
Abstract
Background:
Different surgical techniques have been described for the treatment of knee dislocation (KD). Nonoperative approaches are frequently combined with surgical reconstruction using auto- or allograft.
Purpose:
To evaluate the midterm results of primary surgical repair and suture augmentation to treat KD.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 22 patients (5 women, 17 men; mean age, 45 ± 15 years) with KD were evaluated at a mean of 49 ± 16 months after surgical treatment that included primary repair and suture augmentation. Magnetic resonance imaging, stress radiographs, and outcome scores were obtained at the follow-up. Clinical examination including hop tests and force measurements for flexion and extension was performed.
Results:
The mean difference in pre- to postinjury Tegner scores was –2 ± 1. The outcome scores showed mean values of 84 ± 15 (Lysholm), 73 ± 15 (International Knee Documentation Committee) and 65 ± 25 (Anterior Cruciate Ligament–Return to Sport after Injury scale). Compared with the uninjured knee, the range of motion of the injured knee was reduced by 21° ± 12°. Twelve patients felt fit enough to perform hop tests and showed a mean deficit of 7% ± 17%° compared with the uninjured leg. The mean force deficit was 19% ± 18% for extension and 8% ± 16% for flexion. Stress radiographs revealed an 11 ± 7–mm higher anteroposterior translation on the injured side. Four patients had secondary ligament reconstructions due to persistent instability and 7 underwent arthroscopic arthrolysis due to stiffness. A significant increase of osteoarthritis was found for the medial, lateral, and patellofemoral compartments (P = .007, .004, and .006, respectively).
Conclusion:
Primary repair and suture augmentation of KD led to satisfactory clinical midterm results despite persistent radiological instability and a significant increase in osteoarthritis. This technique allows the return to activities of daily living without subjective instability in most nonathletic patients. Secondary ligament reconstructions should be performed if relevant instability persists to decrease the risk of secondary meniscal and cartilage damage.
Knee dislocation (KD) is a rare but severe injury. 23,28,34,36 Associated vascular injuries occur in up to 40% of cases and make it possibly limb-threatening. Other concomitant injuries are nerve injuries caused by traction or disruption. The peroneal nerve is most frequently affected. Nerve injuries require urgent surgical exploration with decompression or reconstruction to provide the best conditions for recovery. 5,24
In general, most surgeons treat these injuries surgically, as better functional outcomes have been reported compared with conservative treatment. 25,42 Different approaches regarding timing, staging (1 versus 2 stage), and kind of surgery (repair versus reconstruction) have been described. Recent literature advocates early surgery, 7,18,38 although there are controversial reports showing similar results with delayed surgery. 17,26 Two-stage procedures with primary stabilization of the collateral ligaments and secondary reconstruction of the cruciate ligaments have been described in comparison with 1-stage procedures, without a clear superiority of one of these approaches. 3,21,22 In addition, there is controversy regarding the best surgical technique. A systematic review by Levy et al 25 and a meta-analysis by Frosch et al 13 compared primary repair versus primary reconstruction and showed similar clinical outcomes. In summary, currently, there is no clear evidence on the best surgical treatment, which is why our center prefers a cost- and ligament-saving procedure as initial treatment.
Our approach contains primary surgical repair protected by suture augmentation to facilitate the healing of the sutured ligaments. 19,20 The advantage of this technique lies in the reduced need of autograft and allograft, which reduces donor-site morbidity and overall societal costs. In case of persisting instability of certain ligaments, the respective ligaments can be reconstructed subsequently in a selective approach.
To date, only a few short-term follow-up studies of suture augmentation techniques for KDs are available; these studies have reported favorable outcomes. 13,19 The aim of the current study was to provide midterm follow-up data for this surgical technique. 19,20,37 We hypothesized that satisfactory midterm results will be achieved.
Methods
Patient Selection and Demographics
We retrospectively searched our clinical database for patients who underwent reconstruction of a KD between January 2014 and February 2019. This study was approved by the Swiss cantonal ethics committee and every patient signed an informed consent.
Inclusion criteria were rupture of ≥2 knee ligaments at the initial injury with 1 of them being the anterior cruciate ligament (ACL) or the posterior cruciate ligament (PCL) and a minimum follow-up of 24 months. Moreover, ≥1 ligament needed to be treated with suture augmentation. A minimum age of 18 years was also required. Exclusion criteria were the presence of severe additional injuries to the same leg (eg, foot amputation) or general injuries leading to permanent impairment of the knee (eg, paraplegia). Refusal to sign the informed consent led to exclusion.
