
Abstract
Background:
It remains unclear if femoral retroversion is a contraindication for hip arthroscopy in patients with femoroacetabular impingement (FAI).
Purpose:
To compare the area and location of hip impingement at maximal flexion and during the FADIR test (flexion, adduction, internal rotation) in FAI hips with femoral retroversion, hips with decreased combined version, and asymptomatic controls.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Twenty-four symptomatic patients (37 hips) with anterior FAI were evaluated. All patients had femoral version (FV) <5° according to the Murphy method. Two subgroups were analyzed: 13 hips with absolute femoral retroversion (FV <0°) and 29 hips with decreased combined version (McKibbin index <20°). All patients were symptomatic and had anterior groin pain and a positive anterior impingement test ; all had undergone pelvic computed tomography (CT) scans to measure FV. The asymptomatic control group consisted of 26 hips. Dynamic impingement simulation of maximal flexion and FADIR test at 90° of flexion was performed with patient-specific CT-based 3-dimensional models. Extra- or intra-articular hip impingement area and location were compared between the subgroups and with control hips using nonparametric tests.
Results:
Impingement area was significantly larger for hips with decreased combined version (<20°) versus combined version (≥20°) (mean ± SD; 171 ± 140 vs 78 ± 55 mm2; P = .012) and was significantly larger for hips with FV <0° (absolute femoral retroversion) vs FV >0° (P = .025). Hips with absolute femoral retroversion had a significantly higher frequency of extra-articular subspine impingement versus controls (92% vs 0%; P < .001), compared to 84% of patients with decreased combined version. Intra-articular femoral impingement location was most often (95%) anterosuperior and anterior (2-3 o’clock). Anteroinferior femoral impingement location was significantly different at maximal flexion (anteroinferior [4-5 o’clock]) versus the FADIR test (anterosuperior and anterior [2-3 o’clock]) (P < .001).
Conclusion:
Patients with absolute femoral retroversion (FV <0°) had a larger hip impingement area, and most exhibited extra-articular subspine impingement. Preoperative FV assessment with advanced imaging (CT/magnetic resonance imaging) could help to identify these patients (without 3-dimensional modeling). Femoral impingement was located anteroinferiorly at maximal flexion and anterosuperiorly and anteriorly during the FADIR test.
Keywords
Patients with femoral retroversion present with decreased internal rotation (IR) and with anterior hip pain attributed to femoroacetabular impingement (FAI). 8,19 Femoral retroversion can lead to extra-articular contact between the proximal femur and the anterior inferior iliac spine (AIIS) in patients undergoing total hip arthroplasty (THA). 44 Previous studies have noted that a cam-type deformity typically reduces IR of the hip, usually assessed at 90° of flexion. 12,51 Femoral retroversion also decreases IR and thus theoretically can outweigh the effect of a cam deformity for IR. 8,19,53 Before the description of FAI, Tönnis and Heinecke 53 investigated femoral version (FV) and acetabular version and its variance and cited normal FV and acetabular version between 10° and 25°. Femoral retroversion was investigated by them almost 30 years ago, and it was called “diminished femoral antetorsion syndrome,” 54 when they observed that patients with hip pain and early signs of osteoarthritis had femoral retroversion and exhibited decreased IR of the hip joint. 53,54 By then, treatment with derotation osteotomy to correct femoral retroversion (proximal femoral osteotomy) was performed in adult patients 54 ; however, there was no detailed follow-up. More recently, good clinical results after proximal femoral derotation osteotomy have been reported for adult patients. 6 In adolescent patients with femoral retroversion, successful treatment with rotational osteotomy was also found. 16,54
Surgical treatment of patients with FAI was initially performed with open hip preservation surgery or with hip arthroscopy for cam resection and/or acetabular rim trimming and later labral treatment, without detailed consideration of FV or femoral retroversion. 12,33 In 2015, the effect of FV was investigated for patients who underwent hip arthroscopy, 10 but only a few studies 13,19 have investigated the effect of femoral retroversion thereafter. However, it has been shown that increased and decreased FV can significantly impair patient-related outcomes after hip arthroscopy for patients with FAI. 10 Decreased FV has been associated with revision surgery after hip arthroscopy at 2-year follow-up, 36 and femoral retroversion (defined as FV <5°) has been associated with anterosuperior and subspine hip impingement 24 in patients with FAI. Subspine impingement was reported when the AIIS caused bony impingement contact with the proximal femur. 24
Abnormalities in FV are becoming increasingly recognized as important factors regarding treatment of patients with FAI. 26,43 To date, treatment of patients with FAI with femoral retroversion remains controversial because there is conflicting evidence on whether FV affects clinical outcomes after hip arthroscopy for FAI. 17 Excessive femoral retroversion was considered a relative contraindication to FAI surgery by others 53 because of poor outcomes after hip arthroscopy for FAI. 10 In a recent systematic review evaluating whether FV influences the outcome of hip arthroscopy, the authors reported that patients with normal FV and patients with femoral retroversion (defined as FV <5°) exhibited similar failure rates but significantly different scores on the Non-arthritic Hip Score and the Hip Outcome Score–Sport Specific Subscale. 55
Decreased FV was associated with anterosuperior intra- and extra-articular subspine hip impingement in a recent study analyzing impingement conflict using 3-dimensional computed tomography (3D-CT). 24 But impingement conflict in maximal flexion without rotation was not analyzed. So far, the location of extra- or intra-articular hip impingement in flexion in patients with absolute femoral retroversion is unknown. In addition, it is unclear if these patients could be identified without time-consuming 3D modeling and 3D-CT scanning.
