
Abstract
Background:
Characteristics regarding mechanism of injury, management, and return-to-play (RTP) rate and timing are important when treating and counseling athletes with rectus femoris tears.
Purpose:
To systematically review the literature to better understand the prevalence, sporting activity, injury mechanisms, and treatment of patients with rectus femoris injury and to provide prognostic information regarding the rate and timing of RTP.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Following the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, we queried PubMed/MEDLINE, Cochrane, OVID, EMBASE, and Google Scholar in March 2022 for studies reporting on athletes sustaining isolated, full-thickness tearing, or bony avulsion injuries to the proximal rectus femoris during sporting activity. Excluded were studies without evidence of full-thickness tearing or avulsion, with athletes sustaining concomitant injuries, or with injuries occurring from nonsporting activities. The percentage of athletes sustaining injuries was calculated based on sport, injury mechanism, and management (nonoperative versus operative).
Results:
Of 132 studies initially identified, 18 were included, comprising 132 athletes (mean age, 24.0 ± 5.4 years; range, 12-43 years). The most common sporting activities were soccer (70.5%) and rugby (15.2%). The most reported mechanisms of injury were kicking (47.6%) and excessive knee flexion/forced hip extension (42.9%). Avulsion injuries were reported in 86% (n = 114) of athletes. Nonoperative management was reported in 19.7% of athletes, with operative management performed in 80.3%. The mean follow-up time was 21.4 ± 11.4 months (range, 1.5-48 months). The RTP rate was 93.3% (n = 14) in nonoperatively treated and 100% (n = 106) in operatively treated athletes, and the mean RTP time was 11.7 weeks (range, 5.5-15.2 weeks) in nonoperatively treated and 22.1 weeks (range, 14.0-37.6 weeks) in operatively treated athletes. Complications were reported in 7.7% (2/26) of nonoperatively treated and 18% (n = 19/106) of operatively treated athletes.
Conclusion:
Full-thickness proximal rectus femoris injuries occurred most frequently in athletes participating in soccer and rugby secondary to explosive, eccentric contractions involved in kicking and sprinting. Operative management was performed in the majority of cases. Athletes who underwent operative repair had a 100% RTP rate versus 93.3% in athletes treated nonoperatively.
Injuries to the quadriceps complex represent a common cause of pain and time lost from sport in athletes, predominately those participating in American football, soccer, track and field, and rugby. 9,23 As the most superficial component of the quadriceps, the rectus femoris consists of the direct head, originating from the anteroinferior iliac spine, and the reflected, or indirect head, arising from the superior acetabular ridge. 25 In the quadriceps complex, the rectus femoris represents the most commonly injured muscle, 5,7 frequently attributed to the biarthrodial nature of the muscle, crossing both the hip and the knee joint. 8 Due to the infrequent reporting of injuries to the proximal rectus femoris, the potential for misdiagnosis and undertreatment remains high. 7,16,29
Proximal rectus femoris injuries are commonly reported as a result of movements associated with rapid eccentric muscle contraction and acceleration/deceleration, such as kicking or sprinting. 2,19 In the kicking athlete, the tendon is maximally elongated during hip extension and knee flexion, placing the muscle at risk for tearing or avulsion proximally during rapid contraction. 15,17,18 Moreover, abrupt arrest of the kicking motion during the strike phase further increases the risk of injury, such as when a kick is blocked by an opponent. 7,8,28 In nonkicking athletes, sprinting is a commonly reported mechanism of injury due to the eccentric forces placed on the proximal rectus femoris during the swing phase of acceleration, as well during the deceleration phase, in which asynchronous muscle activation and force dissipation occurs from the muscle belly to the tendon.2,11,13,18
The frequency, characteristics, and optimal treatment modalities for athletes sustaining proximal rectus femoris injuries remain largely unknown. The purpose of this investigation was to (1) systematically review the literature to better understand the prevalence, sporting activity, injury mechanisms, and treatment of patients with full-thickness proximal rectus femoris injuries and to (2) provide prognostic information regarding the rate and timing of return-to-play (RTP), to better inform clinicians when counseling patients and framing athletes’ expectations. We hypothesized that (1) injuries would be reported most frequently in athletes involved in sports requiring frequent and repetitive sprinting and kicking (ie, American football, track and field, rugby, soccer) and (2) operatively and nonoperatively treated athletes would experience similar RTP rates, timing, and complications.
