
Abstract
Objective:
This study was conducted to assess the effect of osteochondroplasty on osteoarthritis (OA) prevention, comparing radiological evolution between identical hips from the same patient who had undergone unilateral surgery.
Design:
We retrospectively reviewed radiological evolution between hips with similar shape from the same patient who had undergone unilateral surgery. In all, 56 FAI patients (112 hips) with a mean age of 42.18 ± 9.16 years and had undergone unilateral arthroscopy treatment have been included. Four independent researchers measured Wiberg, Acetabular and Alpha angles, Extrusion index, and Tönnis classification preoperatively to verify that operated and non-operated hips had the same shape. OA evolution was assessed by joint space width (JSW) in 3 different articular points and Tönnis classification.
Results:
No preoperative anatomical differences were present between groups (P > 0.05). At the end of follow-up (31.9 months), a decrease of JSW in the 3 points measured was found in OP hips (OP vs. N-OP; P < 0.01). These results were correlated with changes in the proportion of patients who progressed to grade III in Tönnis classification (from 1.3% preoperative to 23.2% at the end of follow-up).
Conclusions:
Osteochondroplasty and labrum procedures were not associated with OA prevention. The OP hips showed a faster OA degeneration, which was not seen in the N-OP. These results will encourage hip surgeons to perform further investigations to avoid the “Pandora’s Box Opening Process.”
Keywords
Introduction
Diagnosis of femoroactebular impingement (FAI) and its surgical treatment have risen in the past 20 years. Techniques and tools have been improved fast, but some critical doubts about the pathology and surgical indication are still present, compromising functional and pain outcomes. The different randomized clinical trials (RCTs) published to date have a heterogeneous methodology, which makes comparison difficult, leading to different meta-analyses with different conclusions, despite the small number of clinical trials on which they are based.1-4 In parallel, the number of hip arthroscopies performed has grown over 600% in the last 10 years. 5 It is estimated that 4,000 arthroscopic procedures will be performed at the National Health Service (NHS) by 2023. 3
Based on his clinical experience of more than 600 hip surgical dislocations, in 2003, Ganz et al. proposed FAI as a mechanism for the development of early osteoarthritis (OA), through a secondary labrum injury associated with an acetabular (Pincer-type) or femoral (CAM-type) impingement. 6 The procedures associated with hip preservation surgery (HPS) in FAI (femoral and/or acetabular osteochondroplasty and labrum procedures) are focused on the correction of the anatomic morphology, which is supposed to lead to OA to avoid total hip arthroplasty and pain. This mechanical theory has been postulated for many years, and it is far from the multifactorial etiology of OA where genetics plays an important role and is estimated at 70%.7-10 In fact, the presence of unilateral OA is associated with the development of OA in the contralateral hip, regardless of the shape. 11
Haneda et al., in a recent paper, identified metabolic hyperactivity in cartilage from symptomatic patients with early-stage FAI, suggesting that inflammation and degeneration markers are the same as we could expect in patients with OA; however, it does not mean that OA is secondary to FAI.12,13 In the same manner, systemic markers of cartilage turnover and diffuse synovitis observed in OA are present in the early stages of FAI patients and not only in the impingement zone.12,14,15 These data could explain the etiology of the pain in FAI patients, which is not different from the OA degenerative process and sheds some doubts on the value of the HPS concept in OA prevention, because of the poor results reported previously in joints with osteoarthritic microscopic and macroscopic changes.12,14,16-19
Our aim is to assess the effect of osteochondroplasty on OA prevention, comparing radiological evolution between identical hips from the same patient who had undergone unilateral surgery.
Methods
We retrospectively reviewed 56 consecutive FAI patients who had undergone unilateral arthroscopy treatment in 2009, when the technique was implanted in our hospital. We have included patients until the detection of the adverse event, which we call the “Pandora’s box opening process phenomenon” and describe in the present research. We have compared the operated (OP) hip against the contralateral non-operated (N-OP) hip. Inclusion criteria were adult men or women, over 18 years of age, hip pain with physical examination compatible with FAI for more than 6 months with no relief from non-operative means (physiotherapy, non-steroidal anti-inflammatory medication, rest), bilateral shape compatible with FAI, CAM or mixed-type FAI as diagnosed on x-rays and magnetic resonance imaging (MRI) or magnetic resonance arthrogram (MRA). We excluded bilateral surgical patients, patients with hip dysplasia (center edge angle less than 20°), presence of other hip syndromes (concurrent non-FAI-related pathology), history of pediatric hip disease, previous surgery on the affected hip or contralateral hip, and those patients whose x-ray history was impossible to collect and review. Sixty-four patients were initially included, but after evaluating the criteria, we excluded one because of pediatric hip disease (Perthes) and 6 bilateral procedures. Finally, 56 (112 hips) patients were included in the analysis (
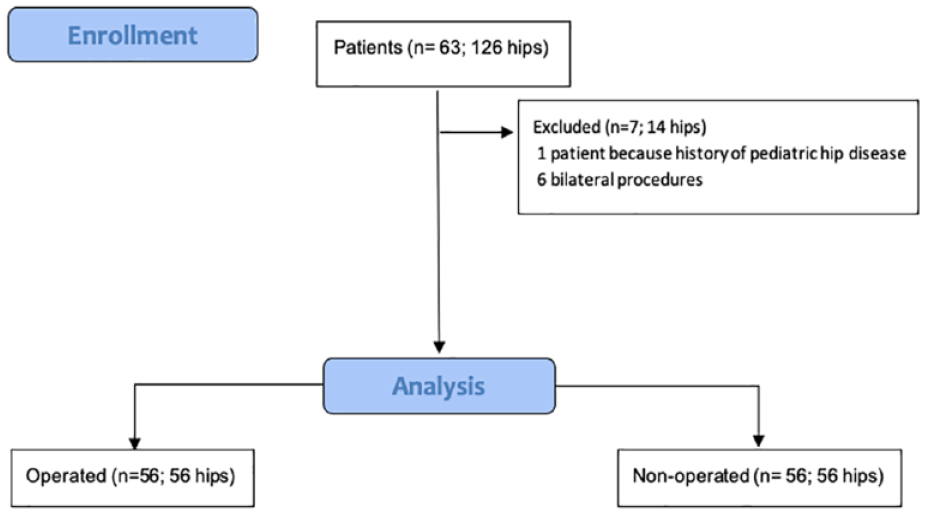
Study flow diagram.