The purpose of the current study was to compare the area and location of hip impingement in maximal flexion and during the FADIR test (flexion, adduction, internal rotation) in patients with FAI with absolute femoral retroversion versus those with decreased combined version. The hypothesis was that patients with absolute femoral retroversion will have a larger impingement area.
Methods
The protocol for this study received institutional review board approval, and all participants provided informed consent. We conducted a retrospective analysis of 24 symptomatic patients (37 hips) with anterior FAI who were seen at our outpatient clinic between January 2014 and December 2016. The patients were part of a previous study. 24 Inclusion criteria were FV <5° on CT scan (termed decreased FV) and the absence of hip dysplasia. Exclusion criteria were a lateral center-edge angle 49 <22° or an acetabular index 53 >14° and Tönnis grade ≥1 osteoarthritis. 52 All patients had undergone standardized anteroposterior and lateral radiographs as well as CT scans including the entire pelvis and the knee joint (distal femoral condyles) 34,35 according to a previously described protocol. 24,42 At the time of imaging, all patients were symptomatic and had anterior groin pain, a positive FADIR test result (performed at 90° of flexion and forced IR), and decreased IR during clinical examination. Some patients also reported hip pain at maximal flexion.
Considerable differences for FV measurement exist. 42 In the current study, we measured FV on standardized pelvic CT scans using the method of Murphy et al. 30 This method has small interobserver variability. 26,42 The hips with decreased FV were categorized into those with absolute femoral retroversion (FV <0°) and those with decreased combined version (McKibbin index 22 <20°). Definitions of the terms used in this study are listed in Table 1.
Definitions of Terms Used a

a FAI, femoroacetabular impingement; LCEA, lateral center-edge angle.
b Patients with hip dysplasia were excluded from the study.
Of the 37 hips with decreased FV, 16 (43%) had cam deformity, 7 (19%) had pincer-type deformity, 6 (16%) had combined cam and pincer deformity (mixed-type FAI), and 8 (22%) had neither cam- nor pincer-type morphology. There were 13 hips with absolute femoral retroversion (Figure 1) and 29 hips with decreased combined version (Table 2); the 2 subgroups could overlap, and some of the hips were part of both groups. Most of the 24 study patients were male (62%), with a mean ± SD age of 28 ± 9 years and FV of 1° ± 4°.

(A) A 3-dimensional model of the bilateral femur and (B, C) axial computed tomography images of the hip and posterior femoral condyle in a 26-year-old man with absolute femoral retroversion. (B) The femoral head center (white dot) was connected with the center of the femoral shaft on the level of the lesser trochanter to define the proximal landmarks. (C) The posterior condyles were connected with a line for the distal landmarks.
Demographic Characteristics and Imaging Information of the Study Patients a

a Data are reported as mean ± SD (range) or percentage.
b Patients: N = 24.