In total, 22 patients met the criteria and were invited to a follow-up with a comprehensive clinical and radiological assessment after a mean postoperative time of 49 ± 16 months. The Schenck classification was used to classify the injuries. 14 Demographics and injury characteristics are listed in Table 1.
Demographics and Injury Characteristics (N = 22) a
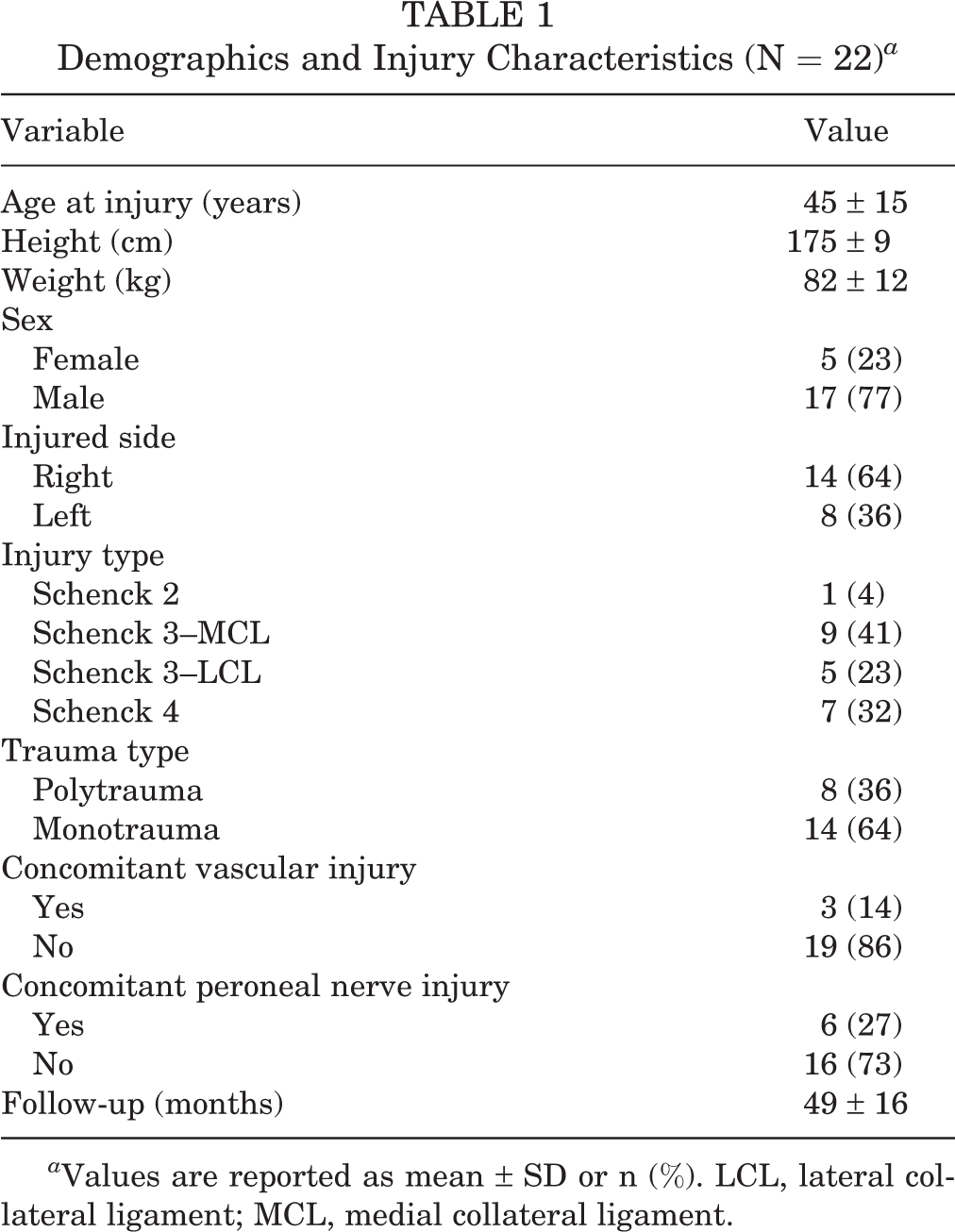
a Values are reported as mean ± SD or n (%). LCL, lateral collateral ligament; MCL, medial collateral ligament.
