
Abstract
Background:
Sexual difficulties and dysfunction are common in patients with femoroacetabular impingement syndrome (FAIS) secondary to hip pain and stiffness.
Purpose:
To determine the risk of impingement in patients with FAIS during common sexual positions using 3-dimensional computer-simulated collision detection before and after cam correction.
Study Design:
Descriptive laboratory study.
Methods:
Ten computed tomography scans of the pelvis and femur from patients with FAIS due to isolated cam morphology were retrospectively reviewed. Three-dimensional osseous models were developed using Mimics software. The cam deformity was then completely corrected. Simulations of hip range of motion for the most common sexual positions for men (n = 15) and women (n = 14) were conducted before and after cam resection. Impingement was determined for each sexual position. Position safety was defined as ≤20% of models demonstrating impingement in a position. Descriptive and simple comparative statistics were calculated.
Results:
There was no sexual position that was impingement free in all models before cam correction. After cam correction, 11 (37.9%) of 29 total positions were impingement free. There was a significant decrease in impingement from before to after cam correction (40.7% vs 11.4%, respectively, of all female positions [P < .0001]; 26.0% vs 6.7%, respectively, of all male positions [P < .0001]). There was a significant increase in the number of “safe” positions from before to after cam correction (4 vs 11, respectively, of all female positions [P = .008]; 7 vs 15, respectively, of all male positions [P = .001]).
Conclusion:
After cam correction, there was a significant reduction in the impingement rate and a significant increase in the number of “safe” sexual positions.
Clinical Relevance:
Impingement in patients with cam morphology is common during sexual activity. Surgical correction of cam morphology significantly reduces the rate of impingement. Although this laboratory imaging-only study did not account for patient symptoms, this likely translates to significant symptomatic improvement during sexual activity after surgical cam correction.
Femoroacetabular impingement syndrome (FAIS) is a common cause of hip pain. FAIS represents premature contact between the proximal femur and acetabulum secondary to cam and/or pincer morphology. 10 The primary symptom of FAIS is motion- or position-related pain in the hip or groin. 10 Thus, during activities of daily living, sports, or any activity requiring deep flexion and rotational motions and/or positions, symptoms may present or progress. The hips and pelvis are an integral component of sexual activity and function. 11,13,15 Therefore, FAIS may negatively affect sexual activity and affect the lives of a large number of people. 6 The sensitive nature of the topic may preclude adequate communication between a patient and clinician to provide an accurate, timely diagnosis and treatment.
A recent study demonstrated that 66% of patients with FAIS reported sexual difficulties secondary to pain (78%), stiffness (47%), and loss of interest (21%). After arthroscopic hip preservation surgery (including cam correction), this improved to only 10.8% with sexual dysfunction. 13 After surgery, 88.9% of patients had relief of pain. Although multifactorial, a large proportion of the symptomatic improvement after cam correction is caused by the improved femoral head-neck offset and biomechanics, permitting greater degrees of impingement-free motion and positioning. 3
A recent computer simulation study (based on 2 young, healthy volunteers’ in vivo simulation) showed that sexual positions with excessive hip flexion increase the risk of impingement after total hip arthroplasty (THA). 5 Computer-simulated 3-dimensional (3D) collision detection models have also been used to estimate the risk of impingement during activities in several studies in patients with cam and/or pincer morphology. 3,4,16,17 However, no study has examined the risk of impingement during sexual positions in patients with FAIS due to cam morphology using 3D-modeled computer simulation.
The purpose of this study was to determine the risk of impingement in patients with FAIS during common sexual positions using 3D computer-simulated collision detection before and after cam correction. We hypothesized that sexual positions with excessive hip flexion (>75°) would increase the risk of FAIS and that the rate of impingement would decrease after cam resection.