In addition to the study groups, we included a control group of 26 unaffected hips from the contralateral side of 146 patients who had undergone THA. The mean age of the control group was 54 ± 11 years. Exclusion criteria for the control group were as follows: THA or total knee arthroplasty (n = 10), pain (n = 4), previous hip surgery (n = 3), Tönnis grade ≥1 osteoarthritis 52 (n = 40), lateral center-edge angle <25° (n = 24), pistol grip deformity 48 (n = 13), coxa profunda (n = 13), coxa vara or valga (n = 1), acetabular retroversion 40,51 (n = 4), protrusio acetabuli (n = 2), alpha angle >50° (n = 4), and femoral retroversion (n = 2).
Imaging
Acetabular version was calculated on axial CT scans on the level of the femoral head center 14 (3-o’clock version). Morphology of the AIIS was evaluated using 3D models of the pelvis according to a published classification system 15 by 2 independent observers with 5 years of experience in musculoskeletal radiology. To build patient-specific 3D bone models of the pelvis and the femur, we performed bone segmentation using the Amira Visualization Toolkit (Visage Imaging Inc). The acetabular reference coordinate system was the anterior pelvic plane, defined by both anterosuperior iliac spines and the pubic tubercles. 24,50 The femoral reference coordinate system was defined by the center of the femoral head, the knee center, and both femoral condyles. 30 Using this 3D model generated from the CT scans, we compared the patient-specific impingement-free range of motion (ROM) and the individual acetabular and femoral impingement location of the patients.
Using personalized CT-based 3D models and software for collision detection (HipMotion; University of Bern), we evaluated all hips with the equidistant method. The software that we used has the features listed in Table 3. The equidistant method was designed for virtual FAI analysis. 35 Based on a cadaveric investigation including cartilage, labrum, and joint capsule, an impingement collision can be detected with a mean accuracy of 2.6° ± 2.5°. 35 Using this computerized analysis, we calculated the ROM for all 3 groups: flexion, extension, IR, and external rotation (at 0° and 90° of flexion). In a validation study of this software, intra- and interobserver measurements for the aforementioned ROM parameters were excellent (ICC>0.9) for the most important motions (maximal flexion and IR at 90° of flexion). 29
Details of the Collision Detection Software Based on 3-Dimensional Models of the Hip Joint

Furthermore, we evaluated 3 motion patterns that corresponded to the FADIR test for anterior impingement. 7,38,39 The impingement location was studied during the FADIR test at 90° of flexion; 30° of IR; and 0°, 10°, and 20° of adduction (Figure 2).
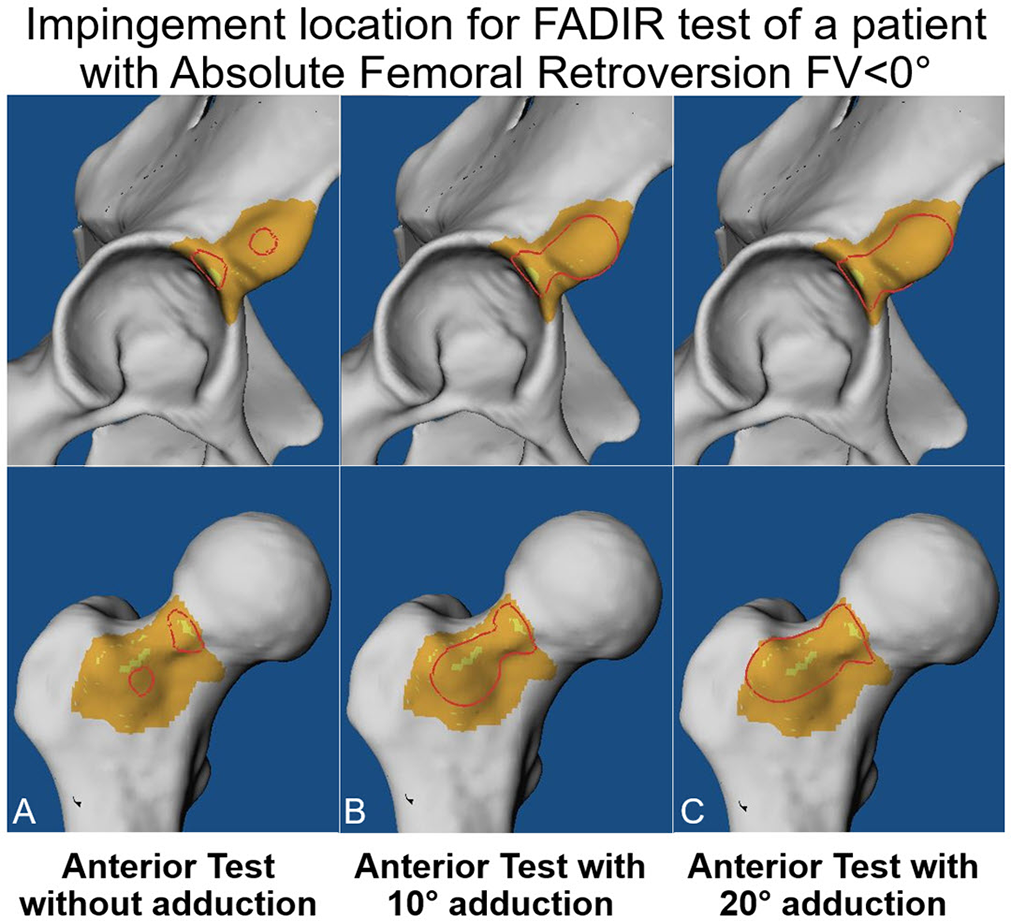
Determining the location of acetabular (top row) and femoral (bottom row) hip impingement during the FADIR test at 90° of flexion and 30° of internal rotation combined with (A) 0°, (B) 10°, and (C) 20° of adduction on computed tomography scans from a 23-year-old man with absolute femoral retroversion. The impingement area is outlined in red. FADIR, flexion, adduction, internal rotation.