Surgical Technique and Rehabilitation
The surgical technique was similar to that reported by Heitmann et al in 2014 for suture augmentation of KD. 20 The main concept is primary repair of the torn ligaments and support with suture augmentation. The repair was performed as transosseous reinsertion in case of avulsion. In midsubstance tears, the sutures of each stump were shuttled through the opposite drill hole and knotted over a suture button. ACL and PCL were braced independent of the rupture site and the medial collateral ligament (MCL) only in case of intraligamentous ruptures. The lateral collateral ligament (LCL) was braced only if sufficient adaption of the stumps could be achieved; otherwise, it was reconstructed. A detailed description of the surgical technique, including approach and augmentation technique for all respective ligaments and tear patterns, is provided separately as supplementary Material.
All torn structures were repaired with No. 2 FiberWire (Arthrex) using a baseball-stitch technique. Drill channels of 4.5 mm were established at the respective ligament insertions to enable insertion of suture augmentation tapes.
For fixation of the suture augmentation of ACL and PCL, a 10-mm fixed-loop Endobutton (CL ULTRA; Smith & Nephew) was used. Regarding the ACL, a FiberTape (Arthrex) was inserted into the loop of the Endobutton, resulting in a 2-strand ACL augmentation. For the PCL, an identical FiberTape was used but was folded in the middle before insertion into the loop, which led to a 4-strand augmentation (Figure 1). Distally the FiberTapes were knotted over a button plate (DePuy Synthes).
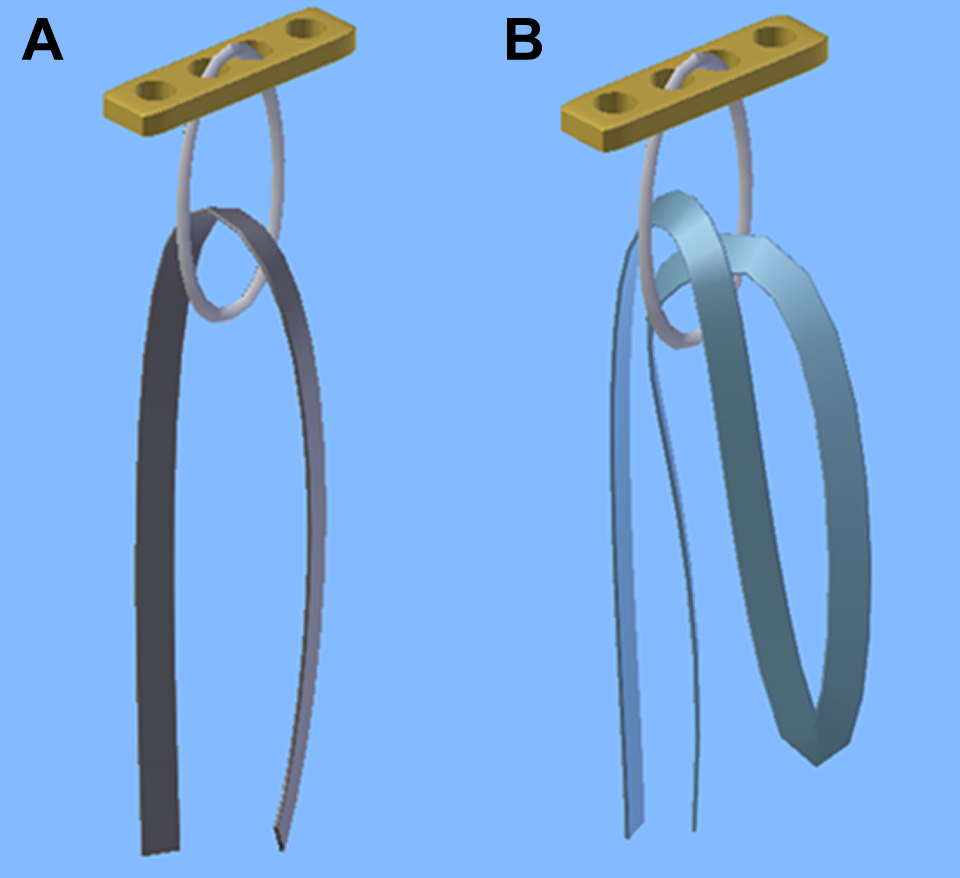
Illustration of Endobuttons with a 10-mm continuous loop in which a FiberTape has been inserted in the (A) 2-strand and (B) 4-strand technique.