Methods
Institutional review board approval was obtained for this retrospective study of patients with FAIS (triad of patient symptoms, clinical signs, and imaging findings) due to isolated (no pincer or subspine impingement, no dysplasia, no arthritis) cam morphology (alpha angle on Dunn 45° plain radiographs >55°) and labral injuries, who underwent hip arthroscopic surgery by a single sports medicine fellowship–trained orthopaedic surgeon (J.D.H.). Patients with FAIS who had completed a minimum 3-month course of nonsurgical treatment (including rest, activity modification, physical therapy, education, oral anti-inflammatory nonnarcotic medications, or intra-articular injections [local anesthetic diagnostic with or without corticosteroid therapeutic]) and were dissatisfied with their hip condition were eligible for arthroscopic hip preservation surgery. 10 Patients with advanced arthritis (Tönnis grade >1 or joint space <2 mm), more than borderline dysplasia (lateral and/or anterior center-edge angle <20°, Tönnis angle >15°, femoral head extrusion index >25%, and/or broken Shenton line), femoral head avascular necrosis, synovial chondromatosis (and osteochondromatosis), or septic arthritis were excluded. 10 Those who had undergone previous open or arthroscopic hip surgery were also excluded.
Patients underwent preoperative computed tomography (CT) of the pelvis and femur with 0.625-mm section thickness using the LightSpeed VCT 64 Slice Scanner (GE Healthcare) and a low–radiation dose protocol. Radiographic parameters were assessed and measured independently by a single sports medicine fellowship–trained orthopaedic surgeon specializing in hip arthroscopic surgery (J.D.H.). Three-dimensional osseous models of the pelvis and femur were developed from the CT scans using Mimics software (Materialise) for each patient according to previously published methods. 4 Virtual surgical cam correction was then performed using Mimics software. Bone was resected at the femoral head-neck junction to establish sphericity, creating 2 models (before correction and after correction) for each patient (Figures 1 and 2). Coordinate systems were established for the pelvis and femur based on anatomic landmarks with x (flexion/extension), y (abduction/adduction), and z (internal rotation/external rotation) axes.

Three-dimensional osseous model of the hip before cam resection.
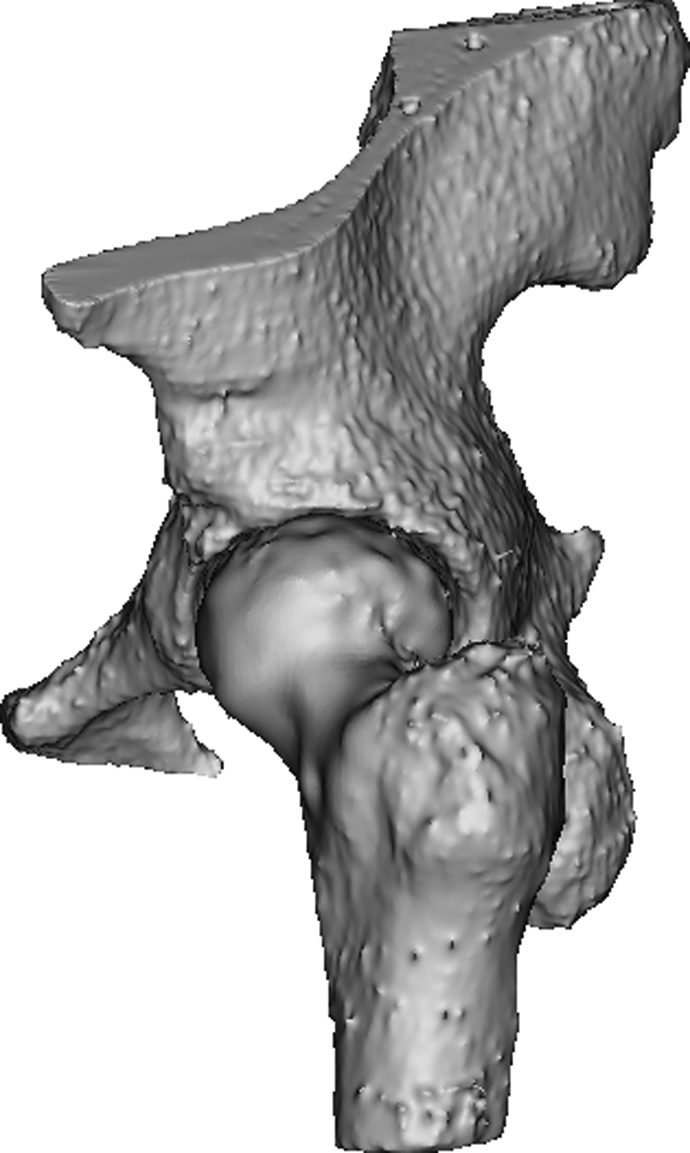
Three-dimensional osseous model of the hip after cam resection.