Methods
Search Criteria and Article Selection
A systematic review was conducted, with articles identified and extracted according to the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. After registration on the PROSPERO International Prospective Register of Systematic Reviews (ID: CRD42021283235), all studies written in English or with English-language translation between January 1988 and March 2022 reporting on athletes sustaining isolated injuries to the proximal rectus femoris during sporting activity were identified. A sporting activity was defined as any event in which an athlete was in competition with fellow athletes, irrespective of competitive level. Two authors (D.M.K., A.G.) performed an independent qualitative systematic review of the literature on March 10, 2022, using the PubMed/MEDLINE, Cochrane, OVID, EMBASE, and Google Scholar databases. A combination of the following search terms was included: “proximal rectus femoris” AND “injury” AND “rupture” AND “tear” AND “athlete” AND “sport” AND “return to play” AND “operative” AND “repair” AND “non-operative,” AND “conservative.”
Articles were included in the systematic review and assessed for quality when meeting the following inclusion criteria: articles written in English or with English-language translation, athletes sustaining proximal rectus femoris avulsions, bony avulsions, or full-thickness musculotendinous junction (MTJ) injuries during sporting activities diagnosed on clinical and imaging evaluation with reported sporting activity causing injury, treatment (nonoperative versus operative), return-to-sport rate and timing, and the incidence of any complications related to injury management. Exclusion criteria consisted of studies reporting proximal rectus femoris injuries without evidence of tearing or avulsion, partial-thickness injuries or strains, athletes sustaining proximal rectus femoris injuries with concomitant injuries to the hip (ie, labral injury, core muscle injury) or knee; injuries occurring as a result of nonsporting activities (ie, walking, jogging, mechanical falls, trauma, or activities not meeting the definition of a sporting activity); and studies not reporting on injury treatment, complications, or return to play (RTP).
Variables of Interest
When reported, proximal rectus avulsion injuries were classified based on injury location, with involvement of the direct, indirect, or direct plus indirect heads. Injuries were further classified into 1 of 3 full-thickness injury patterns: (1) soft tissue avulsion injuries of the proximal tissue from the bony attachment site, (2) bony avulsion fracture, or (3) MTJ tears. Collected data consisted of sporting activity at the time of injury, as well as mechanism of injury. Treatment was classified as either operative or nonoperative. Due to the heterogeneity of patient-reported outcome measures, no statistical analyses were performed based on the treatment of rectus femoris avulsion injuries.
A total of 132 articles were identified after the database search. Any disagreements between the 2 authors were resolved by a third author (M.J.M.); no disagreements were encountered. The search process is shown in the flow diagram (Figure 1). A total of 33 studies were selected for full-text evaluation after title and abstract assessment. Of these studies, 15 were excluded due to injuries sustained during nonsporting activities (n = 7 studies), no data demonstrating clinical and imaging findings consistent with proximal rectus femoris tearing or avulsion (n = 5 studies), or absence of data regarding injury management (n = 3 studies). After application of the inclusion and exclusion criteria, a total of 18 articles were included for analysis. To guarantee that all available studies meeting inclusion criteria were identified, references in each of the included articles were cross-referenced for inclusion in case they were overlooked during the initial search, during which no further studies were identified.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the study inclusion process. .
Assessment of Study Quality
To assess the quality of the included studies, the Modified Coleman Methodology Score (MCMS) was used, which allows for evaluation of study methodology on the basis of 10 criteria, giving a total score between 0 and 100. The subsections that comprise the MCMS are based on the subsections of the CONSORT (Consolidated Standards for Reporting Trials) statement (for randomized controlled trials) that were modified to allow for other trial designs. 5 The Coleman criteria were modified to make them reproducible and relevant for a systematic review evaluating proximal rectus femoris injuries in athletes. Each study was scored independently in duplicate by 2 authors (initials blinded for peer review) for each of the criteria adopted. No disagreement with score differences of >3 points were appreciated. Scores ranging from 85 to 100 were considered excellent, 70 to 84 good, 55 to 69 fair, and <55 poor.