Regarding the MCL, in our experience, nonabsorbable strong tapes may lead to persistent tenderness. Thus, we used an absorbable 3 mm–wide and 60 cm–long biodegradable Vicryl Tape (Ethicon; Johnson & Johnson Medical) for MCL augmentation. The LCL was braced with a FiberTape that was routed through a fibular tunnel based on Larson technique, 10 if necessary. Button plates were used to tighten the sutures and augmentations of all respective ligaments over the bone.
Postoperatively, all patients received a knee brace providing adjustable anteriorly directed force. The flexion limits were 30°, 60°, and 90° for 2 weeks each. During the first 6 weeks, partial weightbearing of 15 kg was allowed. Subsequently, a stepwise load increase to full weightbearing was initiated over a further 6 weeks; the brace was worn during this time, but range of motion (ROM) was not limited.
Laxity Evaluation and ROM
For the ACL the anterior drawer was tested in 20° to 30° of flexion, and for the PCL, the posterior drawer was tested in 90° of flexion. The collateral ligaments were tested in 20° to 30° of flexion by applying varus and valgus stress. Translation or laxity was rated for all ligaments as 0 to 2, 3 to 5, 6 to 10, or >10 mm. Moreover, ROM was measured using a goniometer.
The device-based evaluation of laxity was performed with the KT-1000 Knee Ligament Arthrometer (MEDmetric) at 67 and 89 N for both anterior and posterior translation. 4,29
Radiographic Evaluation
Stress radiographs using the Telos stress device (Austin & Associates) were performed at the final follow-up to assess anterior (in 20° flexion) and posterior translation (in 90° flexion) within both knee joints. For both measurements, a force of 200 N was applied. The translation was quantified as anteroposterior distance of the dorsal femoral condyle to the posterior edge of the tibial plateau on lateral view radiographs. 2 To compare the results, the differences between the translations of the injured and the uninjured legs were calculated.
Magnetic Resonance Imaging (MRI) Evaluation
Twenty (91%) patients had preoperative MRI of the knee, and 22 (100%) underwent knee MRI at latest follow-up. Postoperative imaging was consistently performed at 1.5-T (Siemens Aera; Siemens Healthineers) to reduce artifacts resulting from surgical hardware. A radiology resident (F.S.) and a fellowship-trained musculoskeletal radiologist (R.J.E.) performed the MRI analysis in consensus. Preoperative and follow-up MRI scans were evaluated for tearing of the ACL, PCL, MCL, and LCL in a dichotomous fashion (0 = intact/partially torn fibers; 1 = completely torn fibers).
Meniscal injuries were also assessed dichotomously (lesion: yes or no). Joint degeneration was graded based on a previously validated semiquantitative grading scheme according to Park et al 32 for the medial, lateral, and patellofemoral compartments.
Strength Testing
Isokinetic strength of knee extension (quadriceps) and knee flexion (hamstrings) was tested on the HUMAC Norm Isokinetic Dynamometer (CSMI USA) with the uninjured, contralateral leg tested first. 15 The testing protocol consisted of 3 different speeds: 60°/s for 5 repetitions, 120°/s for 5 repetitions, and 180°/s for 15 repetitions. For each speed, the patients had 4 tries to familiarize themselves with the device and speed, with 90 seconds between each try. Maximum peak torque was determined for both knee flexion and extension strength. Limb symmetry index (LSI) was calculated for flexion and extension as the ratio of the peak torque of the injured limb in relation to the contralateral limb (reported as a percentage; eg, an LSI of 75% means a deficit of 25% of the injured leg).
Hop Testing
Single and triple hop for distance as established in the test battery by Reid et al 35 were performed. The patient’s confidence regarding knee stability during a hop test, and a strength LSI of minimum 80%, were required before these tests were performed. The uninjured leg was tested first with 2 hops to familiarize. Hop distance was measured from the start line to the front of the patient’s shoe. The patients performed 2 tries, of which the average was calculated and documented. LSI was calculated as for strength testing.
Patient-Reported Outcome Measures
To analyze the subjective and objective clinical outcomes, we used the following patient-reported outcome measurements (PROMs): Tegner activity scale, Lysholm score, International Knee Documentation Committee (IKDC) score, and ACL–Return to Sport after Injury scale (ACL-RSI).
