
Abstract
Background:
While sex-based differences in outcomes after hip arthroscopic surgery for femoroacetabular impingement syndrome (FAIS) are often recorded, no studies have been dedicated to analyzing the literature as a whole.
Purpose:
To investigate whether sex is a predictor of outcomes in studies evaluating hip arthroscopic surgery for FAIS.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. We searched the PubMed, Embase, Cochrane, Ovid, and PubMed Central databases for English-language studies that evaluated sex-specific outcomes in human populations. The search terms used were as follows: (“Hip Arthroscopy”) AND (“Femoroacetabular Impingement” OR “FAI”) AND (“Sex” OR “Gender” OR “Male” OR “Female”). Studies with evidence levels 2 through 4 were included. The studies were then screened, followed by data extraction. Modified Harris Hip Score (mHHS) outcomes and return-to-sport (RTS) rates were recorded. These were analyzed using random-effects meta-analysis. Heterogeneity was calculated using the I 2 statistic.
Results:
Of 256 full-text articles screened, 48 articles were included in this analysis; of these, 14 studies (29%) concluded that female sex was a negative predictor of postoperative outcomes, while 6 studies (13%) found female sex to be positive predictor. The remaining 28 studies (58%) found no sex-based differences in postoperative outcomes. Of 7 studies (416 male and 519 female) included in the mHHS analysis, 2 studies concluded that male patients had significantly higher postoperative mHHS scores. Of 6 studies (502 male and 396 female) included in the RTS analysis, 1 study concluded that male patients had a significantly higher RTS rate.
Conclusion:
Almost one-third of the included studies determined that female sex was a negative predictor of postoperative outcomes, 13% found female sex to be a positive predictor, and 58% found no sex-based differences. Our study illustrates an insufficiency of high-level evidence supporting sex-specific differences in outcomes after hip arthroscopic surgery, but findings indicated that the postoperative mHHS score and RTS rate may be influenced by sex.
Femoroacetabular impingement syndrome (FAIS) is increasingly diagnosed and treated in patients of all age groups. 49 These bony impingements present as cam, pincer, or combined morphologies that can severely affect hip function. FAIS treatment is particularly of interest in young athletes because of its hindrance on their performance and lengthy recovery time. 6
Over the past 3 decades, hip arthroscopic surgery has become the leading surgical treatment for FAIS. Hip arthroscopic surgery has proven to lower morbidity, decrease recovery time, and lower complication rates compared with open approaches. 4 Review articles in the literature have addressed the predictors of hip arthroscopic surgery failure as well as approaches to treatment after failure, 35,51 but none has reviewed the literature exclusively looking at sex-based outcomes.
Evaluating sex-based outcomes is important because we often find disparities regarding sex in medicine. 50 This exploration can also serve as a platform from which to discuss the reason for disparities to appropriately address them. Research focusing on female-specific outcomes has historically been excluded from sports science and sports medicine. Although the sports medicine literature has made great strides in generating inclusive studies, the current landscape still fails to reflect the continued increase in the popularity of female sports. 50
More specifically, exploring outcomes regarding sex is important to understand the cause of FAIS and the response to treatment of those undergoing hip arthroscopic surgery. The literature has presented differing findings on the predictive value of sex. 11,39,40,51 While studies have found different cam- or pincer-type lesion rates, degrees of dysplasia, and alpha angles between men and women, our goal was to exclusively analyze outcomes purely through the lens of sex. This study is a systematic review of the literature regarding sex-based outcomes of hip arthroscopic surgery for FAIS.