Statistical Analysis
The percentage of athletes sustaining proximal rectus femoris injuries was calculated based on sport, reported injury mechanism, and injury management (nonoperative versus operative). Continuous variables were presented as means and standard deviations. Categorical variables were presented as percentages. Weighted scores were calculated for continuous variables as previously reported using the following formula 3 :

All statistical analyses were performed using Rstudio (Version 4.0.2, R Core Team).
Results
Patient Demographics, Sport Activity, and Mechanism of Injury
Included were 18 articles consisting of 132 athletes (mean age, 24.0 ± 5.4 years [range, 12-43 years]), of which 94% (124/132) were male. ∥ The most commonly involved sporting activities were soccer (70.5%; 93/132), rugby (15.2%; 20/132), and American football (12.1%; 16/132) (Table 1). Of the 18 studies, 15 studies (n = 63 athletes) reported a specific mechanism of injury (Table 2). ¶ Mechanism of injury was not reported in 1 study of 55 athletes, 17 with incomplete reporting in 1 study (not reported in 9/11 athletes), 11 and 1 study reporting a nonspecific mechanism of injury (eccentric mechanism; 5 athletes). 28 When specifically reported, the most frequent mechanisms of injury were kicking (47.6%; 30/63), excessive knee flexion and forced hip extension (42.9%; 27/63), and sprinting (9.5%; 6/63) (Table 2).
Overview of Included Studies a
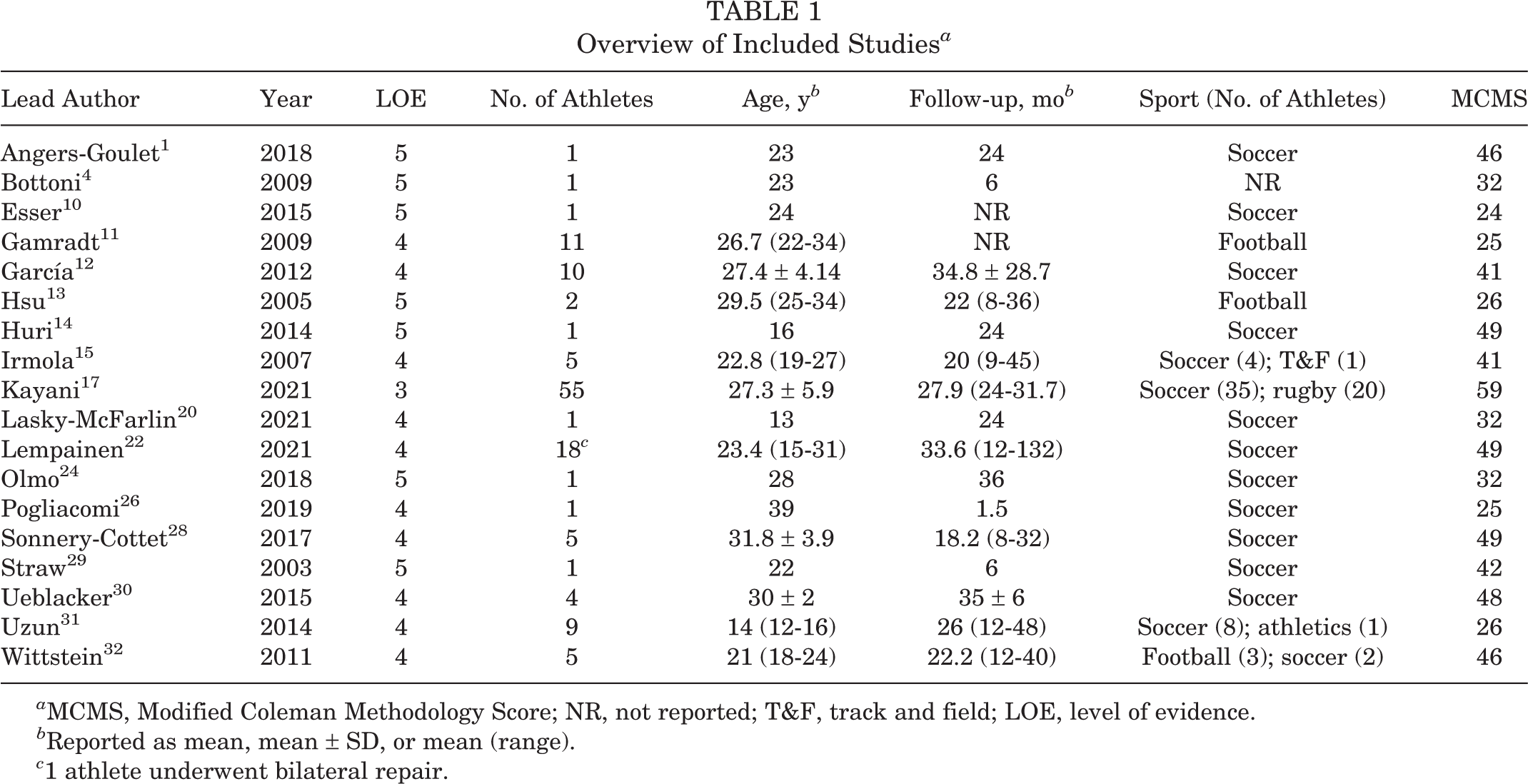
a MCMS, Modified Coleman Methodology Score; NR, not reported; T&F, track and field; LOE, level of evidence.