Hip range of motion (ROM) for the most common sexual positions for women (n = 14) (Table 1) and men (n = 15) (Table 2) was identified based on previous research. 5,7 Charbonnier et al 5 utilized 2 young, healthy volunteers (aged 31 and 26 years) in a single motion-capture session with 14 mm–diameter skin-applied adhesive markers. There were 12 total positions utilized, and all were treated as symmetric regarding the exact ROM for each side (right vs left), with the exception of 3 positions for male patients and 2 positions for female patients. This accounted for 15 total male positions (10 models; 150 total simulations) and 14 total female positions (10 models; 140 total simulations) analyzed. Simulations of hip ROM for each position were conduced using the computerized software for each CT scan before and after cam correction. All 10 hip models were simulated through both the male and the female positions. Femoral head center of rotation was kept static. Impingement was determined (yes/no) if the femur contacted the acetabulum during simulated hip ROM for each position (Figure 3). To describe and report the exact location of the impingement zone, the acetabulum was divided into 8 sectors (superior, anterosuperior, anterior, anteroinferior, inferior, posteroinferior, posterior, and posterosuperior) (Figure 4). A position was defined as “safe” (ie, low risk of impingement) if ≤20% of the 10 analyzed hip models demonstrated impingement for that position. A position was defined as “impingement free” if none of the 10 analyzed hip models demonstrated impingement for that position. Descriptive statistics were calculated. Impingement before resection and after resection was compared using chi-square tests.
Hip Range of Motion During Sexual Positions for Women

Hip Range of Motion During Sexual Positions for Men

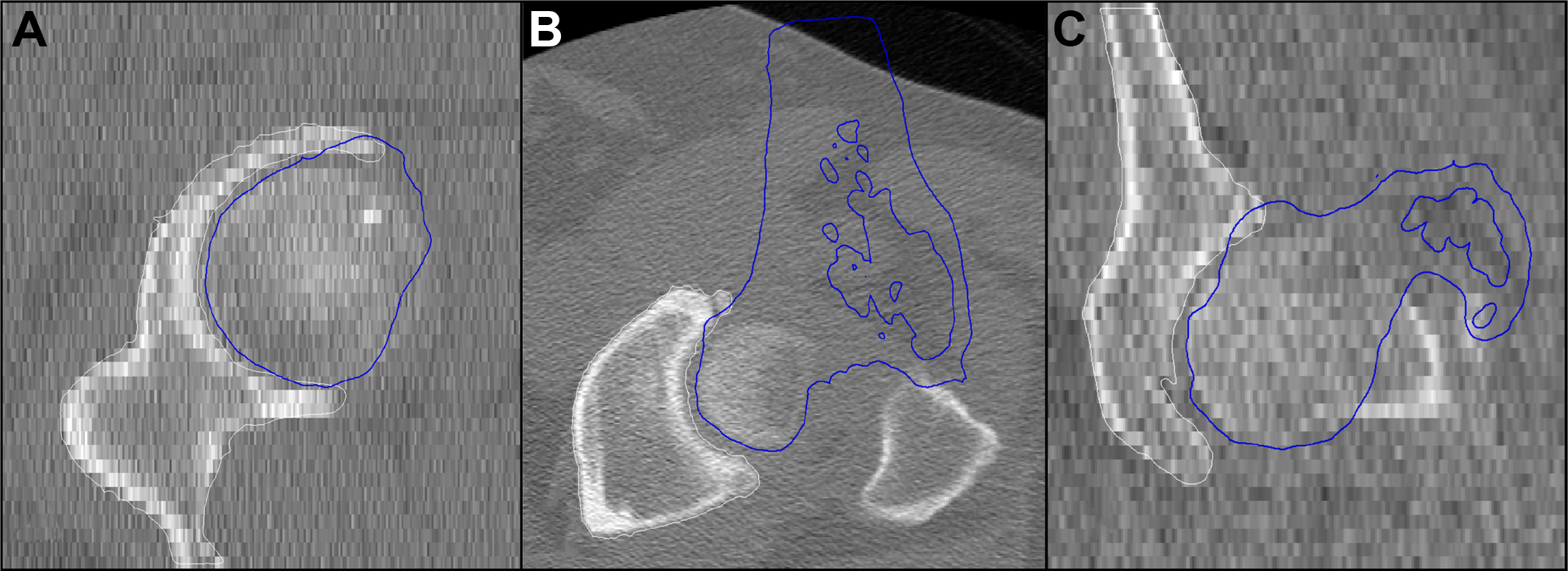
Model of the hip demonstrating impingement in the (A) sagittal, (B) axial, and (C) coronal planes with the femur (blue) crossing over the acetabulum (white).