The femoral location of impingement was compared between the FADIR test (90° of flexion and 30° of IR) and maximal flexion (no hip rotation). Impingement area was calculated using specific software (HipMotion). Evaluation of impingement area was performed via standardized views of the proximal femur and the acetabulum by 2 observers (T.D.L. and T.A.) using a brush tool to mark the area with bone-to-bone contact. Acetabular and femoral impingement area were calculated separately.
Statistical Analysis
Statistical analysis was performed using WinSTAT software (R. Fitch Software). The data were assessed for normal distribution with the Kolmogorov-Smirnov test. Because not all the parameters were normally distributed, we used nonparametric tests for comparison. To compare demographic and radiographic data, ROM, or location of impingement, we used the Mann-Whitney U test. To compare binominal demographic data and the prevalence of impingement, we used the Fisher exact test to compare the subgroups. Bonferroni correction was applied owing to multiple comparisons (4 groups, correction: 0.05/4 = 0.0125). Because of the applied correction, P < .0125 was considered the threshold for significance to avoid false-positive results. Impingement area, location, and frequency were compared between the subgroups and with control group.
Results
Almost half (49%) of the 37 hips with decreased FV underwent surgical treatment at the time of data collection. Surgical treatment included hip arthroscopy with femoral cam resection in 3 hips (8%), surgical hip dislocation with combined femoral cam resection and acetabular rim trimming in 5 hips (14%), and derotation proximal femoral osteotomies to increase FV in 10 hips (27%). Thirty percent of patients with decreased FV had type 1 AIIS morphology (11/37 hips, 30%), 70% (26/37 hips) had type 2, and none had type 3.
Impingement area was significantly larger in the hips with decreased combined version (<20°) versus the hips with combined version (≥20°) (171 ± 140 vs 78 ± 55 mm2; P = .012). Impingement area was slightly larger in hips of patients with FV <0° (absolute femoral retroversion) as compared with patients with FV >0° (189 ± 188 vs 132 ± 93 mm2; P = .025). During the FADIR test, the impingement area was slightly larger for the hips of patients with pincer-type FAI (382 ± 150 mm 2 ) or mixed-type FAI (411 ± 129 mm2) as compared with cam-type FAI (304 ± 284 mm2), and the impingement area increased during the FADIR test from 0° of adduction (135 ± 133 mm2) to 10° (232 ± 180 mm2) and 20° (340 ± 218 mm2).
During the FADIR test, hips with decreased FV had a significantly higher frequency of extra-articular subspine impingement as compared with control hips at 20° of adduction (84% vs 0%; P < .001). Hips with absolute femoral retroversion had a significantly higher frequency of extra-articular subspine impingement as compared with controls at 20° of adduction (92% vs 0%; P < .001) (Figure 3), while 84% of patients with decreased combined version had extra-articular subspine impingement (Table 4).

Frequency of extra-articular subspine hip impingement for patients with absolute femoral retroversion during the FADIR test: 90° of flexion; 30° of internal rotation (IR); and 0°, 10°, or 20° of adduction. FADIR, flexion, adduction, internal rotation.