Survival analysis was conducted, considering the presence of Tönnis grade 3 OA or the conversion to total hip arthroplasty as the endpoint event. Furthermore, we compared survival rates based on the baseline Tönnis grade of 0 or 1.
All the procedures were approved by the institutional review board of the Clínica Universidad de Navarra and the Spanish Agency of Medicines and Medical Devices (2021.038 TFG).
Surgical Procedure
Arthroscopic surgery was standardized and performed by 4 different orthopedic hip surgeons, each with varying levels of experience. One surgeon, with an average of 20 arthroscopies per year, performed 44 interventions. Two high-volume surgeons, who typically perform 100 procedures per year, conducted a total of 4 surgeries. Additionally, 2 novice surgeons, under the guidance of more experienced colleagues, performed 8 surgeries.
Surgery was performed under general anesthesia in the supine position. Arthroscopic portals were established in the central and peripheral compartment, according to each surgeon’s usual practice. Osteochondroplasty at the acetabular rim and the head-neck junction was assessed by intraoperative image intensifier radiograph, and satisfactory impingement-free range of movement of the hip was checked intraoperatively. Labrum pathologies were treated at the same time. The quality of surgery was defined as a postoperative alpha angle of 55° or less or at least 20° of relative correction.20,21
Femoral osteochondroplasty was performed in all cases: acetabuloplasty for Pincer-FAI in 13 cases (23.21%), and labrum rupture was identified in 31 cases (55.35%), of which labrum repair was performed in 26 cases (46.64%) and labral regularization in 5 cases (8.9%).
Radiological Measurement
Four independent researchers measured the hips to minimize bias, and the mean value was used to build the database. In the preoperative study, we used 2 x-ray views of the hip, an anteroposterior view and a Dunn x-ray view. 22
The alpha angle is formed by the axis of the femoral neck and a line connecting the center of the femoral head to the point where the asphericity of the headfirst is evident. 23 Alpha angle was measured in the Dunn view, and an alpha angle larger than 55° defines CAM-type FAI. The lateral center-edge or Wiberg angle (WA) is the angle formed by a line drawn through the center of the femoral head and perpendicular to the horizontal line of the pelvis and a line connecting the center of the femoral head and the lateral lip of the acetabulum. Its normal values range from 25° to 40°. A WA less than 20° can classify as hip dysplasia. 24 The Femoral Head Extrusion index is defined as the percentage of the femoral head that is not covered by the acetabulum. An extrusion index larger than 25% is suggestive of hip dysplasia. 25 The Tonnïs angle or acetabular index (AI) is formed by a line connecting the two ends of the acetabular sourcil and the horizontal line of the pelvis. 26 An angle less than 0° is suggestive of a Pincer-type FAI. The Tönnis classification was used to assess the evolution of hip OA. It is divided into 4 grades: grade 0 meaning normal morphology of the joint; grade 1 describes the start of the narrowing of the joint space and slight sclerosis of the acetabulum; grade 2 describes the presence of further OA signs such as cysts, clear narrowing of the joint space, and femoral head asphericity; and grade 3 indicates severe narrowing or complete loss of the joint space, larger cysts, osteophytes, severe asphericity of the head, and/or avascular necrosis and is the most critical grade.27,28
To classify the severity and evaluate the narrowing of the articular space, the hip joint space width (JSW) was measure at 3 different points (lateral, center, and medial) on anteroposterior x-rays. The space measured is between the femoral head surface and the acetabular sourcil at a 90° angle, perpendicular to the femoral head center (
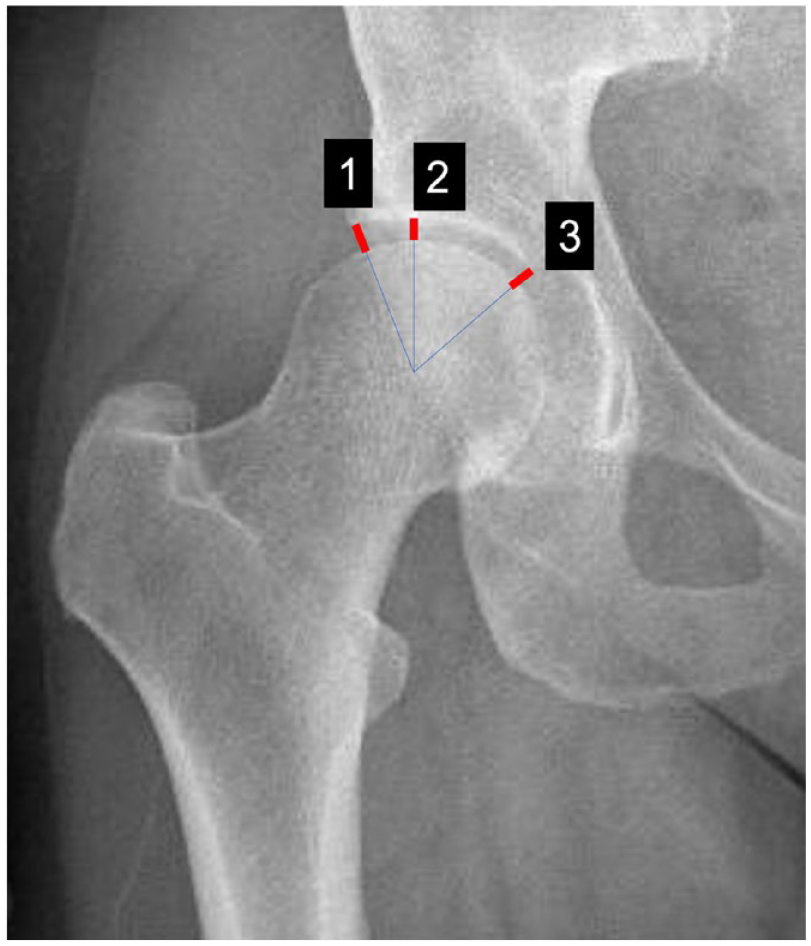
Schematic drawing of the joint space width measured at 3 different weight-bearing points measured by 4 independent investigators (26).