Acetabular zones of impingement.
Results
There were 5 left and 5 right hips analyzed (mean age, 32.1 ± 11.3 years) (Table 3). Impingement occurred in at least 1 position in 8 (80.0%) of the 10 models before cam correction. There was no position that was impingement free in all 10 models. Before cam correction, there were 4 (28.6%) of 14 positions in female patients and 7 (46.7%) of 15 positions in male patients that were deemed “safe” and unlikely to cause impingement (Tables 4 and 5). Overall, more female position simulations (57/140; 40.7%) demonstrated impingement compared with male position simulations (39/150; 26.0%) (P = .009). Most impingement was observed in female positions that required high hip flexion (Table 4). Impingement occurred in the anterior (59.6%), anterosuperior (31.6%), and superior (8.8%) acetabulum. Similarly, for male positions, most impingement was observed in positions that required high hip flexion (>75°) (Table 5). Impingement occurred in the anterior (87.2%), superior (7.7%), and anterosuperior (5.1%) acetabulum.
Patient Radiographic Parameters a

a Values are presented as mean ± SD unless otherwise indicated.
Impingement During Sexual Positions for Women a

a Asterisks indicate a “safe” position.
Impingement During Sexual Positions for Men a
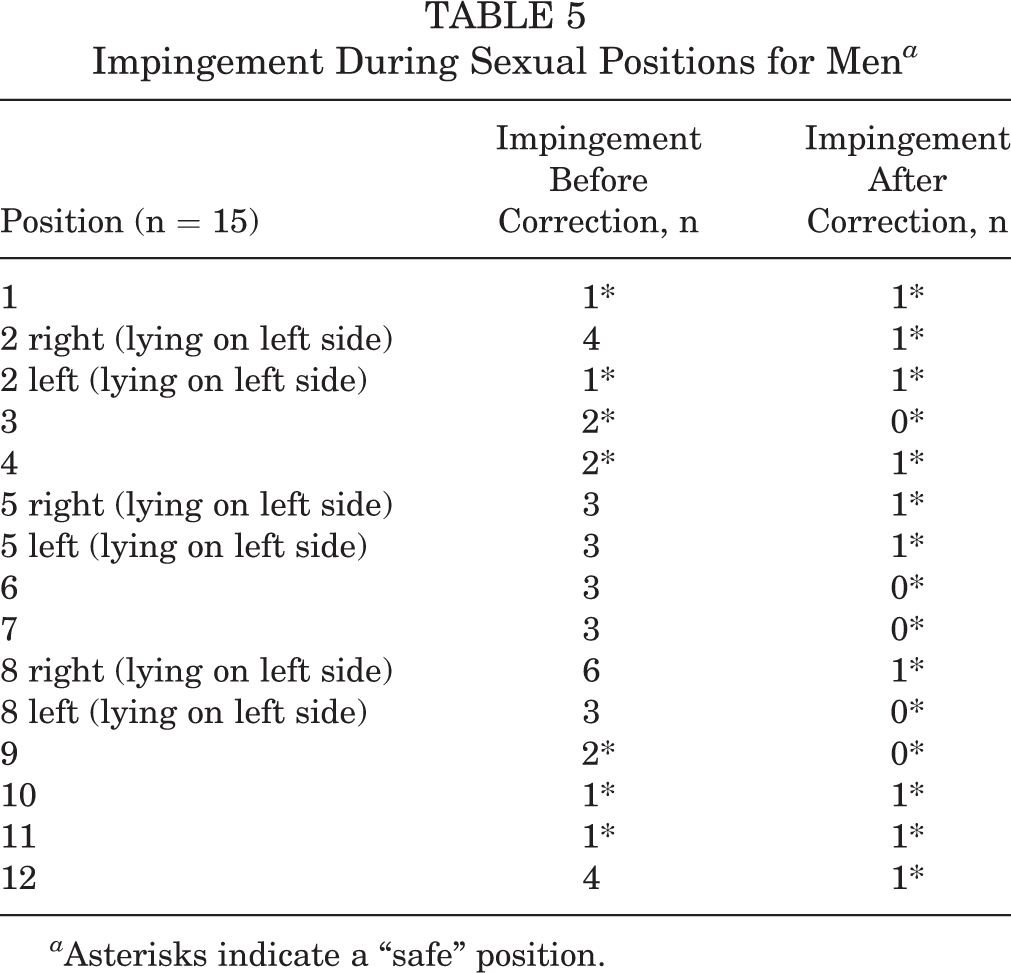
a Asterisks indicate a “safe” position.