b Reported as mean, mean ± SD, or mean (range).
c 1 athlete underwent bilateral repair.
Overview of Injury Mechanism, Location, Treatment, and Complications a

a CT, computed tomography; DH, direct head; IH, indirect head; LFCN, lateral femoral cutaneous nerve; MRI, magnetic resonance imaging; MTJ, musculotendinous junction; Nonop rehab, nonoperative rehabilitation; NR, not reported; NSAID, nonsteroidal anti-inflammatory drug; PRP, platelet-rich plasma; RTP, return-to-play; US, ultrasound; XR, radiograph.
b Parentheses signify number of athletes.
c Parentheses signify date range.
d PRP injection provided at postinjury days 5 and 16.
e PRP injections performed at postinjury days 10, 20, and 30.
Anatomic Involvement of Injury and Management
Of the 132 patients, 114 experienced proximal avulsion injuries, 8 had MTJ ruptures, and 10 had bony avulsion fractures (Table 1). Nonoperative management was reported in 19.7% of athletes (7 studies 10,11,13,20,24,26,31 ; 26 athletes) with proximal rectus avulsion injuries (15 athletes), bony avulsion fractures (10 athletes) and MTJ ruptures (1 athlete). Nonoperative management generally consisted of rest, platelet-rich plasma injections, 24,26 and physical therapy, emphasizing hip range of motion and core strengthening. Operative management was performed in 80.3% of athletes (11 studies; 106 patients) with rectus avulsions (99 athletes) and MTJ ruptures (7 athletes). Operative management consisted of primary repair utilizing suture anchors (60.4%; 64/106 athletes), primary tenodesis via excision of periosteum and suture of the muscle belly to surrounding muscle (33.0%; 35/106 athletes) or direct side-to-side suture repair (6.6%; 7/106 athletes) (Table 2).
Return-to-Sport Rates and Timing
The mean final follow-up time for all athletes was 21.4 ± 11.4 months (range, 1.5-48 months). The mean follow-up periods for nonoperative and operative patients were 18.1 ± 14.5 and 22.9 ± 10.2 months, respectively. The RTP rate was reported in 17 studies (121 athletes), # with 93.3% (14/15) of nonoperatively and 100% (106/106) of operatively treated patients returning to play at their preinjury level. RTP timing was reported in 5 studies 11,13,20,24,26 (16 athletes) reporting nonoperative management and 11 studies (106 athletes) reporting on operative management. ** Mean RTP timing in patients undergoing nonoperative and operative management was 11.7 weeks (range, 5.5-15.2 weeks) and 22.1 weeks (range, 14-37.6 weeks), respectively.
Complications
Complications were reported in 18% (19/106) of athletes who underwent operative management, with symptomatic lateral femoral cutaneous nerve (LFCN) neurapraxia being the most commonly reported complication (Table 3). Recurrent proximal rectus femoris avulsion injuries within 6 months of surgery were reported in 4% (4/106) of athletes, with 4 athletes returning to play after treatment involving debridement of the avulsed tendon stump and revision tenodesis. 17 Recurrent pain was reported in 7.7% (2/26) of athletes treated nonoperatively.