Statistical Analysis
SPSS Statistics was used for data analysis (Version 25 for Windows; IBM SPSS Statistics). Data were normally distributed according to Kolmogorov-Smirnov test and were therefore presented as means with standard deviations. Simple descriptive statistics were used to answer the study questions. The Wilcoxon signed-rank test was used to compare ordinal data and Student t test to compare quantitative data. The significance level was set at P < .05.
Results
Initial Trauma
MRI was performed in 20 of the 22 study patients (91%) to evaluate the extent of the ligamentous injury. Two patients (9%) were directly treated with open reduction and debridement in the operating room due to relevant soft tissue injury and traumatic opening of the knee joint. Therefore, no preoperative MRI could be performed. Concomitant vascular and peroneal nerve injuries are listed in Table 1. In 1 patient (5%) conservative observational treatment due to femoral popliteal dissection was performed, whereas in 2 patients (9%) open reconstruction of the popliteal artery with a venous autograft was necessary. A peroneal nerve palsy was found in 6 cases (27%), but during surgical exploration, the continuity of the nerve was confirmed in all cases. In 2 cases (33%), an incomplete sensorimotoric deficit persisted at the final follow-up, whereas 1 patient (17%) reported some sensory deficit. The remaining 3 cases (50%) showed a complete recovery.
Surgical Ligamentous Stabilization
The mean time between injury and surgery was 11 ± 8 days. The ACL was sutured and braced in 20 cases (91%). In 2 cases (9%), a repair was not possible because the ACL was absent and reconstruction was not performed. The PCL was sutured and braced in all 22 cases (100%). The MCL was treated with primary repair alone in 7 cases (44%) and with additional augmentation in 9 cases (56%). The LCL was treated with primary repair alone in 4 cases (33%), with additional augmentation in 1 case (8%), and with primary reconstruction (Larson technique 10 ) using allograft (Achilles tendon) in 7 cases (58%).
Subsequent Surgeries
Four patients had persistent ligamentous instability and underwent secondary reconstruction of the ACL in 2 cases (9%), the PCL in 1 case (5%), the MCL in 2 cases (9%), and the LCL in 2 cases (9%). One patient (5%) received a lateral meniscal allograft transplantation; and in 7 cases (32%), an arthroscopic arthrolysis was performed due to stiffness. One patient (5%) received arthroscopic lavage and debridement due to an early infection 3 weeks after initial treatment. Overall secondary surgeries were performed after a mean of 9 ± 7 months. Regarding arthrolysis and secondary ligament reconstructions, the time to secondary surgery was 8 ± 6 months and 6 ± 4 months, respectively. One (50%) of the secondary ACL reconstructions was performed in a case in which primary repair was not possible during the first surgery.
Clinical Evaluation and Functional Testing
The mean ROM of the uninjured leg was 21° ± 5° higher than of the injured leg. Seven patients had an extension deficit of mean 9° ± 5°. The detailed results of the clinical examination comparing both legs are listed in Table 2. Overall extension force was significantly lower than overall flexion force (P = .025). Twelve patients (55%) felt fit enough to perform hop tests. A comparison of the patients confident enough to perform the hop test with those who were not revealed a mean LSI for extension of 85% ± 14% and a mean LSI for flexion 95% ± 9% in the first group compared with respective values of 76% ± 21% (extension) and 87% ± 20% (flexion), albeit not statistically significant (P = .279 and .270, respectively). Table 3 summarizes the results of functional testing, hop tests, and strength assessments.
