articular injection immediately after APM. The primary outcome is change in Knee injury and Osteoarthritis Outcome Score Pain subscore at 3-month follow-up. Synovial biopsy, joint fluid aspirate, and urine and blood sample analyses will examine the associations between various objective measures of baseline inflammation and pre- and postoperative outcome measures and clinical responses to triamcinolone intervention. Quantitative 3-T magnetic resonance imaging will evaluate cartilage and meniscal composition and 3-dimensional bone shape to detect early joint degeneration.
Results:
We discuss methodologic innovations and challenges.
Conclusion:
To our knowledge, this is the first randomized double-blind clinical trial that will analyze the effect of extended-release triamcinolone acetonide on pain, magnetic resonance imaging measures of structural change and effusion/synovitis, soluble biomarkers, and synovial tissue transcriptomics after APM.
Keywords
Symptomatic knee osteoarthritis (OA) is a costly and disabling degenerative disease affecting 14 million adults in the United States and is one of the leading causes of disability worldwide. 8,25 Meniscal tear with pain and mechanical symptoms of catching and locking is a phenotype of early knee OA. 9,10,23 In patients who do not achieve pain relief from physical therapy, arthroscopic partial meniscectomy (APM) is a commonly elected procedure that has been shown to lead to a clinically significant improvement in symptoms in about 70% of cases. 13,19,32 Outcomes of APM are variable, however, 13,19,32 and the variability in outcomes remains unexplained. This knowledge gap is important since identification of modifiable drivers of variability may point to strategies to improve postoperative pain and patient satisfaction.
Synovitis, or inflammation of the synovial lining of the knee joint, has been found to be an important contributor to the symptomatology and progression of OA. 1,26,28,29 Furthermore, in cross-sectional analyses, synovitis has been associated with worse baseline pain in patients undergoing APM. 6 Thus, synovitis and joint inflammation may be drivers of persistent pain and variable outcomes in patients post-APM.
Triamcinolone acetonide, a glucocorticoid, has ameliorated synovitis-associated inflammation and outcomes in animal and human studies of anterior cruciate ligament injury. 16,30 However, the effects of triamcinolone on inflammatory and cellular components of the synovium in joints with early OA and degenerative meniscal injury have not been studied in a randomized controlled trial. We designed a 150-person randomized placebo-controlled trial stratified by the presence of reactive synovitis to test the clinical efficacy of intra-articular extended-release triamcinolone administration immediately post-APM. The injection will be administered at the time of APM to maximize the exposure of synovial tissue to the anti-inflammatory glucocorticoid medication immediately after the event presumed to incite the joint inflammation. The primary outcome for the trial is change in the Knee injury and Osteoarthritis Outcome Score (KOOS)-Pain subscore from baseline to 3 months post-APM. We will use stratified permuted-block randomization to ensure adequate balance of synovitis between the treatment groups, and we will use synovitis-stratified analysis to evaluate whether patients with inflamed synovium are likely to experience greater improvement in KOOS-Pain from the treatment than patients without inflammation. The Corticosteroid Meniscectomy Trial (CoMeT) sponsor is the Arthritis Foundation, which supports all study-related activities. Pacira BioSciences will provide all doses of extended-release triamcinolone (Zilretta) free of charge and support collection and analysis of biospecimens.
SPECIFIC AIMS
Specific Aim 1
Specific aim 1 is to perform a randomized controlled double-blind trial to evaluate the efficacy of extended-release triamcinolone for the relief of pain after APM.
We hypothesize that patients injected with the drug immediately post-APM will have greater improvement of pain on patient-reported outcomes (PROs) at 3 months after surgery than placebo-injected controls and that these improvements will be maintained at 6 and 12 months.
Specific Aim 2
Specific aim 2 is to characterize structural damage in knees in placebo controls vs subjects receiving, immediately post-APM, extended-release triamcinolone injections using quantitative magnetic resonance imaging (MRI) at baseline, 3 months, and 1 year.
We will quantify cartilage and meniscal tissue composition using T1ρ and T2 imaging and the thickness/volume and grade of OA lesions (cartilage defects and thinning, bone marrow edema–like lesions, effusion/synovitis) using a semi-quantitative scoring system and quantitative thickness/volume calculations. We will also quantify 3-dimensional (3D) bone shape using non–fat-saturated 3D turbo spin echo (TSE) images and statistical shape modeling. We hypothesize that the placebo-injected knees will have significantly greater baseline to 1-year increases (worsening) in cartilage T1ρ and T2 and significantly larger changes in bone shape than those injected with triamcinolone acetonide immediately post-APM.