Methods
Search Strategy and Study Selection
A systematic review of the literature was performed using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 32 The search was performed using PubMed, Embase, Cochrane, Ovid, and PubMed Central databases. The search terms applied were as follows: (“Hip Arthroscopy”) AND (“Femoroacetabular Impingement” OR “FAI”) AND (“Sex” OR “Gender” OR “Male” OR “Female”). All articles fitting the search terms up to November 15, 2021, were reviewed. Screening was performed by 2 reviewers (T.J.M. and M.L.V.). After initial screening, a consensus between the reviewers determined the final inclusion of studies. Duplicates were removed using EndNote reference management software (Clarivate). The remaining studies were then filtered using inclusion and exclusion criteria. Inclusion criteria were as follows: English language, human studies, and studies evaluating sex-specific outcomes. Exclusion criteria were as follows: animal studies, cadaveric studies, review studies/systematic reviews, commentaries, letters to the editor, studies not evaluating sex-specific outcomes, studies including other associated injuries and isolated cartilage damage (ie, associated chondroplasty and microfracture), studies including revision, and studies including open procedures (eg, periacetabular osteotomy and adjunctive femoral osteotomy). Filtering took place first through abstract and title screening and then through a full-text review.
The selection was initially intended to only include level of evidence 1 and 2 studies, but after search criteria were applied, it became evident that we would need to include level 3 and 4 studies. This decision is reported and analyzed in the following Results and Discussion sections.
Data Extraction
The following data were extracted from each article if reported: number of patients (subdivided by sex), age, body mass index, follow-up in months, procedures performed, surgical technique, number of athletes, level of competition, sport type, position in sport, functional outcome measures, minimal clinically important difference, lateral center-edge angle (or alpha angle), sexual activity, satisfaction, osteoarthritis progression, procedure survival time, joint space width, return-to-sport (RTS) duration, RTS percentage, return to activity, conversion to total hip arthroplasty, revision rate, and complications.
Quality-of-Bias Assessment
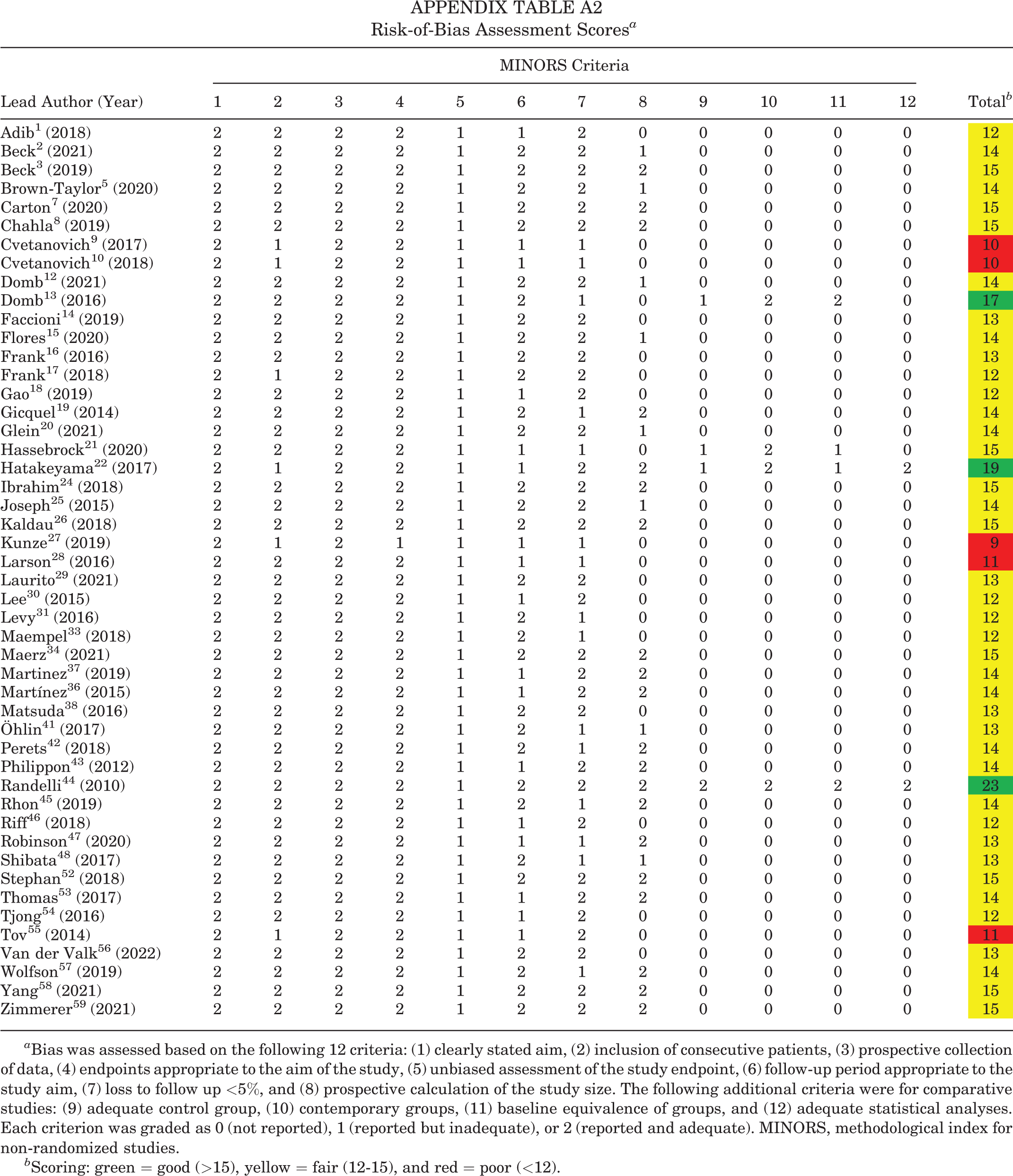