Statistical Analysis
Data were summarized using means and standard deviations. The Kolmogorov-Smirnov test was used to test the normality assumption. Paired test and 2-tailed t tests were used as appropriate. A P value <.05 was considered statistically significant. Overall survival data were expressed as Kaplan-Meier curves, and groups (Tönnis 0 vs Tönnis I) were compared by means of the log-rank test (Mantel-Cox test). All the statistical analyses were performed using SPSS 21 (Stata Corp. 2015. Stata Statistical Software: Release 14. Stata Corp LP, College Station, TX).
Results
Demographic Data and Basal Angular Hip Description
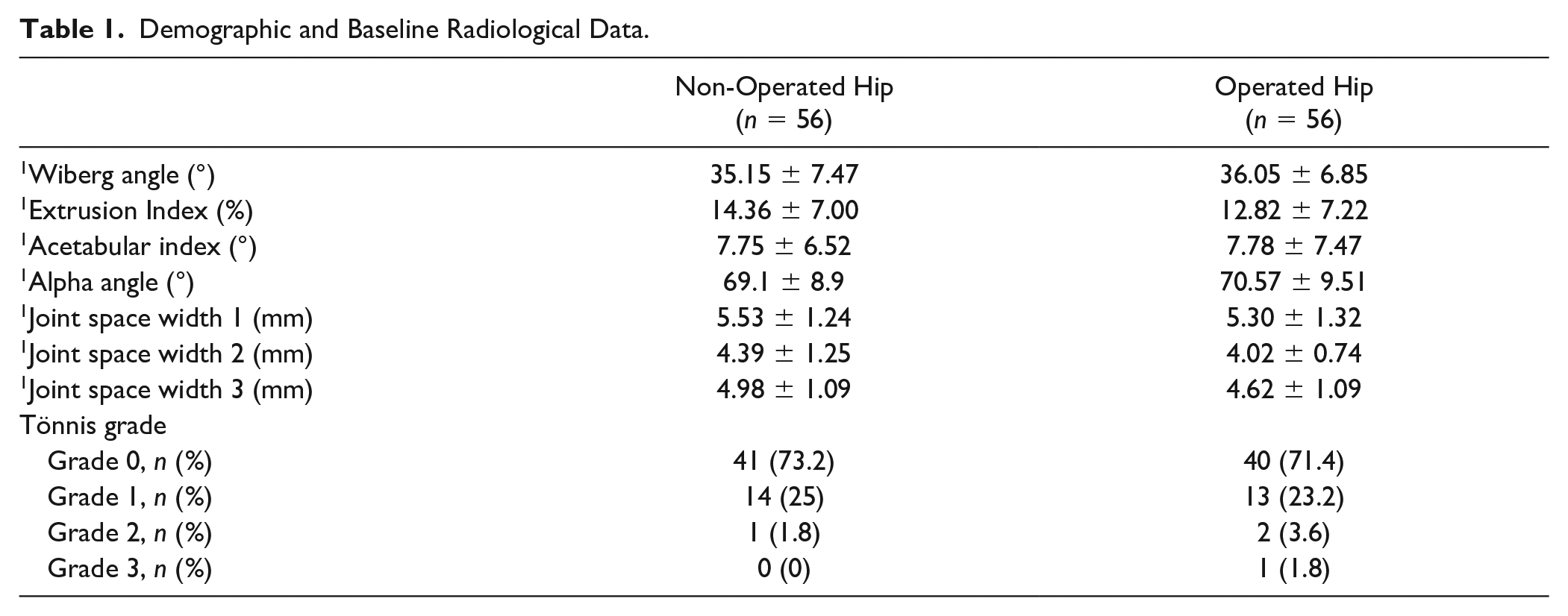
The final sample consisted of 112 hips (56 OP and 56 N-OP) from 56 patients. The average age of the patients was 42.18 ± 9.16 years. In all, 55.35% of the OP hips were right, and 44.5% were left. Mean follow-up duration was 31.9 (2-155) months. No difference in shape between groups was assessed before the surgical procedure (P > .05). This allowed us to state that both groups were anatomically similar before going under surgery, which enabled us to compare the evolution ( Table 1 ).
Demographic and Baseline Radiological Data.
Radiological Analysis
No differences in the angular analysis were present at the end of the follow-up between groups, except for the alpha angle, which showed a difference in the OP group with a presurgical value of 70.57 ± 9.50 and postsurgical value of 49.98 ± 6.70 (P = .01) with a mean correction of 20.6° (95% confidence interval [CI]: 18.00-23.26) ( Table 2 ).