Specific Aim 3
Specific aim 3 is to explore the associations of biomarker changes in joint fluid, urine, serum, and synovial tissue with 3- and 12-month post-APM changes in pain and to determine which biomarkers respond to triamcinolone treatment and/or are predictive of pain responses to the treatment.
Synovial fluid, synovial tissue, urine, and serum will be collected at surgery, and urine and serum will be collected at the 3- and 12-month postoperative visits. We hypothesize that subjects with the greatest levels of inflammatory biomarkers at baseline will have the best response to treatment (ie, greatest pain reduction).
Specific Aim 4
Specific aim 4 is to explore the relationships between markers of synovial inflammation and PROs.
Combined proteogenomic single-cell profiling (CITE-seq; cellular indexing of transcriptomes and epitopes by sequencing) will be used to define cell populations in the synovium of the 10 subjects in the active treatment group with the greatest improvement in KOOS-Pain score at 3 months (“responders”) and in the 10 subjects in the active treatment group with the least improvement in KOOS-Pain score at 3 months (“nonresponders”). Additionally, bulk RNA sequencing of synovial cells in all 150 subjects will determine if genetic expression signatures, averaged over approximately 1000 cells, can predict changes in KOOS-Pain.
Methods
Trial Design
CoMeT is a 3-center (Cleveland Clinic, Brigham and Women’s Hospital, and Vanderbilt University Medical Center) randomized trial to assess the clinical efficacy of extended-release triamcinolone injection immediately after APM. It is a superiority study with a design that features double blinding, parallel groups (1 sham/placebo control), and permuted blocks. The primary outcome is change in patient-reported pain at 3 months, with the secondary outcomes being the changes from baseline to 6 months and baseline to 12 months. Figure 1 depicts the flow of patients through the trial from recruitment to study completion, and Table 1 specifies the components of each scheduled examination. The protocol and trial design are written in accordance with the SPIRIT guidelines on clinical trials, 5 and the SPIRIT 33-item checklist is included as supplemental material. CoMeT is registered at clinicaltrials.gov (NCT04641351), and the study protocol has been approved by the institutional review boards (IRBs) of Cleveland Clinic, Massachusetts General/Brigham and Women’s Hospital, and Vanderbilt University Medical Center. The IRB-approved detailed protocol for the coordinating center (Cleveland Clinic) is available as supplemental material.

Flow diagram of participant enrollment, randomization, and follow-up. APM, arthroscopic partial meniscectomy; KOOS, Knee injury and Osteoarthritis Outcome Score; MRI, magnetic resonance imaging; REDCap, Research Electronic Data Capture.
Schedule of CoMeT Study Assessments a

a Blank cells indicate areas not applicable. CoMeT, Corticosteroid Meniscectomy Trial; KOOS, Knee injury and Osteoarthritis Outcome Score; MRI, magnetic resonance imaging.
Patient Sample
The target population for this trial is patients >40 years of age with meniscus tear and OA scheduled for APM. Subjects must meet all inclusion criteria and no exclusion criteria (Table 2). We plan to recruit 150 subjects to be randomized with equal probabilities to extended-release triamcinolone injection and saline injection. Enrollment commenced June 2021 at Cleveland Clinic and at other sites in 2022. Most inclusion and exclusion criteria are assessed before surgery, and subjects meeting all presurgical criteria will provide consent after being counseled by a CoMeT physician-investigator at Brigham and Women’s Hospital and a research coordinator at Cleveland Clinic and Vanderbilt. The consent form used at Cleveland Clinic is included as supplemental material. The recruiting surgeons will complete a Clinic Criteria Form for each potentially eligible patient before surgery, which is included as supplemental material. Final eligibility will ultimately be determined during the operation, before randomization. Subjects found ineligible during the operation will not be randomized and will not continue in the trial.
Trial Inclusion and Exclusion Criteria a

a APM, arthroscopic partial meniscectomy; MRI, magnetic resonance imaging; OA, osteoarthritis.
b Criterion assessed before and during surgery.
c Criterion assessed during surgery.
Participants will be recruited by participating surgeons at enrolling medical centers from patients already scheduled for APM procedures. The schedules of recruiting surgeons will be monitored weekly by research coordinators to allow all patients undergoing APM scheduled by participating physicians to be prescreened for exclusion criteria. In addition to the prespecified exclusion criteria listed in Table 2, patients may be excluded owing to abnormalities or medical conditions that, in the opinion of the investigator, could compromise patient safety or data quality, such as recent myocardial infarction, rheumatoid arthritis, psoriatic arthritis, subchondral insufficiency fracture, pigmented villonodular synovitis, or a large loose body in the joint that necessitates treatment above and beyond APM. Other exclusions include recent intra-articular injections of corticosteroids, hyaluronic acid, or platelet-rich plasma, as these medications may have long-lasting effects that can temporarily lower baseline pain levels and mask pain improvements attributed to triamcinolone or APM.