A quality-of-bias assessment was conducted using the methodological index for nonrandomized studies (MINORS). This was accomplished by analyzing each study using 12 separate criteria. Each score was then tallied and categorized by its inherent risk of bias on a graded scale in which a score of 0 indicates that the item was not reported, a score of 1 denotes that the item was reported but inadequate, and a score of 2 indicates that the item was reported and adequate. The global ideal score for the MINORS criteria is 16 for noncomparative studies and 24 for comparative studies. For our assessment, scores >15 were considered good, scores from 12 to 15 were considered fair, and scores <12 were considered poor.
Statistical Analysis
Because of the prevalence of studies that reported modified Harris Hip Score (mHHS) outcomes and RTS rates, these studies were included in a separate review. They were analyzed using random-effects meta-analysis. The mean difference, along with the 95% CI, was calculated for postoperative mHHS scores. For RTS rates, the odds ratio (OR) and 95% CI were calculated. Heterogeneity was examined using the I 2 statistic. 23 P < .05 was considered significant. Heterogeneity was found to be too high for the mHHS and RTS to appropriately analyze and include. R (Version 3.6.3; R Core Team) was used for all statistical analyses. Forest plots were generated to report both mHHS and RTS results.
Results
Characteristics of Included Studies
The literature search results can be observed in Figure 1. After search terms were applied, 13,340 articles were identified. After title and abstract screening, 256 were left for a full-text review. At the conclusion of the search, 48 studies were included in the qualitative synthesis, while a total of 13 studies were included in the mHHS 9,15,16,20,43,48,55 and RTS 13,20,46,48,53,54 analyses. Most studies (176/256 [68.8%]) were excluded during the full-text review because they lacked a sex-based comparison of functional outcomes. A summary of the 48 included studies is shown in Appendix Table A1, and a summary of study bias according to MINORS criteria is included in Appendix Table A2.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study selection.
The 48 studies comprised 11,698 hips, with 6066 being male (51.9%) and 5632 being female (48.1%). A wide range in patient characteristics was seen among the studies. For example, patient ages ranged from 10 to 76 years. There were 1185 athletes; however, only 898 (75.8%) were able to be stratified by sex: 502 male (55.9%) and 396 female (44.1%). The studies that categorized athletes by sex reported the following sports for their participants: hockey, football, baseball, softball, soccer, track, water polo, triathlon, lacrosse, tennis, gymnastics, basketball, running, dancing, golf, volleyball, swimming, rowing/crew, rugby, fencing, field hockey, bobsled, weight lifting, wrestling, and high-intensity interval training.