Prevalence of Intra- and Extra-articular Subspine Impingement During the FADIR Test at 0°, 10°, or 20° of Adduction a

a Data are presented as percentages. FADIR, flexion, adduction, internal rotation.
Anteroinferior femoral impingement location was significantly different in maximal flexion (anteroinferior [4-5 o’clock]) versus the FADIR test (anterosuperior and anterior [2-3 o’clock]; P < .001) (Figure 4).

A clockface system was used for intra-articular impingement location, where 1 to 2 o’clock represents anterosuperior, 4 to 5 o’clock represents anteroinferior, and 3 o’clock anterior (for left and right hips). The anterior femoral impingement location was significantly different at maximal flexion (anteroinferior; 4-5 o’clock) vs during the FADIR test (anterosuperior and anterior; 2-3 o’clock) (P < .001). FADIR, flexion, adduction, internal rotation.
Intra-articular femoral impingement was most often (95%) anterosuperior and anterior (2-3 o’clock), and it extended to anterolateral, including the proximal femoral tubercle (tuberculum tertius) in one-third of hips (32%) during the FADIR test. Acetabular intra-articular impingement was located anterosuperior (1-2 o’clock) for maximal flexion and the FADIR test.
Discussion
Most important, a significantly larger impingement area was found for hips of patients with combined version <20° versus ≥20° (171 ± 140 vs 78 ± 55 mm2; P = .012). Analyzing the frequency of extra-articular subspine impingement, a significantly higher frequency was identified for hips with absolute femoral retroversion as compared with control hips (92% vs 0%; P < .001).
FAI is a known cause for hip pain and a precursor to hip osteoarthritis in young patients. 12 Hip arthroscopy is increasingly being used for treatment of FAI; a tremendous increase in hip arthroscopy to treat FAI (>4-fold) was noted between 2005 and 2013. 28 While use of hip arthroscopy for treatment of FAI continues to rise, there is no international consensus for the indications for this procedure. Excessive femoral retroversion is regarded as a contraindication for hip arthroscopy for some hip surgeons, 10 while others have reported good patient-reported outcomes after hip arthroscopy for patients with femoral retroversion 17 and have found no difference in outcomes as compared with patients with normal FV. 13
Direct comparison studies are challenging, and the biomechanical effects of hip impingement for these hips are not yet fully understood. In the current study, patients with absolute femoral retroversion had a significantly higher rate (92%) of anterior extra-articular subspine impingement as compared with control hips (0%; P < .001). In addition, we found that patients with decreased combined version (<20°) exhibited a significantly larger impingement area as compared with patients with combined version (≥20°; P = .012). To our knowledge, no other study has investigated the biomechanical effects of decreased combined version.
The literature remains sparse regarding patients with FAI with femoral retroversion, and different definitions of femoral retroversion exist. 55 Some authors have defined it using FV <5°, 10,11 FV <10°, 26 or FV <–2°. 17 Different measurement methods for FV have been used, and FV has been measured on oblique axial CT or magnetic resonance imaging (MRI). 10,17 These inconsistencies make it difficult to compare our results with previous studies. Detailed assessment of hip impingement location in maximal flexion for hips with absolute femoral retroversion (FV <0°) is unclear. Therefore, we investigated impingement in maximal flexion in 2 subgroups, with 1 subgroup consisting of hips with absolute femoral retroversion. For hips with anterior FAI attributed to cam- or pincer-type morphologies, similar acetabular and femoral osseous impingement locations have been reported in the anterosuperior region. 20,50 In a recent study assessing location of labral tears in hips with abnormal FV, the tears were located anteriorly in hips with decreased FV 17 ; those findings correspond with the results of the current study. For patients with THA and femoral retroversion, the location of impingement has been described as between the anterior greater trochanter and the AIIS. 44 For patients with type 3 AIIS, impingement contact between the AIIS and the distal area along the anterior inferior femoral neck has been described, whereas for patients with type 2 AIIS, the impingement contact was localized between the femoral neck and the AIIS. 15
Regarding the clinical assessment of ROM in patients with FAI, the method that we used in the current study is a more accurate and anatomically based quantification of ROM because clinical 46 assessment can be inaccurate. 9 In addition, this method enables the analysis of a specific motion pattern (FADIR test) instead of isolated amplitudes of ROM (eg, maximal flexion without rotation) and the detection of the corresponding patient-specific location of acetabular and femoral impingement. We found no other study with which to compare the results of the impingement area.