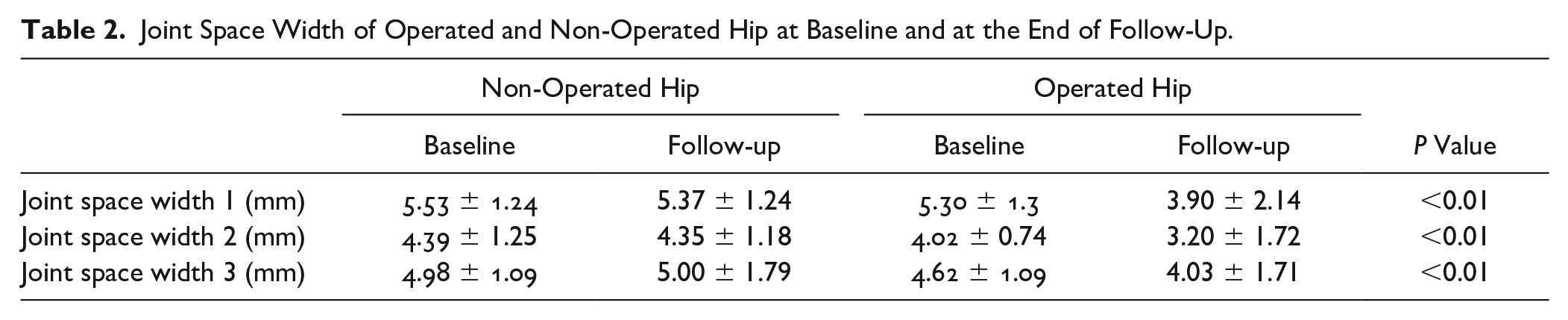
Joint Space Width of Operated and Non-Operated Hip at Baseline and at the End of Follow-Up.
JSW and Tönnis Classification
Four independent investigators measured the JSW, at 3 hip joint space points, and the Tönnis classification to evaluate OA development. In the OP hip group, JSW changed at 3 weight-bearing points from 5.3 ± 1.3, 4.02 ± 0.7, and 4.62 ± 1.09 mm to 3.9 ± 2.1, 3.2 ± 1.7, and 4.0 ± 1.7 mm, respectively (P < 0.01), whereas in the N-OP group, no change was detected in JSW during the follow-up ( Table 2 ).
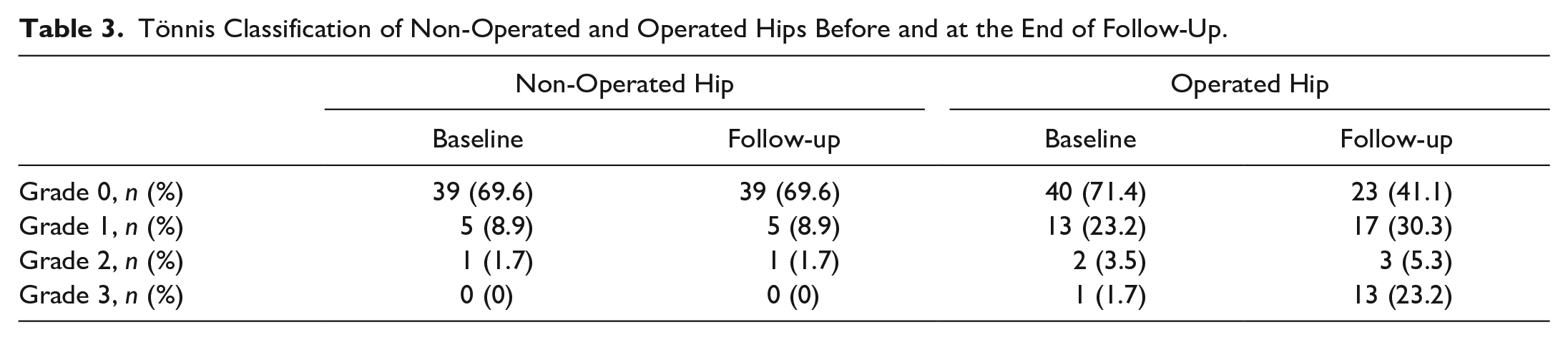
JSW reduction was correlated with degenerative articular deterioration, as we have seen in the Tönnis grade distribution before and after the FAI correction procedure. In the OP group, an increase in the prevalence in Tönnis grade 3 from 1.7% of the cases preoperatively to 23.2% of the cases at the end of follow-up at 31.9 (2-155) months was assessed (1.7% vs. 23.2%) (
Table 3
). In the N-OP group, the Tönnis distribution grade did not change, with no hips in grade 3 at the end of follow-up (
Tönnis Classification of Non-Operated and Operated Hips Before and at the End of Follow-Up.