Randomization and Blinding Procedures
Final eligibility will be assessed in the operating room after diagnostic arthroscopy. Research Electronic Data Capture (REDCap) will be used to randomize eligible subjects 1:1 to the triamcinolone extended-release or saline treatment group in random permuted blocks of variable size, stratified by the presence or absence of reactive synovitis (inflammation of the synovial lining being a known contributor to symptoms and progression of knee OA 26 –29 ) as graded by the surgeon during the diagnostic arthroscopy.
This trial is double blind: subjects, investigators, and research staff otherwise interacting with the patient will not know the treatment administered. To ensure blinding and the delivery of the specified experimental treatment, a blinded research coordinator will provide a randomization code to an unblinded operating room circulating nurse or physician assistant to dispense the correct medication to the surgeon in the operating room. The circulating nurse will not be involved in any subsequent care or follow-up of the patient. The nurse will deliver the extended-release triamcinolone medication or saline to the surgeon in a foil-wrapped syringe to hide the identity of the injected agent. In preparing the saline placebo solution, this nurse will follow all procedures that would be necessary to prepare a triamcinolone injection. Thus, all clinicians, including the surgeon and research staff involved in postoperative care and assessment of outcomes, are blinded to treatment. The blind will be broken on completion of the clinical study and after the study database has been locked. If a patient has a serious adverse event (SAE) in the perioperative period or a postoperative reaction or dangerous side effect, the patient and the surgeon will be unblinded, if needed, to provide the patient with proper medical treatment. This decision will be reviewed with the principal investigator (PI) of the site. This is the only circumstance in which unblinding will occur.
Biospecimen Collection
Tissue samples and synovial fluid will be collected during the APM operation, and blood and urine samples will be collected throughout the study. The complete biospecimen-handling protocol is available as supplemental material; a summary is provided here.
Synovial Fluid Collection
On the day of surgery, after induction of general anesthesia and before the start of the APM procedure, the surgical knee will be aspirated, and an 18-gauge needle and a 10-mL syringe will be used to collect as much synovial fluid as possible. If <1 mL of synovial fluid is collected in this manner, joint lavage may be performed with 5 mL of preservative-free saline solution injected into the knee joint and withdrawn.
Synovial Tissue Biopsy
Synovial tissue (approximately 500 mm3) will be collected intraoperatively from the surgical knee. The surgeon will use a pituitary rongeur inserted through an arthroscopic portal to retrieve the tissue from the area judged visually to have the most severe synovitis. Specimens will be divided into 2 portions: 1 for histology (approximately 100 mm3) and 1 for RNA sequencing (approximately 400 mm3). Biopsies for histology will be stored in 10% neutral-buffered formalin for 24 hours at room temperature and then transferred to 70% ethanol and stored at room temperature. Biopsies for RNA sequencing will be cooled at a rate of –1°C per minute for a minimum of 24 hours and then transferred to liquid nitrogen as soon as possible. Samples will be stored in a liquid nitrogen freezer until analysis.
Blood and Urine Collection
A minimum of 1.2 mL of serum and a minimum of 200 µL of urine will be collected at the time of surgery and at each of the 3- and 12-month visits (Table 1).
Intervention
Participants will be randomized to receive either 32 mg of FX006 (extended-release triamcinolone acetonide; brand name Zilretta [Pacira BioSciences]) in a 5-mL intra-articular injection or saline placebo in a 5-mL intra-articular injection at the conclusion of APM surgery. FX006 is formulated as 75:25 polylactic-co-glycolic acid microspheres and triamcinolone acetonide powder reconstituted as an isotonic, sterile, aqueous solution of sodium chloride, carboxymethylcellulose sodium, and polysorbate 80. The protocol for preparing the study boxes that contain Zilretta or saline placebo is included as supplemental material. For further information on FX006, see https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/208845s000lbl.pdf.
After delivery of the saline or triamcinolone injection, all subjects will remain on their prior medications with no new chronic knee pain-related therapies added as part of the trial. Subjects will be administered standard post-APM pain control therapies consisting of (1) nonsteroidal anti-inflammatory drugs as needed for pain control; (2) narcotic pain medication as needed for 14 days postsurgery; and (3) postoperative physical therapy following the standardized, 3-stage, progressive 8- to 12-week protocol used in the MeTeOR Trial (Meniscus Tear and Osteoarthritis Research). 12
Prohibited medications for the duration of the 3-month postoperative period include (1) intra-articular injection of any agent and (2) narcotic pain medication after the initial 14 days postsurgery. Other concomitant medications are allowed, and all relevant details of concomitant medications and therapies (dose, route, frequency, indication for administration, etc) will be documented at screening and at 3-month follow-up.