A wide range of outcome measures was used in the studies. The following are functional outcomes that were subdivided by sex in ≥2 studies: Hip Outcome Score–Activities of Daily Living (HOS-ADL), 2,3,8,9,15,16,25,27,31 Hip Outcome Score–Sports Specific, 2,3,8,9,16,20,27,31 mHHS, § 12-item international Hip Outcome Tool, 27,33,41,47 33-item international Hip Outcome Tool, 5,25,48 EuroQol–5 Dimensions, 26,33,47 and visual analog scale for pain or satisfaction. 2,3,8,20,33,47 Overall, 14 studies in the qualitative analysis indicated that female sex, according to various measures, was a negative predictor of outcomes after hip arthroscopic surgery for FAIS. ∥ In comparison, 6 studies found that female sex was a positive predictor of outcomes. 2,7,9,15,31,45 The remaining 28 studies either concluded that sex did not significantly affect outcomes or that there were not enough data to support this claim.
Analysis of mHHS and RTS
The 7 studies 9,15,16,20,43,48,55 included in the mHHS analysis comprised 416 male and 519 female patients. Because of heterogeneity of the data (I 2 = 51%), these outcomes could not be pooled. There were 2 studies that found male patients to have a significant increase in the mHHS score compared with female patients postoperatively. 16,43 The remaining studies found the difference to be nonsignificant. A forest plot presenting mHHS outcomes is seen in Figure 2. The 6 studies 13,20,46,48,53,54 included in the RTS analysis comprised 502 male and 396 female patients. As with the mHHS analysis, heterogeneity was too high (I 2 = 71%) to pool the outcomes. One study found male patients to have a higher RTS rate. 53 The remaining studies found the difference to be nonsignificant. A forest plot presenting RTS outcomes is shown in Figure 3.


Discussion
The major findings of our study are that when observing different outcomes, both male and female sexes were found to be a positive or negative predictor of success after hip arthroscopic surgery for FAIS. With 14 of the 48 studies included in the systematic review concluding female sex as a negative predictor, it could be determined that sex may play a role in postoperative outcomes. While some articles in the qualitative review suggested female sex as a negative predictor, 58% of the included studies could not find a statistical difference in the 2 sexes regarding outcomes. These results were somewhat limited by the insufficient literature and heterogeneity of the data, highlighted by the fact that approximately 70% of the studies had a level of evidence of ≥3. Also, this is emphasized by the I 2 values from the mHHS (51%) and RTS (71%) analyses.
The greatest factor contributing to this high heterogeneity was the lack of randomization throughout the studies. In our assessment of the risk of bias using the MINORS criteria, only 3 comparative studies were given an adequate rating for the baseline equivalence of groups: Domb et al 13 , Hatakeyama et al 22 , and Randelli et al. 44 Because of this lack of randomization, pooling the data for analysis was not reliable.
Interestingly, 2 studies highlighted the finding that female patients aged ≥45 years fared worse after surgery than their male counterparts. 3,16 Beck et al 3 stratified their study cohort by age and sex and determined that female patients aged ≥45 years scored consistently lower than every other sex/age group on the HOS-ADL, HOS-SS, and mHHS while also having the highest pain score. Similarly, Frank et al 16 categorized their study population by sex and age, also finding that female patients aged >45 years scored significantly lower than all other groups when looking at the same outcomes as Beck et al. 3 That study noted that in the age group <45 years, female patients fared as well as male patients in terms of functional outcome scores. Throughout the literature, age was often presented as a negative predictor of outcomes for both male and female patients. 2,16,59
There are 2 previous systematic reviews worth noting: Minkara et al 39 and Sogbein et al 51 both touched on sex as a predictor of outcomes after hip arthroscopic surgery. Minkara et al mentioned male sex to be associated with higher postoperative mHHS scores as well as a higher risk of labral tears and acetabular chondromalacia. That study contrasted these results to female sex, which they linked to less severe cam-type deformities but also a higher risk of persistent pain after surgery, requiring second-look hip arthroscopic surgery. Overall, Minkara et al claimed that their review is consistent with the notion that female sex is a risk factor associated with hip arthroscopic surgery. Sogbein et al also mentioned an array of studies linking negative outcomes to female sex, but they found men to be more likely to undergo subsequent total hip arthroplasty than women (44% vs 20%, respectively; P = .002). While we recognize some of the same mixed results of these 2 reviews, it is also important to acknowledge that these reviews were analyzing outcomes in relation to many factors, not only sex. We believe that our sex specific–based analysis shows a more heterogeneous picture than some of their more anecdotal claims.