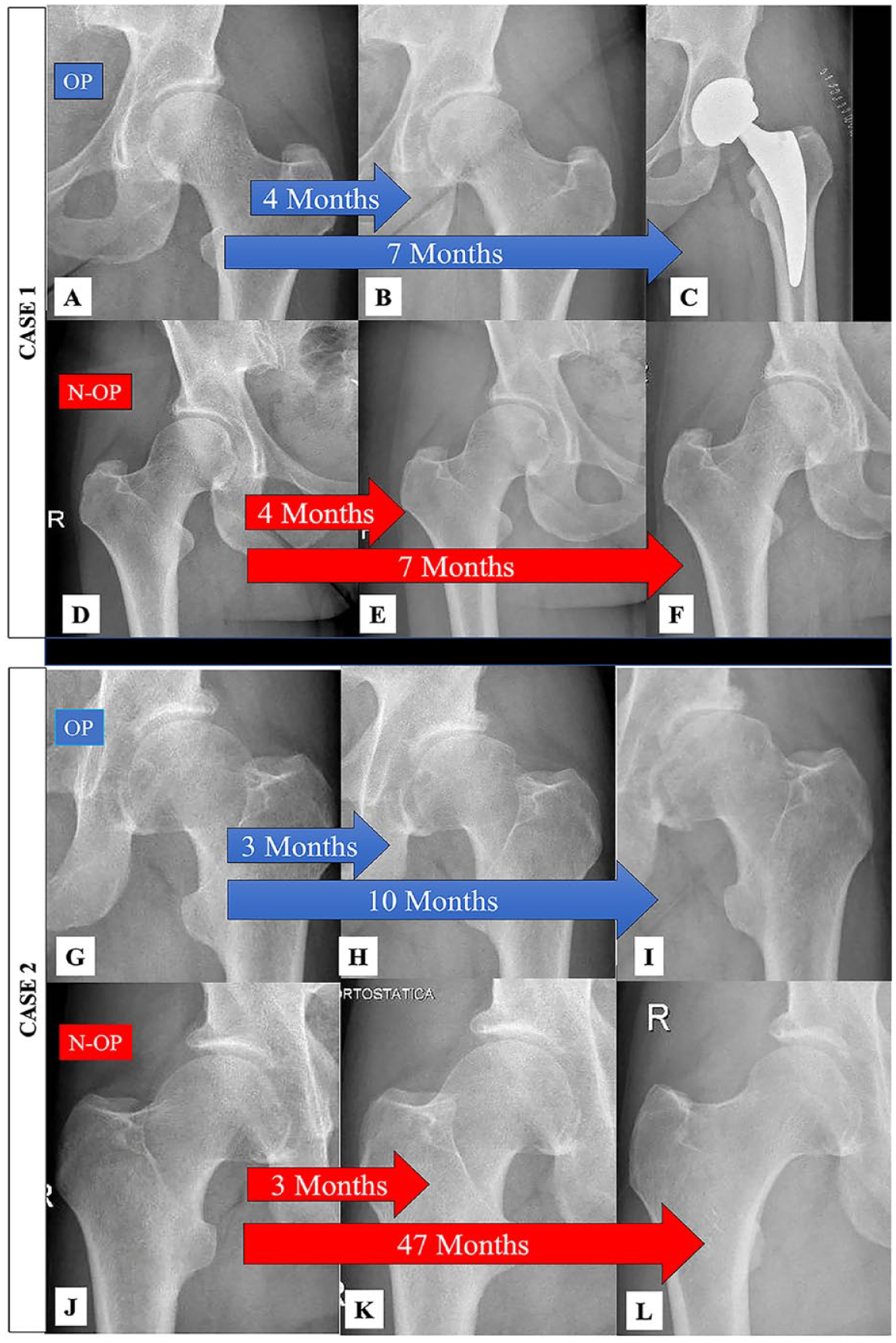
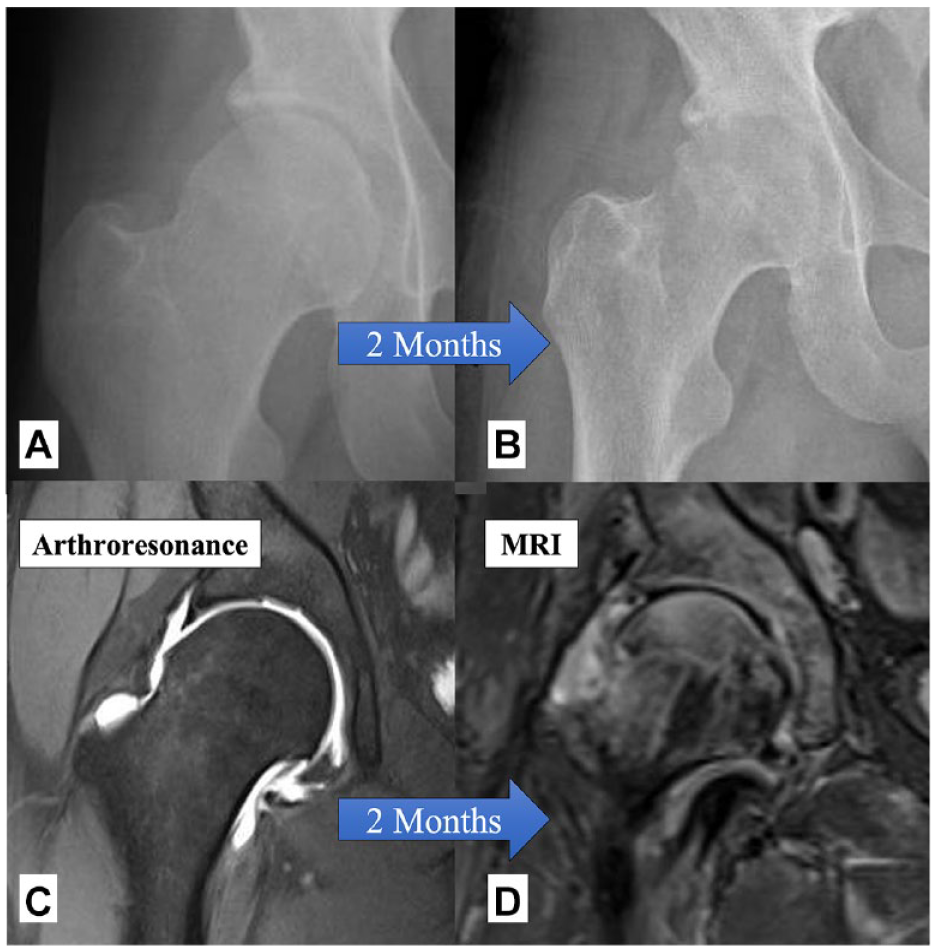
Case 1. (
The analysis of JSW by age indicates a consistent pattern of joint deterioration in the OP hips. In the ≤40 years and >40 years age groups, significant reductions in JSW are observed compared to the N-OP hip (
Suppl. Tables S1
and
The distribution of Tönnis grades in operated hips before and at the end of follow-up, stratified by age groups (≤40 years and >40 years), revealed a decrease in the proportion of Tönnis grade 0 cases and an increase in the proportion of higher-grade cases in both age groups at the end of follow-up, indicating a progression of hip degeneration ( Suppl. Table S3 ).