After cam correction, impingement occurred in at least 1 position in 5 (50.0%) of the 10 models. Eleven (6/14 female, 5/15 male; 37.9%) positions were impingement free after correction (vs 0 before correction) (Tables 4 and 5). There were 11 (78.6%) of 14 positions in female patients and 15 (100.0%) of 15 positions in male patients that were deemed “safe” and unlikely to cause impingement (Tables 4 and 5). There was a significant increase in the number of “safe” positions from before to after cam correction in both female positions (4 vs 11, respectively; P = .008) and male positions (7 vs 15, respectively; P = .001). After cam correction, there was a significant reduction in the number of both female position simulations demonstrating impingement (16/140; 11.4%; P < .0001) and male position simulations demonstrating impingement (10/150; 6.7%; P < .0001). Most impingement was observed in female positions that required high hip flexion. Impingement occurred only in the anterior (100.0%) acetabulum.
Discussion
FAIS occurred in 80% of the 3D hip models with isolated cam morphology during common sexual positions in this collision-detection investigation. After cam correction, there was a significant reduction in the impingement rate and a significant increase in the number of “safe” male and female positions. All male positions and 78.6% of female positions tested were likely safe after cam correction. Both before and after cam correction, positions with excessive flexion were at highest risk for impingement. This confirmed our hypothesis that sexual positions with excessive hip flexion (>75°) would increase the risk of impingement and that the rate of impingement would significantly decrease after cam correction.
No prior study has evaluated the risk of impingement during common sexual positions in patients with FAIS. However, analysis of the impingement risk in patients after THA (based on motion analysis in young, healthy volunteer nonarthroplasty hips) demonstrated that sexual positions requiring excessive hip flexion (>95°) were associated with an increased risk of impingement. 5 The trend was similar in the current investigation, as the sexual positions requiring increased hip flexion for female and male patients were at an increased risk for impingement before cam correction. However, impingement occurred at lower degrees of flexion than what is routinely believed (>90°). 9 This is not entirely unexpected, as a prior study by Fernquest et al 8 demonstrated that larger degrees of cam morphology (more asphericity) impinge with lower degrees of flexion. After cam correction, the risk of impingement was decreased and occurred at higher degrees of flexion, which was more similar to the study involving THA. This is likely because of restoration of more normal proximal femoral anatomy.
Reduced ROM due to impingement is a known sequela of cam morphology, as FAIS has been demonstrated to reduce hip flexion, abduction and adduction, and rotation compared to healthy controls in several athletic populations. 1,8,14 Improved hip motion has also been demonstrated after cam correction. 3,4 This same trend was observed in the current study; there were significant increases in the number of safe and impingement-free male and female sexual positions after cam correction.