Imaging Protocol
The MRI scans will be collected at baseline, 3-month, and 1-year visits using 3-T magnetic resonance systems (Skyra-fit, Prisma, or Verio [Siemens Healthcare AG]; Ingenia Philips Healthcare) with a transmit/receive knee coil (1Tx/15Rx, QED; 1Tx/16Rx, Philips; 1Tx/8Rx Verio). The scan protocol includes morphologic 2-dimensional TSE scans for clinical evaluations, 3D TSE images (SPACE on Siemens and VISTA on Philips), 3D dual echo steady state (DESS) scans, and T1ρ and T2 scans based on 3D magnetization-prepared angle-modulated partitioned k-space spoiled gradient echo snapshots (MAPSS) for quantitative cartilage evaluation. 14,18 Table 3 details the specific MRI protocols.
Fixed flexion radiographs will be performed at baseline and 12 months using the Synaflexer positioning device (Synarc Inc) to ensure consistent positioning for measurement of joint space width changes over time. 15
Magnetic Resonance Imaging Scan Protocol Parameters a

a 3D, 3-dimensional; DESS, double echo steady state; MAPSS, magnetization-prepared angle-modulated partitioned k-space spoiled gradient echo snapshots; NA, not applicable; PD, proton density; TE, time to echo; TR, repetition time; TSE, turbo spin echo.
b Shared parameters: field of view = 140 × 140 mm3, fat suppression for all images except T1 TSE coronal and 3D TSE.
c Other parameters for MAPSS: spin-lock frequency = 500 Hz, T1 recovery time = 1.5 seconds, views per segment = 92. Time of spin lock = 0, 10, 30, 70 milliseconds. T2 preparation TE = 0, 20.06, 40.13, 60.19 milliseconds.
Follow-up Procedures
Evaluations conducted at baseline (prerandomization) and 3, 6, and 12 months after randomization will include PROs, urine and serum samples, synovial tissue biopsies, synovial fluid, fixed flexion radiographs, and MRI (Table 1). Questionnaires filled at all time points will be sent via email through secure REDCap links. To encourage attendance at follow-up visits, the research coordinators will call participants the day before their 3- and 12-month visits to remind them of their appointments and to ensure that the questionnaire is complete. Any questionnaires not completed ahead of the study visit will be collected on the day of the visit.
At the 6-month time point, participants will receive reminder calls to complete their questionnaires. Participants will be compensated by checks for US $50 for the 3-month visit and US $75 for the 12-month visit for a total of US $125. Participants will also be given parking vouchers if parking is not free at the site.
Data Management
Cleveland Clinic will provide central data coordination and management. All data will be entered by study personnel from source documents corresponding to a subject’s visit into a common electronic case report form (CRF) stored in a studywide REDCap database developed and maintained by Cleveland Clinic. Deidentified images will be uploaded from all sites to a centralized, secure Cleveland Clinic Picture Archiving and Communication System. The site PIs will be responsible for all information collected on subjects in the study and will review the data collected during the study for accuracy and completeness. To further ensure data quality, a data analytic and management group—including the project lead statistician, database manager, and lead imaging scientist—will regularly review the REDCap data for quality assurance and audits. A standard folder of hard copy CRFs, informed consent, and other study documents will be kept for each subject, as required for all clinical studies at each institution. If corrections are required for a hard copy CRF, the corresponding electronic form will be updated at that time with an electronic audit trail. The funding agency (Arthritis Foundation) will receive annual progress reports, financial reports, and IRB approvals and renewals. Pacira BioSciences will provide Zilretta free of charge, and additional funds from Pacira will be allocated to support collection, storage, and analysis of biospecimens. Pacira will review summary monthly updates, including the total enrollment number, adverse events (AEs), and significant changes to the protocol but not treatment-specific information.
To protect patient confidentiality, access to the encrypted and password-protected servers and database will be restricted to IRB-approved study personnel, whose interactions with the database are controlled by task-specific permissions that allow only such interactions as necessary to perform assigned study duties. These measures protect enrolled patients and potentially eligible patients who provide data during screening but are not ultimately enrolled. All study documents will be stored securely for at least 6 years after study completion and 2 years after initial marketing of the investigational product or, if this does not occur, 2 years after centers are notified that the investigational product has been discontinued without marketing. Only the investigators will have access to the final trial data set, but requests for access to trial data will be considered on a case-by-case basis by the Executive Committee, including the study PI and site PIs, without requiring approval from the Arthritis Foundation or Pacira BioSciences. Authorship for all future publications will be determined per criteria of the International Committee of Medical Journal Editors. The Executive Committee will review all publications and make publication decisions independent of the Arthritis Foundation and Pacira BioSciences.