In the analysis of overall survival, a total survival rate of 0.75 was observed (
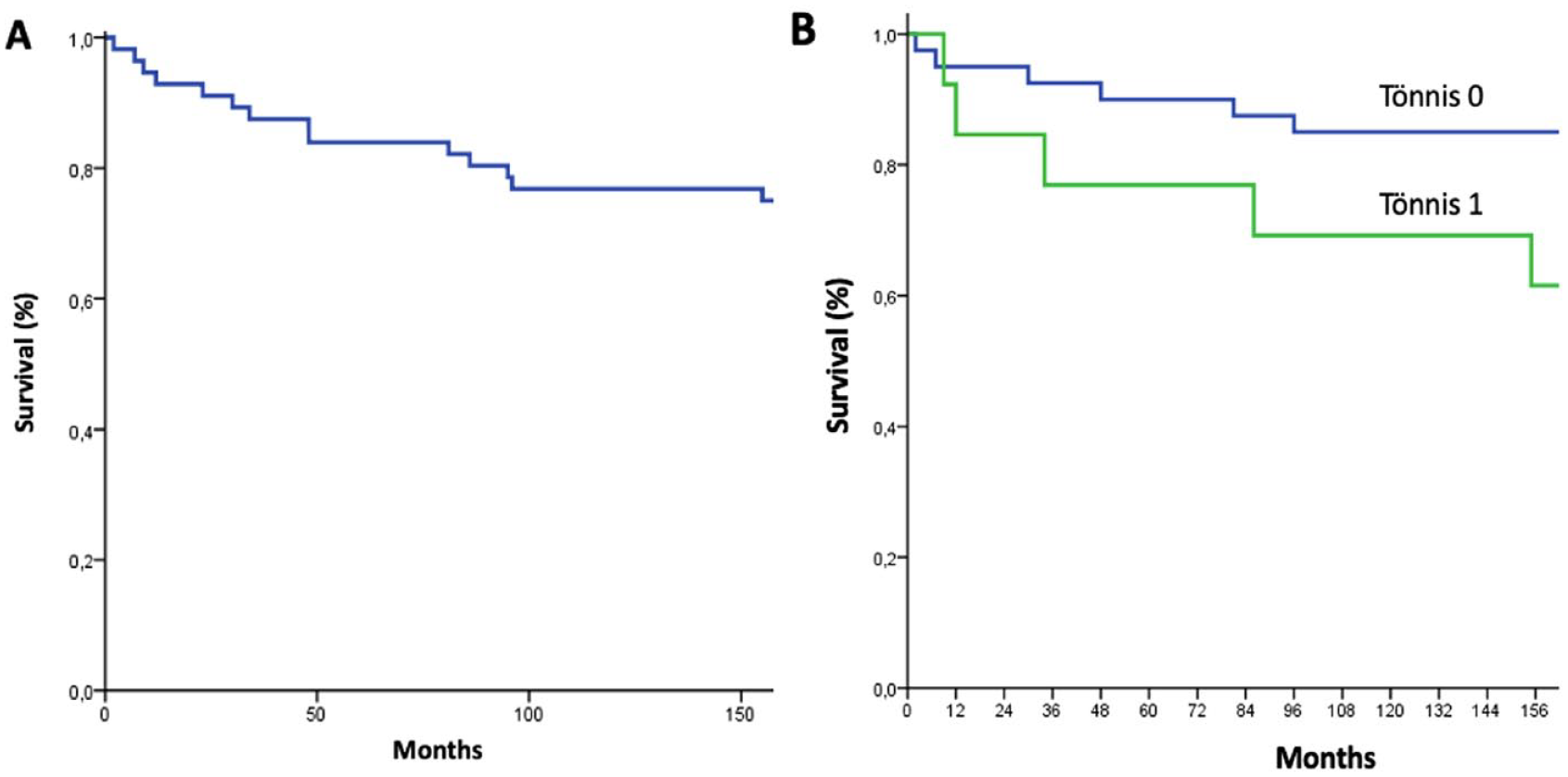
(
Discussion
The procedures associated with HPS in terms of OA prevention in FAI (osteochondroplasty and labrum procedures) are focused on the correction of the anatomic morphology, which is supposed to lead to OA. Our major finding is that osteochondroplasty and labrum procedures were not associated with OA prevention, defining the “Pandora’s box opening process” as an adverse event defined by a fast JSW reduction and OA progression after osteochondroplasty.
Several factors could affect the joint after osteochondroplasty, defining the “Pandora’s box opening process.” Femoral osteoplasty consists of creating an osteochondral lesion in the femoral head to reduce the alpha angle. Although the osteochondral lesion is intended to avoid the loading zone, it is intraarticular and may extend many square centimeters. The spherical shape of the head is achieved through different types of motorized high-revolution burrs over the bump. We should note that articular cartilage from the impingement zone of hips with CAM expresses higher levels of inflammatory, anabolic, and catabolic genes, representing a heightened metabolic state.