It is important to discuss the studies that found female sex to be a positive predictor of outcomes. 7,9,28,44 Carton and Filan 7 found that for the 36-item Short Form Health Survey (SF-36), which reviews quality-of-life measures, female sex was a significant clinical predictor of achieving the minimal clinically important difference (OR, 0.121 [95% CI, 0.026-0.568]; P = .007). Carton and Filan was the only study that used the SF-36. Cvetanovich et al 9 presented in their results that female patients in the borderline dysplastic group had greater improvements in both HOS-ADL (P = .05) and mHHS (P = .005) scores compared with their male counterparts in the borderline dysplastic group. Levy et al 31 discovered in their case series that in those who identified as recreational or competitive runners, female patients had a greater improvement in HOS-ADL scores compared with male runners (28.8 ± 17.5 vs 13.8 ± 10.5, respectively; P = .001). Last, Rhon et al, 45 who included 1870 participants, found that male sex was a predictor of osteoarthritis within 2 years of hip arthroscopic surgery for FAIS (OR, 1.31 [95% CI, 1.04-1.65]). While more articles suggested male sex as a positive predictor of outcomes, it is worth acknowledging the differing results in these studies.
Some studies stood alone because of their exploration of unique outcomes. Kunze et al 27 focused on the sleep quality of patients after surgery. They found no difference in the mean Pittsburgh Sleep Quality Index at any point after surgery between the sexes. Data were collected at 3, 6, 12, and 24 months postoperatively. Lee et al 30 aimed to compare sexual functional outcomes between male and female patients. Their study found that female patients returned to sexual activity later (34.8 ± 23.2 vs 21.0 ± 10.7 days, respectively; P < .0001), more male patients reported an increase in sexual activity postoperatively (61.9% vs 38.1%, respectively; P < .0001), and female patients reported more alterations in sexual positioning (82.3% vs 17.7%, respectively; P < .0001). Thomas et al 53 were unique in that they calculated the rate of return to duty in a military population as opposed to RTS, which was frequently examined in other articles. In a case series of 469 participants, Thomas et al found that 45% of men were able to return to duty, while only 26% of women were able to do the same (P < .0001). Finally, Brown-Taylor et al 5 described sagittal- and frontal-plane gait mechanics postoperatively. This provided physicians with insight on sex-specific gait impairments that can affect outcomes. While these studies started interesting conversations on hip arthroscopic surgery and FAIS, it is clear that there is a need for more standardized measures to reach proper conclusions.
Limitations
There are several limitations to this study, including the lack of control for other associated surgical procedures, such as labral repair or debridement. While there is a plethora of data regarding outcomes after hip arthroscopic surgery for FAIS, relatively few studies aimed to compare sex-based differences. Therefore, the data that can be extracted from the literature are quite heterogeneous and lack a clear functional outcome standard to be applied. A small portion of the studies included in the review did not provide raw data regarding sex-based outcomes, simply reporting that there was no significant difference between the 2. This lack of transparency could introduce a number of biases. Also, some of the studies included had relatively small sample sizes, which could lead to selection bias.