Complications of Proximal Rectus Femoris Avulsion a
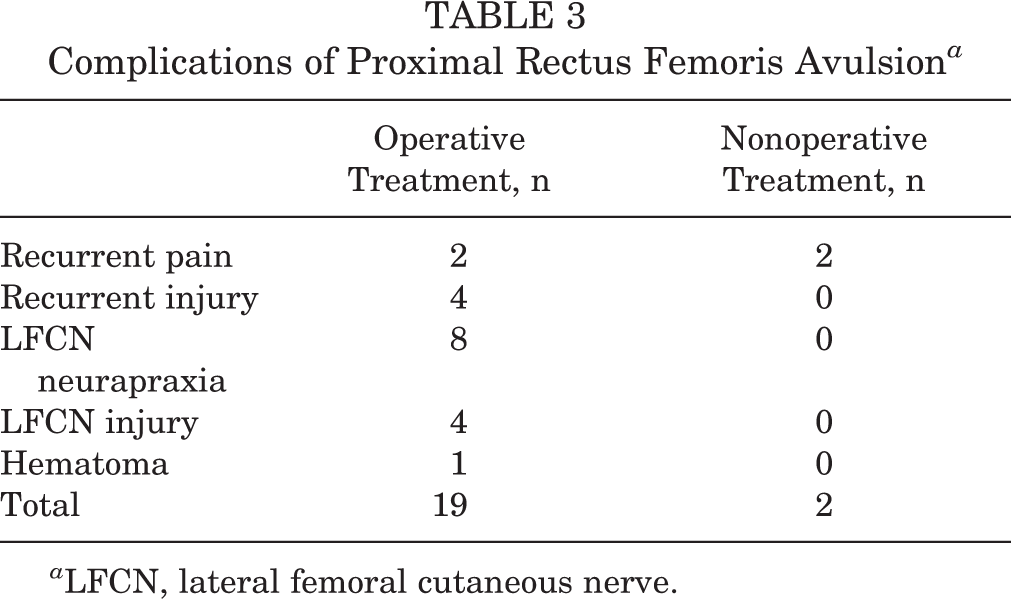
a LFCN, lateral femoral cutaneous nerve.
Assessment of Study Quality
The mean MCMS score was 34.8 (range, 24-59) demonstrating the quality of the studies to be poor (Table 1). The intraclass correlation coefficient value between the mean values of the MCMS calculated between the 2 authors was excellent (0.915).
Discussion
The results of this systematic review identified isolated, full-thickness proximal rectus femoris injuries in 132 athletes from 18 studies. The injuries occurred most frequently in men participating in soccer and rugby, with kicking and excessive knee flexion and forced hip extension being the most common mechanisms of injury. Operative management was performed in 80% of athletes, most commonly consisting of primary repair. All (100%) athletes undergoing operative management and 93% of athletes treated nonoperatively reported successful RTP at their preinjury level. Mean time to RTP was nearly twice as long for athletes treated operatively (22 weeks) compared with those undergoing nonoperative management (12 weeks). Complications were reported in 18% of athletes undergoing operative management, consisting primarily of LFCN neurapraxia, LFCN injury and recurrent injury to the proximal rectus femoris.
Reported management for proximal rectus femoris injuries primarily involves operative treatment, as 80% of cases reported in the literature were managed surgically. Operative management has been indicated in the setting of avulsion injuries with displacement >20 mm, 27 severe functional deficits on physical examination, 4 and patient-specific goals to return to elite or high-level athletic activities. 14,29 Some athletes with failed nonoperative management have been shown to improve and RTP successfully after surgical repair. Namely, Straw et al 29 reported failed nonoperative treatment in a soccer player with inability to sprint or kick a ball after 12 months. Subsequent surgical repair allowed for successful RTP at preinjury level 6 months after surgery. Huri et al 14 reported successful surgical repair of a proximal rectus femoris avulsion in a professional soccer player after 24 months of failed nonoperative management. It should be noted that there are currently no prospective randomized studies comparing operative and nonoperative management for this injury in athletes. Therefore, clinicians contemplating the treatment of athletes with this injury must understand that the indications for surgery are based on expert opinion and subjective factors rather than purely objective criteria established through prospective controlled studies.