30
When subchondral bone is exposed and cartilage and bone detritus are produced and delivered, the “Pandora’s box” is now open, and the cartilage and bone-delivered fragments make contact with a synovial membrane in an inflammation environment that has been previously described in FAI patients.12-14,30,31 The products of the cartilaginous matrix have the potential capacity to activate inflammatory cells that are well known to be present in the synovial membrane (macrophages, fibroblasts, and T cells) of FAI patients.
32
Upon contact with these fragments, synovial cells react by producing more inflammatory mediators (prostaglandin E2, nitric oxide, and reactive oxygen species), which lead to further activation in the remaining chondrocytes of metalloproteinases, with increased cartilage degradation and production of proinflammatory cytokines such as TNF-alpha and IL-1 beta, and aggravated because of the activation of the subchondral bone
33
(
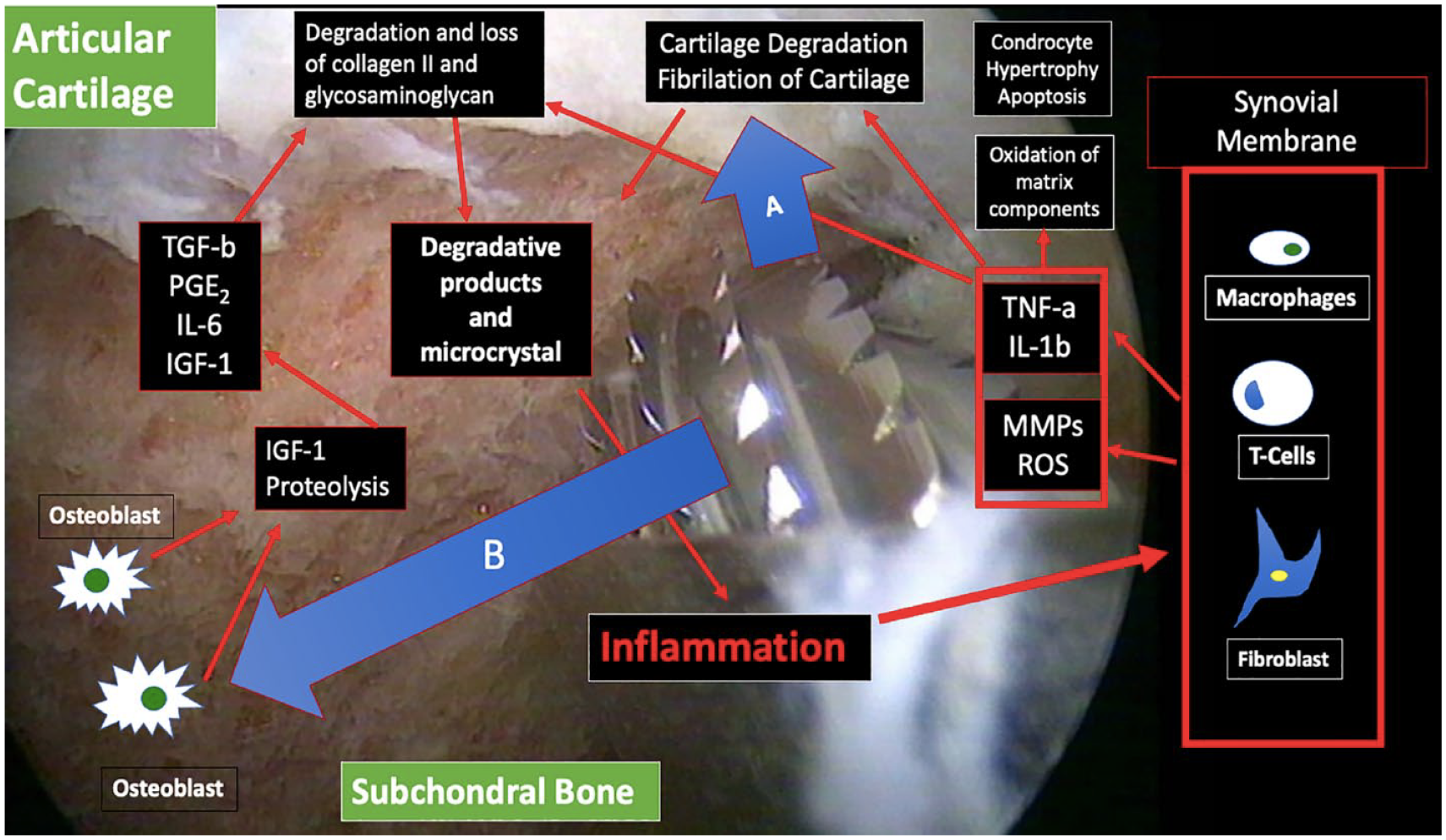
Physiopathology of the “Pandora’s box opening process”: To reduce the alpha angle, osteochondroplasty is carried out on the articular cartilage (
(
Some authors have reported worse cartilage changes after osteochondroplasty, which are broadly consistent with our results.35-37 The Australian FASHion RCT published the data from semi-quantitative MRI (dGEMRIC technique) showing worse cartilage and labral scores in the arthroscopic group at 12 months in comparison to physiotherapy group. 35 Rhon et al. in 2019 observed that 21.9% of patients developed OA in just 2 years after hip arthroscopy treatment, 37 similar to that observed by Bardakos and Villar in non-operated patients, at 10 years of follow-up. 24 Despite the aforementioned findings, in 2019, Olach reported no progression of OA in a sample of 20 patients with OA after more than 10 years of follow-up following arthroscopy. However, it is important to note that the analysis did not take into account the patients who had to undergo total hip replacement during the follow-up period, which represented 25.6% of the total sample size of 43 patients. 38
Pincer-type association with OA is unknown.8,39,40,41 Pincer-type morphology has been described in 67% of 2,114 hips in asymptomatic patients with a mean age of 25 years and has been considered to be a protective factor for OA in studies with follow-up close to 20 years because of a more homogeneous distribution of loads.8,24,40,41 Acetabuloplasty reduces the load surface and requires a partial detachment and reattachment of the labrum, which could affect the vacuum effect that the hip has with a fully intact labrum. In other words, if pincer effect does not seem to correlate with the development of early OA, the orthopedic surgeon should at least be careful when indicating acetabuloplasty, especially in cases where the labrum is not damaged and partial detachment and reattachment of the labrum is required, partially losing their vacuum effect. Our study is not exempt from limitations. The sample size and follow-up are small, but the results reported define well the “Pandora’s box opening process” and have modified our behavior in the same manner as, during a clinical trial, investigators detect an adverse event. We have described a phenomenon that should be the focus of future research.