Clinical Examination Results a
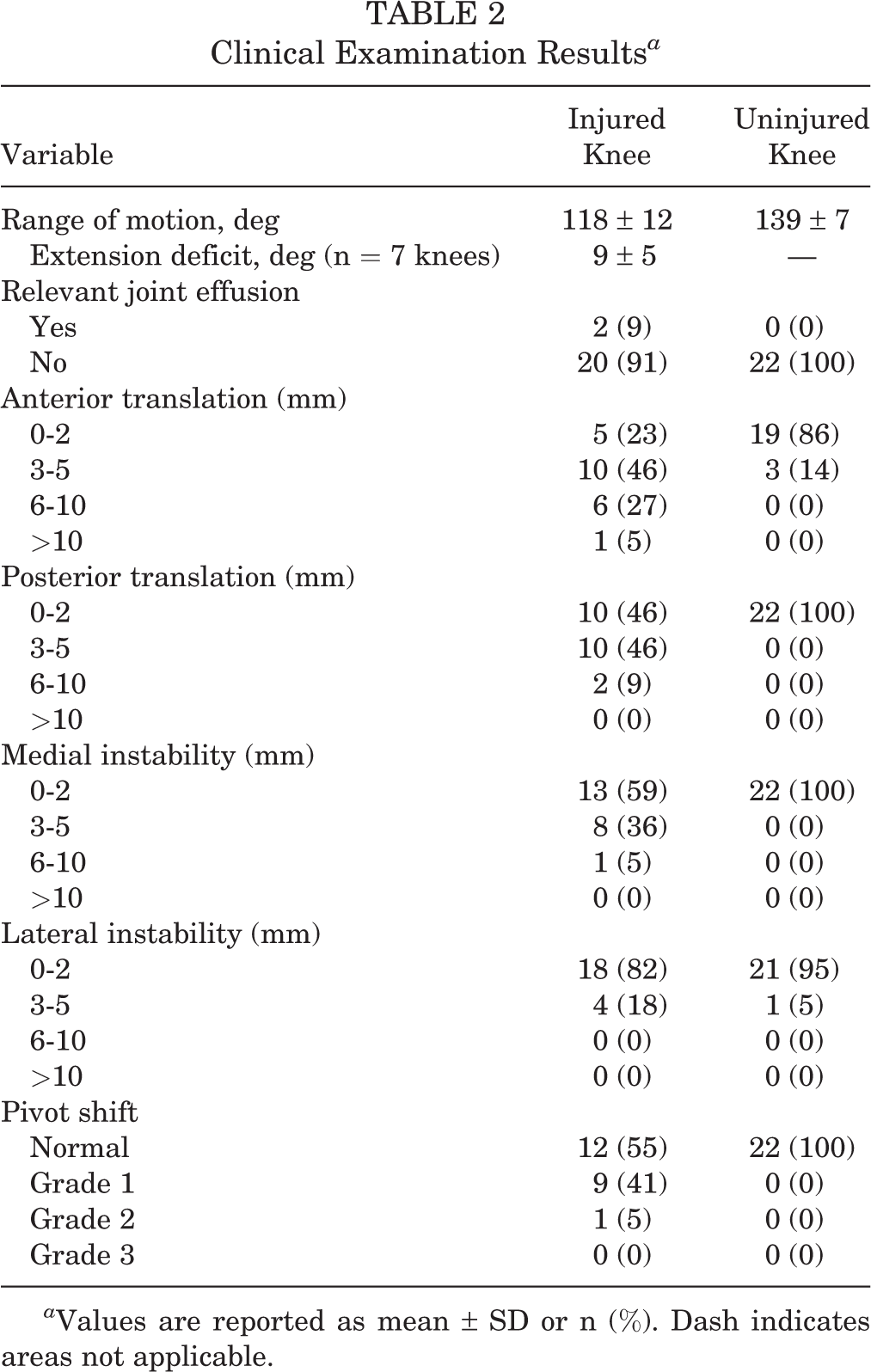
a Values are reported as mean ± SD or n (%). Dash indicates areas not applicable.
Results of Functional, Hop, and Strength Testing a

a Values are reported as mean ± SD. Dashes indicate areas not applicable. LSI, limb symmetry index.
b Hop tests were only performed on 12 patients.
Radiographic and MRI Results
The stress radiographs revealed a significantly higher mean anterior translation of 4 ± 6 mm (P = .011), posterior translation of 7 ± 6 mm (P < .001), and maximal anteroposterior translation of 11 ± 7 mm (P < .001) on the injured side compared with the uninjured side (Table 4).