Study Outcomes
Outcomes captured for each objective are outlined in Table 4 and described here.
Outcome Measures Associated With Study Objectives a
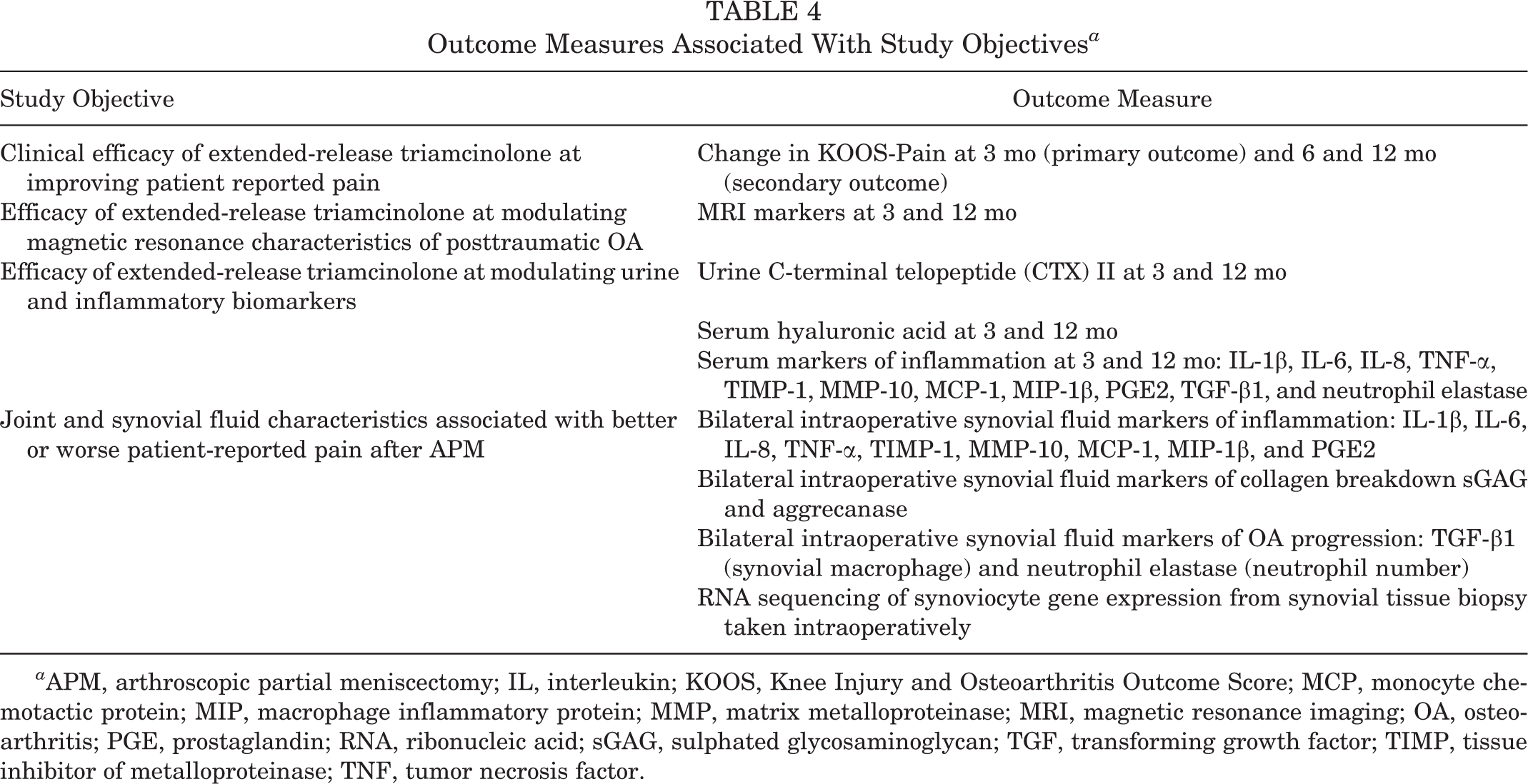
a APM, arthroscopic partial meniscectomy; IL, interleukin; KOOS, Knee Injury and Osteoarthritis Outcome Score; MCP, monocyte chemotactic protein; MIP, macrophage inflammatory protein; MMP, matrix metalloproteinase; MRI, magnetic resonance imaging; OA, osteoarthritis; PGE, prostaglandin; RNA, ribonucleic acid; sGAG, sulphated glycosaminoglycan; TGF, transforming growth factor; TIMP, tissue inhibitor of metalloproteinase; TNF, tumor necrosis factor.
Primary Outcome
The primary objective of this project is to test the clinical efficacy of intra-articular extended-release triamcinolone administration at the end of APM for improving patient pain, operationalized as change in KOOS-Pain score from baseline to 3 months post-APM. This endpoint was selected as the most clinically relevant since APM is performed to improve pain.