Conclusion
While many studies found no difference or conclusive evidence when comparing sex-based outcomes after hip arthroscopic surgery, almost one-third of the included studies determined that female sex was a negative predictor of postoperative outcomes. In 13% of the included literature, female sex was determined to be a positive predictor. This study illustrates an insufficiency of high-level evidence evaluating sex-based outcomes after hip arthroscopic surgery but also shows the beginning of our understanding of sex-specific medicine. Further literature with more standardized measures is needed to evaluate the difference in postoperative outcomes in terms of sex.
Footnotes
Notes
Final revision submitted August 21, 2022; accepted August 30, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.L.V. has received education payments from Titan Surgical Group and hospitality payments from DePuy and Zimmer Biomet. M.K.M. has received education payments from Arthrex, Alon Medical Technology, and Quest Medical and nonconsulting fees from Arthrex. J.P.S. has received education payments from Arthrex and Titan Surgical Group, consulting fees from Vericel, and hospitality payments from Zimmer Biomet. B.G.V. has received education payments from Titan Surgical Group and consulting fees from DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethics approval was not required for this study.
APPENDIX
Risk-of-Bias Assessment Scores a
| Lead Author (Year) | MINORS Criteria | Total b | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| Adib 1 (2018) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Beck 2 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Beck 3 (2019) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Brown-Taylor 5 (2020) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Carton 7 (2020) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Chahla 8 (2019) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Cvetanovich 9 (2017) | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 10 |
| Cvetanovich 10 (2018) | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 10 |
| Domb 12 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Domb 13 (2016) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 1 | 2 | 2 | 0 | 17 |
| Faccioni 14 (2019) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 13 |
| Flores 15 (2020) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Frank 16 (2016) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 13 |
| Frank 17 (2018) | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Gao 18 (2019) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Gicquel 19 (2014) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 14 |
| Glein 20 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Hassebrock 21 (2020) | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 1 | 2 | 1 | 0 | 15 |
| Hatakeyama 22 (2017) | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 19 |
| Ibrahim 24 (2018) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Joseph 25 (2015) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 1 | 0 | 0 | 0 | 0 | 14 |
| Kaldau 26 (2018) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Kunze 27 (2019) | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 9 |
| Larson 28 (2016) | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 11 |
| Laurito 29 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 13 |
| Lee 30 (2015) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Levy 31 (2016) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 12 |
| Maempel 33 (2018) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | 0 | 12 |
| Maerz 34 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Martinez 37 (2019) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 14 |
| Martínez 36 (2015) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 14 |
| Matsuda 38 (2016) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 13 |
| Öhlin 41 (2017) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 13 |
| Perets 42 (2018) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 14 |
| Philippon 43 (2012) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 14 |
| Randelli 44 (2010) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 23 |
| Rhon 45 (2019) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 14 |
| Riff 46 (2018) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Robinson 47 (2020) | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 13 |
| Shibata 48 (2017) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 13 |
| Stephan 52 (2018) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Thomas 53 (2017) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 14 |
| Tjong 54 (2016) | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 12 |
| Tov 55 (2014) | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 11 |
| Van der Valk 56 (2022) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 13 |
| Wolfson 57 (2019) | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 0 | 0 | 14 |
| Yang 58 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
| Zimmerer 59 (2021) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | 15 |
a Bias was assessed based on the following 12 criteria: (1) clearly stated aim, (2) inclusion of consecutive patients, (3) prospective collection of data, (4) endpoints appropriate to the aim of the study, (5) unbiased assessment of the study endpoint, (6) follow-up period appropriate to the study aim, (7) loss to follow up <5%, and (8) prospective calculation of the study size. The following additional criteria were for comparative studies: (9) adequate control group, (10) contemporary groups, (11) baseline equivalence of groups, and (12) adequate statistical analyses. Each criterion was graded as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). MINORS, methodological index for non-randomized studies.
b Scoring: green = good (>15), yellow = fair (12-15), and red = poor (<12).