Operative management is also recommended in the setting of more severe injuries. Specifically, Lempainen et al 21 reported acute repair in the setting of magnetic resonance imaging (MRI) demonstrating retraction of both direct and indirect tendon heads. Kayani et al 17 recommended acute repair only in athletes with a “higher-than-acceptable” risk of injury recurrence based on the British Athletics Muscle Injury Classification (BAMIC) system determined by MRI. The BAMIC system classifies muscle injury based on severity of injury, where grade 0 has no MRI findings, grade 1 is characterized by a small tear to the muscle, grade 2 has a moderate muscle tear, grade 3 has a more extensive muscle tear, and grade 4 is characterized by a complete tear to the muscle or a tendon avulsion. BAMIC grade 4 avulsion injuries of the straight head of the proximal rectus femoris were considered higher-than-acceptable risk of injury recurrence. 17 As such, operative treatment may have some advantages in competitive athletes, especially in the setting of severe, retracted injuries involving both heads of the proximal rectus femoris, as well as in athletes with inability to RTP after attempted nonoperative management. 14 However, further studies are warranted to better determine which athletes and injury variables best determine the success of operative versus nonoperative management of these injuries, as well as when to proceed from nonoperative to operative treatment.
Timing of RTP for athletes undergoing operative management was 22.1 weeks, compared with 11.7 weeks for athletes treated nonoperatively. This finding corresponds with the results reported by Dalal et al 6 in their analysis of 9 studies (N = 82 patients), observing that athletes who underwent nonoperative management returned at a faster rate (69.2 days) compared with athletes who underwent operative management (112.6 days). Furthermore, the authors reported a RTP rate of 95% in the operative group versus 92.7% in the conservative treatment group (P = .93). 6 Our review of the literature found a 100% RTP rate in athletes treated operatively compared with 93.3% of athletes treated nonoperatively. Athletes undergoing operative treatment had a higher RTP rate but longer convalescence compared with those athletes managed nonoperatively. This finding is likely due to a variety of reasons in athletes undergoing surgery, such as the time needed to allow for surgical wound healing, the pain inherent in surgical intervention, and the necessity of a course of postoperative rehabilitation to restore muscle strength and function. It is possible that the literature is biased toward surgical treatment, which makes it difficult to interpret the comparison with nonoperative treatment. Moreover, operative management may be reserved for patients in whom nonoperative management had previously failed or was insufficient. 14,21,29 Obviously, operative repair requires prolonged healing times when compared with nonoperative care due to initial immobilization, as García et al 12 reported knee immobilization for 1 week as part of their postoperative rehabilitation whereas Angers-Goulet et al 1 reported knee immobilization for 10 days postoperatively. Additional investigations are warranted to compare operative and nonoperative treatment of this injury, as well as to evaluate the patient- and injury-specific variables dictating the timing and success of RTP.
Limitations
This study was not without limitations. The small sample size and poor MCMS score is related to the low incidence of reported proximal rectus femoris injuries occurring in athletes in the literature. As such, the poor MCMS score is a result of the included studies with evidence levels of 3 to 5, as the MCMS criteria lead to higher scores in large, randomized, prospective studies, of which none are currently present in the literature. Moreover, the studies included in this systematic review were largely limited to small case series and retrospective reviews, further limiting the generalizability of outcomes to nonathletes, emphasizing the necessity for higher quality investigations in larger patient populations. As mentioned, there is clearly a selection bias toward reporting surgical treatment of athletes sustaining proximal rectus femoris injuries. Due to the heterogeneity of patient-reported outcome measures and the small sample size of nonoperatively treated patients, we were unable to perform any meaningful statistical analyses evaluating outcomes based on injury management. In addition, there were no objective rating scales or accepted patient-reported outcome measures on which to base the success of treatment. Furthermore, due to the small number of identified studies, we elected to include studies reporting data with less than 2-year follow-up. Finally, based on the inherent limitations of systematic reviews, indications and justifications for operative versus nonoperative management were not always reported, limiting our ability to define criteria validating 1 treatment over the other. Further high-quality investigations are necessary to better determine the indications for surgery and both subjective and objective outcomes following treatment of proximal rectus femoris tears.
Conclusion
Full-thickness proximal rectus femoris injuries occurred most frequently in athletes participating in soccer and rugby secondary to explosive, eccentric contractions involved in kicking and sprinting. Operative management was performed in the majority of cases reported in the literature. Athletes undergoing operative repair had a 100% RTP rate versus 93.3% in athletes treated nonoperatively.