Secondary Outcomes
Secondary objectives include the following:
Using single-cell RNA sequencing to understand the relationships between synovial inflammation and PROs
Testing the efficacy of intra-articular extended-release triamcinolone administration for improving patient KOOS-Pain at 6 and 12 months post-APM
Testing the efficacy of intra-articular extended-release triamcinolone administration for improving magnetic resonance characteristics of the knee associated with posttraumatic OA (PTOA)—specifically, MRI Osteoarthritis Knee Score (MOAKS), high-resolution 3D morphologic sequences for cartilage and bone segmentation and bone shape modeling, and quantitative T1ρ and T2 mapping sequences for cartilage and meniscal composition—evaluated for changes from baseline to 3 and 12 months post-APM (for details of the MRI protocol, see Table 3)
Testing the effect of intra-articular extended-release triamcinolone on the rate of radiographic joint space loss from baseline to 12 months post-APM
Testing the efficacy of intra-articular extended-release triamcinolone administration for improving urine and serum biomarker profiles associated with PTOA and inflammation from baseline to 3 and 12 months post-APM (Table 4)
Assessing baseline joint fluid and synovial tissue characteristics predictive of better or worse PROs 3 and 12 months after APM, using RNA sequencing to explore cell populations of inflamed synovial tissue as well as genetic markers of inflammation in these cells
Statistical Analyses
Since eligibility is ultimately determined intraoperatively before randomization and the treatment consists of a single blinded injection immediately after the patient’s APM surgery, the only opportunity for a departure from the randomized treatment would be an operational error by the research coordinator or circulating nurse during the selection and administration of the intervention. In the unlikely case of 1 or more such events, analyses of efficacy endpoints will follow the intention-to-treat approach, and analyses of safety endpoints will follow the as-treated approach. No interim analyses are planned. Analytic approaches for KOOS-Pain scores, magnetic resonance characteristics, and biomarker profiles are described in turn.
KOOS-Pain Score
Changes in KOOS-Pain scores will be compared between treatment arms within a single mixed linear analysis of covariance model for the dependence of change score on a random Gaussian patient effect and on fixed effects of 4 variables (baseline KOOS-Pain score and postoperative intervals [3, 6, and 12 months]), their interaction, and the treatment arm (triamcinolone or placebo) nested within a follow-up interval. Residual variability will itself be allowed to vary among 3-, 6-, and 12-month intervals initially, but an equivariance model will be utilized unless variance inequality reaches conventional statistical significance. Formal statistical inference will be based on restricted maximum likelihood and associated Wald tests and confidence intervals.
If significant treatment benefit is observed at 3 months, we will fit additional models to separately explore potential modification of the treatment effect by smoking status and sex, as well as linear effects of baseline KOOS-Pain, age, and body mass index. If significant treatment benefit at 12 months is confirmed, we will proceed similarly. Regardless of overall outcome, we will conduct a subgroup analysis by presence or absence of baseline reactive synovitis and examine the interaction of treatment effect with this stratification variable.
Data loss—unless it is well below 10% and primary results are clearly unequivocal—will be addressed before the modeling process by fully conditional multiple imputation (n = 20). Sensitivity of primary and secondary results will be checked against a missing-at-random assumption using basic pattern-mixture and possibly selection models.
MRI Results
Mixed models will be used as for the KOOS-Pain analysis. Inasmuch as triamcinolone benefit on these outcomes may be expected to take longer to manifest than pain benefit, 12-month measurements will be considered primary and 3-month measurements considered exploratory for MRI results.
Biomarkers of Inflammation and Tissue Degradation
Biomarker results will be analyzed on 3 levels. We will first describe their cross-sectional associations with KOOS-Pain score using Pearson or Spearman correlation coefficients, depending on the distributions of these variables, and then examine the effects of triamcinolone injection on 3- and 12-month changes in biomarkers using mixed effects regression models analogous to those for KOOS-Pain score and MRI markers. Then we will examine the extent to which baseline biomarker levels may modify the triamcinolone treatment effects on longitudinal changes in outcomes by augmenting prior models for outcomes with the main effect and interaction of each biomarker with treatment. In each of these 3 sets of analyses, we will control the false discovery rate at <10% for each outcome and time interval by adjusting the P values for testing multiple biomarkers using the method of Benjamini and Yekutieli. 2
Sample Size and Statistical Power
A simplified power analysis of the test of primary outcome was performed via a 2-sample t test (2-sided, 5% level) comparing changes in KOOS-Pain score across treatments based on the following assumptions and sources:
A standard deviation of change of 18.58 points—from the 6-month confidence interval of the MeTeOR Trial, 12 increased by 7% to protect against underestimation from variability of that study’s observed standard deviation
An 11.4% reduction in residual standard deviation from covariate control for baseline pain score—from analysis of 486 consecutive patients aged ≥40 years and with 12-month post-APM follow-up available during planning from Cleveland Clinic’s prospective OME cohort (Orthopaedic Minimal Data Set Episode of Care) 21
A 15% dropout and complete case analysis, neglecting recovered information from multiple imputation
Under these assumptions, the trial will have 80% power against an 8.1-point treatment difference and 85%, 90%, and 95% power against differences of 8.7, 9.4, and 10.5 points, respectively. These results presume similar variability of 3- and 6-month KOOS-Pain score changes and that baseline KOOS-Pain explains similar fractions of variation of its 3- and 12-month changes. The minimum clinically important difference in KOOS-Pain score is thought to be 8 to 10 points, 24 suggesting that CoMeT is appropriately powered to detect clinically significant treatment benefit.