This study may have some clinical implications to better understand hip impingement. The location of femoral impingement differed between maximal flexion (anteroinferior [4-5 o’clock]) and the FADIR test (anterosuperior and anterior [2-3 o’clock]). This could be important for orthopaedic surgeons performing hip arthroscopy or open hip preservation surgery. For patients with hip pain in flexion, bone resection (cam resection or acetabular rim trimming) should theoretically be adapted. Based on preoperative measurement of FV, the risk for extra-articular subspine hip impingement could be estimated if a patient with absolute femoral retroversion is identified. Preoperative assessment of decreased combined version and absolute femoral retroversion could help to identify patients with subspine extra-articular hip impingement, similar to preoperative assessment of out-toeing of the foot. Subspine extra-articular hip impingement could be diagnosed with a simple measurement of FV, eliminating the need for time-consuming 3D bone segmentation and impingement simulation for these patients. Furthermore, the study results have implications for daily activities and sports: deep flexion during squats should be avoided in patients with femoral retroversion. 21 In addition, femoral retroversion was previously identified for patients with slipped capital femoral epiphysis. 32,41 Subspine impingement could be a problem for those patients as well, but further studies are needed to investigate this.
Quantification of FV depends on the measurement method. Differences in FV measurements of up to 20° between methods have been described. 42 For example, an FV of –9° measured with the Reikerås method 37 corresponds to an FV of 0° measured with the Murphy method used in this study (assuming a difference of 9° according to a recent study 42 ). Therefore, we propose to use the definition of –9° or –10° to avoid false-positive results for severe femoral retroversion when using the Reikerås method. Interpretation of our results is based on the Murphy method, and the applied method should be considered when reporting FV.
Limitations
This study has limitations. First, the software for collision detection calculates the osseous ROM without taking into account soft tissue (labrum, muscles, or cartilage). This is unavoidable using pelvic CT scans for 3D modeling and could be integrated using MRI of the hip in the future 5,47 or with CT arthrograms. 2,18 Therefore, we believe that the clinical ROM should be even lower in these hips. 2 This means that a patient with absolute femoral retroversion could present clinically with 0° of IR in 90° of flexion. However, this is the case for published ROM results using other software for collision detection. 2 –4 This method has also been applied to hips with severe hip deformities, including hips with high FV, 27,45 hips with slipped capital femoral epiphysis, 25 and hips with deformities caused by Legg-Calvé-Perthes disease. 48 The application of this method to various hip morphologies underlines the validity of the software for collision detection used in the current study.
A second limitation is that the study patients were evaluated for hip preservation surgery in a European university hospital with limited generalizability. There could be a selection bias of complex cases. Third, no detailed surgical outcome or clinical follow-up was reported, because this was not the aim of this study. However, all hips were symptomatic at the time of image acquisition. Of the patients with femoral retroversion, almost half of them (49%) underwent surgical treatment. The current analysis is intended to focus on computer-assisted simulation of ROM in patients with symptomatic anterior FAI and femoral retroversion. Based on this 3D collision detection, we changed our clinical practice and now perform CT or MRI to measure FV in all patients eligible for hip preservation surgery to detect femoral retroversion. Finally, we evaluated the pelvis in a fixed position, without evaluating the effect of pelvic tilt or pelvic incidence, 23 which can affect hip ROM 1 (eg, posterior pelvic tilting to avoid anterior FAI).
Conclusion
Patients with absolute femoral retroversion (FV <0°) had a large hip impingement area, and most exhibited extra-articular subspine impingement and anterolateral femoral impingement. Femoral impingement location differed significantly between maximal flexion (anteroinferior location) and the FADIR test (anterosuperior location). The study findings may have implications for hip preservation surgery, especially for the planning of hip arthroscopy and for patient-specific bone resection and potentially to improve outcomes. Preoperative assessment of FV with advanced imaging (CT or MRI) could help to identify these patients in the future without 3D modeling.
Footnotes
Final revision submitted September 21, 2022; accepted September 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was provided from the Swiss National Science Foundation (grant P2BEP3_195241 to T.D.L.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics commission for the Canton of Bern (No. 2018-00078).