Radiographic Evaluation (Stress Radiographs) a
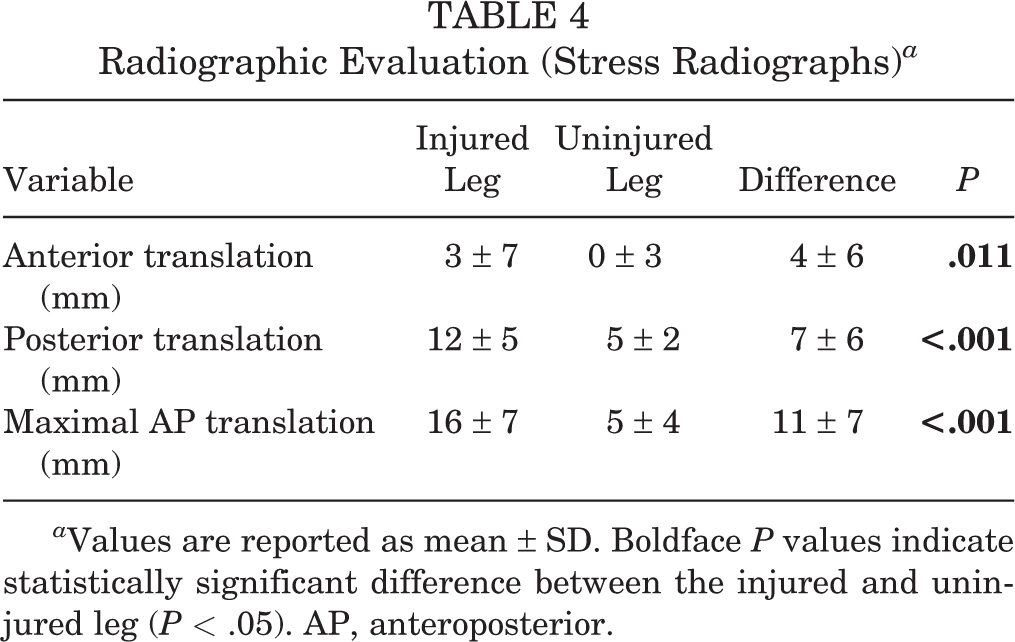
a Values are reported as mean ± SD. Boldface P values indicate statistically significant difference between the injured and uninjured leg (P < .05). AP, anteroposterior.
The retrospective comparison of the preoperative MRI versus final follow-up MRI revealed a 100% healing rate for PCL, MCL, and LCL, although it must be remembered that some of these ligaments were secondarily reconstructed. The ACL reconstructions were not as successful. Two (9%) ACLs could not be repaired or braced at the initial surgery and 2 (9%) of the ACL repairs failed. Moreover, 10% (2/20) of the ACLs and 15% (3/20) of the PCLs were falsely rated as intact on the preoperative MRI scans, while subsequent surgery revealed that they were torn. The results of the MRI analysis are displayed in Tables 5 and 6. Overall, a significant increase in osteoarthritis (OA) grade was found for the medial (P = .007), lateral (P = .004), and patellofemoral (P = .006) compartments.
MRI Evaluation a

a Values are given as n (%). ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
MRI Evaluation of Osteoarthritis a

a Values are reported as n (%). Boldface P values indicate statistically significant difference between preoperative and final follow-up (P < .05). MRI, magnetic resonance imaging.
b According to Park et al. 33
Patient-Reported Outcome Measures
No patient reported a preinjury limitation of the knee function. The mean preinjury Tegner score was 7 ± 2, whereas at the final follow-up the score was 5 ± 2. The PROMs showed mean values of 84 ± 15 (Lysholm), 73 ± 15 (IKDC), and 65 ± 25 (ACL-RSI).
Exemplary Cases
Figures 2 and 3 show the exemplary radiologic outcome of 2 patients with a similar age and follow-up time. Despite the fact that in both cases, all respective ligaments were healed and only very small ligamentous instability was present (compared with the uninjured leg), 1 of the patients (Figure 3) developed osteophytes in the context of OA whereas the other patient did not (Figure 2).

MRI scans from a 37-year-old patient with Schenck 3–MCL knee dislocation. Primary surgical repair was performed with suture augmentation of the ACL, PCL and MCL. (A-F) Preoperative (A) coronal, (C) sagittal ACL (proximal rupture, bold arrow), and (E) sagittal PCL (distal rupture, long arrow) MRIs were compared with the respective postoperative MRIs at 3.9 years after reconstruction (B, D, and F). Arrowheads in (B) mark osteophytes. All affected ligaments had healed. (G-J) PCL stress radiographs of the (G) uninjured and (I) injured knee are shown as well as ACL stress radiographs of the (H) uninjured and (J) injured leg. The red line marks the tangent to the posterior medial femoral condyle, the blue line the posterior edge of the medial tibial plateau, and the yellow line indicates the joint level. Green lines and text indicate (G and I) posterior translation and (H and J) anterior translation of the tibia. ACL, anterior cruciate ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.