AEs and Participant Safety
AEs are defined as any untoward medical occurrences temporally associated with the use of the experimental intervention in a participant, whether or not considered intervention related. AEs may be expected or unexpected. AEs may be also be classified as SAEs. CoMeT AE and SAE definitions follow the guidelines of the US Health and Human Services Office for Human Research Protections as recommended by the US National Institutes of Health. 20
Assessment for causal relationship with the intervention will be done by a medically qualified investigator for every AE and SAE. An unexpected AE is one of a type not identified in the package insert of the experimental intervention (extended-release triamcinolone; Zilretta). When an AE occurs, it will (1) be classified by severity (mild, moderate, or severe) and seriousness (based on meeting any of the US Food and Drug Administration’s 7 reporting criteria: death, life-threatening, hospitalization, disability, congenital anomaly/birth defect, required intervention to protect patient, or other important medical event) and (2) be assessed for causal relationship with the intervention. AEs will be judged not related to the study medication if not reasonably temporally proximal to its administration OR if other causative factors related to the subject’s health, such as a preexisting condition or concomitant treatment, are more likely to explain the event. AEs will be judged as related to the study intervention if there is a short-term temporal relationship with the study medication administration AND the AE is more likely explained by the investigational product than by another cause.
AEs will be collected from the time of intra-articular injection of placebo or triamcinolone through the completion of the participant’s time in the study (14 months postrandomization or early discontinuation). The site PI will determine if an AE has occurred, subject to review by the study PI. The site PI will be responsible for reporting SAEs to the local IRB within 10 days of discovery/awareness. The overall study PI will be responsible for reporting SAEs (1) to Pacira BioSciences within 10 calendar days when occurring in a patient treated with the experimental extended-release triamcinolone and (2) to the US Food and Drug Administration per 21 CFR 314.80. The investigator will probe for AEs during discussions with the participant at each study visit (Table 1). AEs will be described and recorded by duration, outcome, and treatment in addition to the classifications indicated here but not described by treatment in reports to Pacira BioSciences until the end of the study.
Discussion
Postoperative outcomes after APM are variable, 17 and inflammatory processes have been suggested to contribute to the symptoms, disease progression, and overall variable outcomes of APM. 13,19,27,32 Reduced postoperative inflammation resulting from administration of triamcinolone has been associated with improved outcomes in other knee pathologies, notably anterior cruciate ligament injury, 16,30 making it an attractive target in meniscal injury, but the clinical efficacy of triamcinolone post-APM has not been examined in a randomized controlled trial. Triamcinolone injections have been shown to decrease synovial tissue volume in knee OA, 22 and synovitis is hypothesized to be associated with symptomatic knee OA. Extended-release triamcinolone, in particular, is a novel intervention with potential to address a proposed mediator of postoperative heterogeneous outcomes in patients undergoing APM. Although previous clinical trials 3,7,31 have tested the efficacy of extended-release triamcinolone in patients with knee OA, this agent has never been investigated in patients undergoing APM, and such an adjunctive intraoperative intervention might improve outcomes of some members of this patient population. CoMeT will evaluate the efficacy of extended-release triamcinolone (Zilretta) for improving patient-reported pain outcomes after APM and for preventing PTOA. When completed, CoMeT will provide insight into the clinical efficacy of post-APM triamcinolone and contribute to our understanding of the role that synovitis and inflammation play in APM outcomes and meniscal/OA disease processes.