The mean age of the participants was 42 years, which can be considered relatively advanced because it is worldwide accepted that arthroscopy is more effective in younger people.20,29 However, in the UK FAShion RCT, the only level I study analyzed by age groups, a greater proportion of elderly participants achieved a minimum clinically significant improvement. The International Hip Outcome Toll-33 scores were 5.0 (95% CI: −1.2 to 11.3) for participants younger than 40 years and 10.9 (1.7-20.1) for those older than 40 years. It is important to note that both groups’ CIs include the minimal clinical difference of 6.1 points. 39 Our findings highlight the age-independent nature of joint degeneration following surgery.
Although the OP and N-OP groups can be considered identical in bone shape, labrum lesions have not been determined in the N-OP group. However, according to the high prevalence of labral lesions in asymptomatic hips (80%-96%), we could suppose that the differences would not be important.42-48 The prevalence of labrum lesions in patients older than 30 years has been reported in 80% to 96% with no relationship between CAM morphology-labrum ruptures and CAM morphology-mechanical pain.42-48 As a consequence, labrum lesions are highly prevalent among people older than 30 years. In 3,202 patients, Gosvig et al. found no correlation between CAM morphology with mechanical groin pain and CAM morphology with hip OA. 48 Philippon et al., in 2013, in a study of asymptomatic individuals, observed a prevalence of CAM type in 75% of ice hockey players and 40% of skiers. 47 Curiously, despite this difference in the prevalence of the CAM morphology, no differences in labrum lesions were reported between groups. 47 Furthermore, the relationship between labrum injury and OA development was studied in a cadaveric study. With a mean age of 78 years, 96% of the hip presented labrum injury, and 67% showed no OA changes. 46
The Tönnis scale has a subjective component. To minimize bias, the evaluation has been performed by 4 independent researchers. We should note that subjective component is small when we describe the grade 3, which JSW is 0 mm.
In summary, osteochondroplasty and labrum procedures were not associated with OA prevention. The OP hips showed a faster OA degeneration, which was not seen in the N-OP hips. These results will focus on hip surgeons for further investigations to avoid the “Pandora’s Box Opening Process.”
Supplemental Material
sj-docx-1-car-10.1177_19476035231191202 – Supplemental material for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process
Supplemental material, sj-docx-1-car-10.1177_19476035231191202 for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process by José M. Lamo-Espinosa, Jorge Gómez-Álvarez, Elena Pascual Roquet-Jalmar, Asier Iribarren, Anne Recke, María Cruz Roa, Andrés Valentí-Azcárate, Froilán Granero-Moltó and Mikel San-Julián in CARTILAGE
Supplemental Material
sj-docx-2-car-10.1177_19476035231191202 – Supplemental material for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process
Supplemental material, sj-docx-2-car-10.1177_19476035231191202 for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process by José M. Lamo-Espinosa, Jorge Gómez-Álvarez, Elena Pascual Roquet-Jalmar, Asier Iribarren, Anne Recke, María Cruz Roa, Andrés Valentí-Azcárate, Froilán Granero-Moltó and Mikel San-Julián in CARTILAGE
Supplemental Material
sj-docx-3-car-10.1177_19476035231191202 – Supplemental material for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process
Supplemental material, sj-docx-3-car-10.1177_19476035231191202 for Femoroacetabular Impingement and the Effect of Osteochondroplasty on Hip Osteoarthritis Prevention: The Pandora’s Box Opening Process by José M. Lamo-Espinosa, Jorge Gómez-Álvarez, Elena Pascual Roquet-Jalmar, Asier Iribarren, Anne Recke, María Cruz Roa, Andrés Valentí-Azcárate, Froilán Granero-Moltó and Mikel San-Julián in CARTILAGE
Footnotes
Authors’ Contributions
Conceptualization, J.M.L.-E. and M.S.-J.; methodology, J.M.L.-E., J.G.-A., E.P.R.-J., M.S.-J.; formal analysis, J.M.L.-E., J.G.-A., E.P.R.-J.; resources, J.M.L.-E.; A.V.-A.; A.I.; M.C.R.; data curation, A.I., A.R., M.C.R., and A.V.-A..; writing—original draft preparation, J.M.L.-E., J.G.-A., E.P.R.-J., M.S.-J., F.G.-M.; writing—review and editing, J.M.L.-E.; J.G.-A.; A.V.-A.; F.G.-M.; A.R.; M.S.-J.; A.V.-A.; E.P.R.-J. All authors have read and agreed to the published version of the manuscript.”
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All the procedures were approved by the institutional review board of the Clínica Universidad de Navarra and the Spanish Agency of Medicines and Medical Devices (2021.038 TFG).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.