In addition to improved ROM after cam correction, the location of impingement changed after cam correction. Prior studies have shown that impingement most often occurs on the anterosuperior aspect of the acetabulum with cam morphology, with resultant chondrolabral lesions (and possibly the commencement of arthritis) frequently occurring here. 2 –4 This differed from the present study, in which most (70.1% before correction and 100.0% after correction) impingement occurred along the anterior acetabulum. The difference in findings could be a result of the current model keeping the center of femoral head rotation static and preventing any translation, which may not accurately represent true in vivo conditions (capsular, labral, musculotendinous influences), an omnipresent limitation of imaging-based collision detection investigations. It could also simply be because of a difference in classification systems for assigning intra-articular central compartment geography. There was also no contrecoup lesion along the posterior acetabulum in the current study, with the impingement locations mutually exclusive from one another. This difference is likely because of sex-specific sex positions and patient-specific anatomy of the pelvis and femur playing a role in the location of impingement. 12 Additionally, the lack of soft tissue structures around the hip in the 3D model limits the detection of impingement to solely bone-on-bone contact.
It is likely that the significant reduction in impingement after cam correction is responsible for the clinical and sexual activity improvements as reported by Lee et al. 13 These authors showed that 66% of patients reported significant sexual dysfunction before arthroscopic hip preservation surgery (including cam correction), which then significantly decreased to only 10.8% after surgery, with 88.9% of patients reporting relief of pain. Return to sexual activity after surgery is highly multifactorial because of a variety of osseous, soft tissue (capsule, iliopsoas, rectus femoris, adhesions, peritrochanteric, etc), and mental (confidence, fear, apprehension, kinesiophobia, anxiety, etc) reasons. Further, a sex-dependent positional influence also exists because of several female positions requiring excessive flexion. Despite the current study illustrating significant improvements in the safety of many sexual positions after surgery, there were still “unsafe” positions that demonstrated a risk of impingement (despite correcting cam) with greater hip flexion. These findings can serve as a guide for patient counseling on which positions are less likely to impinge and cause discomfort after surgery for FAIS.
There are limitations to this study. This study is based on computer simulation and may not mirror the in vivo environment before and after hip preservation surgery. This collision-detection study relates only to osseous impingement and does not take into account soft tissue structures (capsule, labrum, postoperative adhesions, musculotendinous units) surrounding the hip. The loss of motion observed with cam morphology may have varying patient-specific contributions from bone and soft tissue. The improvement in motion after cam correction may be caused by improved sphericity, head-neck offset, and femoroacetabular clearance or could be from altered capsular integrity permitting greater motion in multiple planes. The small sample size may also limit the generalizability of the results, as cam morphology differs from hip to hip, but it was based on previously published methods. 4
Further, cam morphology is a complex 3D morphology, but complete analysis of proximal femoral anatomy requires investigations beyond that of the alpha angle: neck-shaft angle, neck version, femoral version, femoral neck offset, omega angle, omega surface, and triangular index. Additionally, the acetabular side (dysplasia and pincer) and lumbopelvic side (pelvic incidence, sacral slope, pelvic tilt, lumbar lordosis, thoracic kyphosis, scoliosis) were omitted during this investigation, but they do play a role. Analysis of hip motion was only conducted for specific sexual positions and was not carried out for every possible plane of motion, leaving us unable to quantify the degrees of motion improvement after cam correction. In addition, not all sexual positions were analyzed. Further, the degrees of motion utilized were based on another institution’s motion analysis using young, healthy volunteers (similar to that of the current study), but only 2 volunteers were used. These degrees of motion may not be applicable to a larger population.
Conclusion
After cam correction, there was a significant reduction in the impingement rate and a significant increase in the number of “safe” sexual positions.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: S.J.N. receives research support from AlloSource, Arthrex, Athletico, DJ Orthopaedics, Linvatec, MioMed, Pivot Medical, Smith & Nephew, and Stryker; has received educational support from Elite Orthopaedics; receives royalties from Ossur and Springer; and is a paid consultant for Ossur and Stryker. J.D.H. receives research support from DePuy and Smith & Nephew, is a consultant for NIA Magellan and Smith & Nephew, receives royalties from SLACK, has received educational support from Arthrex and MedInc of Texas, and is a paid speaker/presenter for Smith & Nephew and Ossur.
Ethical approval for this study was obtained from Houston Methodist.