To the best of our knowledge, this will be the first randomized double-blind clinical trial to assess the effect of extended-release triamcinolone acetonide on pain, MRI measures of structural change and effusion/synovitis, soluble biomarkers, and synovial tissues transcriptomics. The collection of intra-articular samples with serum and urine biomarkers presents a unique opportunity to evaluate not only the clinical efficacy of extended-release triamcinolone but also the role of synovitis and inflammation of the knee joint in the pathogenesis of PTOA after APM. In particular, single-cell RNA sequencing of synovial tissue cells will provide insight into molecular and cellular features of the synovium in patients with OA and meniscal tear. High-dimensional analyses will elucidate if determinants of response to triamcinolone exist at the transcriptional level. Previous research has utilized these high-dimensional analyses to understand the heterogeneity of synovial cell types in patients with knee OA. Huang et al 11 identified 7 distinct cell types in OA synovial tissues from bulk RNA sequencing data, and Zhou et al 33 used single-cell RNA sequencing to compare gene expression profiles of macrophages in healthy knees as compared with OA knees. Relating these cell types and genetic markers to PROs and comparing cell types and markers between selected subjects who do and do not respond to treatment are innovative features of our trial design, the findings of which could inform future treatment options for patients with mild to moderate OA and meniscal tear, regardless of their decision to undergo APM.
Beyond biological samples, the 3D MAPSS acquisition for T1ρ and T2 cartilage measurements has been shown to be sensitive to OA disease progression and has proven to have good reproducibility across multiple imaging sites. 14 Thus, this trial will investigate the value of this imaging technique for determining the relationship between cartilage imaging biomarkers, as well as the effect of extended-release triamcinolone on PROs and biological biomarker outcomes specifically and the association with PTOA more generally.
Limitations
Several limitations of the trial design must be recognized. Noncontrast MRI is inferior to contrast-enhanced MRI for detecting and grading synovitis severity. 4 We have chosen to utilize noncontrast MRI as the trial’s imaging modality to aid in subject recruitment, as patients may be less inclined to participate in an MRI study that requires an intravenous injection. Trial participants will be advised to avoid use of intra-articular injections or narcotics for postoperative swelling and discomfort for 3 months after randomization (until the primary outcome is obtained), which would limit the efficacy of APM typically observed in clinical practice. As the largest effect of triamcinolone is hypothesized to be in patients with synovitis, it is possible that patients without substantial synovitis will have similar outcomes to those who receive saline. To minimize potential confounding in this situation, we will stratify randomization by the presence or absence of reactive synovitis. Nevertheless, if a substantial treatment effect is confined to the subgroup of patients with baseline reactive synovitis, the study power will be considerably reduced. Last, the exclusion criteria selected for CoMeT may limit applicability of the findings to the general population, particularly with respect to participation in physical therapy and pain post-APM (eg, bilateral surgery, recent intra-articular injection, and Kellgren-Lawrence grade IV OA).
Conclusion
The combination of molecular, structural, and PROs will allow analyses that further our understanding of the response to triamcinolone after APM, as well as the role of inflammation in PTOA disease progression without the injection of triamcinolone. Thus, this study will provide high-quality randomized trial evidence that can advance the knowledge of PTOA development with a specific focus on synovitis. The evaluation of extended-release triamcinolone injection after APM through patient-reported pain, molecular biomarkers, and structural evaluation has the potential to increase our understanding of the underlying mechanisms of OA progression after APM and OA progression more generally.
Supplemental Material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671221150812#supplementary-materials.
Supplemental Material
Supplemental Material, sj-zip-1-ojs-10.1177_23259671231150812 - The Corticosteroid Meniscectomy Trial of Extended-Release Triamcinolone Injection After Arthroscopic Partial Meniscectomy: Protocol for a Double-Blind Randomized Controlled Trial
Supplemental Material, sj-zip-1-ojs-10.1177_23259671231150812 for The Corticosteroid Meniscectomy Trial of Extended-Release Triamcinolone Injection After Arthroscopic Partial Meniscectomy: Protocol for a Double-Blind Randomized Controlled Trial by James K. Sullivan, Julia R. Gottreich, Peter B. Imrey, Carl S. Winalski, Xiaojuan Li, Kurt P. Spindler, Patrick M. Tomko, Charles L. Cox, Rick W. Wright and Morgan H. Jones in Orthopaedic Journal of Sports Medicine
Footnotes
Correction June 2024:
Laura J. Huston, MS has been added to the author list.
Final revision submitted September 22, 2022; accepted October 21, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: All study-related activities are supported by the Arthritis Foundation, with the exception that Pacira BioSciences will provide the necessary doses of extended-release triamcinolone (Zilretta) to all 3 study sites and will support collection and analysis of biospecimens. C.S.W. has received consulting fees from Siemens Medical. K.P.S. has received consulting fees and honoraria from Flexion Therapeutics. R.W.W. has received royalties from Responsive Arthroscopy. M.H.J. has received consulting fees from Regeneron. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cleveland Clinic (No. 20-1074).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.