MRI scans from a 39-year-old patient with Schenck 3–LCL knee dislocation. Primary surgical repair was performed with suture augmentation of the ACL and PCL. Furthermore, Larson reconstruction of the posterolateral corner with allograft and transosseous reinsertion of the posteromedial meniscal root and of the popliteal tendon were performed. Preoperative MRI–-(A) coronal, (C) sagittal ACL (proximal rupture, bold arrow), (E) sagittal PCL (proximal rupture, long arrow)–-is compared with the respective postoperative MRI (B, D, and F; arrowheads mark osteophytes) 4.2 years after reconstruction. All affected ligaments are healed. PCL stress radiographs of the uninjured (G) and injured (I) knee are shown as well as ACL stress radiographs of the (H) uninjured and (J) injured leg. The red line marks the tangent to the posterior medial femoral condyle and the blue line the posterior edge of the medial tibial plateau. The yellow line indicates the joint level. The translation is given in green for the (G, I) posterior translation and (H, J) anterior translation of the tibia. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MRI, magnetic resonance imaging; PCL, posterior cruciate ligament.
Discussion
This study reports the clinical and radiological midterm outcome of 22 patients after KD treatment with open repair and suture augmentation. We hypothesized that satisfactory midterm results can be achieved using this technique. We could confirm our hypothesis in this study with 4 years of follow-up. As there is no clear definition of “satisfactory results,” we now discuss the results of this study in the context of a KD. In our study of patients with a mean age of 45 years, we found a mean Tegner score of 5 points corresponding to performing heavy labor work or to perform cross-country skiing and is comparable with the reported mean score of 6 points in a study of 488 patients (mean age of 41 years) without any preexisting injuries reported. 6 Other studies reported Tegner scores in patients with multiligament knee injury (MLKI) of 3 (nonoperative treatment) and 4 points (primary reconstruction). 25 Even in professional athletes, the return to play on a preinjury level has been reported as low as 22% to 33%. 31 In this context, a drop in Tegner score of 2 points and a mean absolute postoperative Tegner score of 5 points is in the opinion of the authors a satisfying result. In our cohort, Lysholm and IKDC scores lie within the upper third of the scale, which further confirms our hypothesis. Only the ACL-RSI scale was lower at 65 points, suggesting that patients’ confidence in their injured limb was lower than the actual function raised by the other scores would suggest. This phenomenon has also been reported. 41
Regarding surgical treatment of KD, some authors opt for an early reconstruction with autograft or allograft. 7,18,38 Looking at our data after initial surgical repair and suture augmentation, 18% of the patients needed secondary ligament reconstruction whereas 32% needed arthroscopic arthrolysis. In primary reconstruction surgery, rates of 6% and 17% have been reported, respectively. 33 This higher rate of secondary surgeries can lead to the discussion whether ligament repair and augmentation can be recommended in the treatment of KD. In our opinion, in particular, in countries where allograft is not easy to obtain this option should be considered. Reconstruction of all ligaments in patients with KD might reduce the secondary surgeries but, on the other hand, in would lead to an overtreatment of about two-thirds of the patients. This would additionally significantly increase the costs. As the subjective results may not be significantly different after primary repair and primary reconstruction, we believe it is legitimate to repair first and do reconstructions only if relevant instability persists. 13,25 We observed a mean ROM of 118°, which is sufficient for activities of daily living as well as for many sports. Nevertheless, other studies report a 5° to 10° higher ROM after surgical reconstruction of MLKIs. 25,38,42 An extension deficit of more than 5° was present in 18% of our patients, which is slightly out of the reported range of 5% to 10%. 30 Seven patients had a postoperative extension deficit of mean 9°, which indicates that most of the current study’s reported side differences in ROM were due to a decrease in flexion. A reason for this reduced ROM might be our restrictive rehabilitation protocol. Early aggressive mobilization might lead to better ROM but also contains the risk of impaired ligament healing. 27,30 Though joint stiffness and extension deficits are well-known problems after KD independent of the treatment strategy, to date no good solution for this problem has been reported. 31 As this study’s reported ROM leads to good subjective and objective clinical functioning, we recommend a cautious rehabilitation protocol rather than risk failure of ligament healing.
The reported results of mediolateral stability lie within the expected range. However, in this regard, it has to be stated that 58% of the LCL injuries were directly reconstructed with allograft, because there is some evidence available reporting worse outcomes in higher degree LCL lesions when primary repair (and augmentation) is performed compared with direct reconstruction. 25 We believe that (bony) avulsions of the LCL can be treated with transosseous reinsertion but that in case of intraligamentous lesions, a primary reconstruction should be considered. The cohort presented here was treated accordingly. However, there is no large study comparing the results of lateral repair and reconstruction in terms of the tear patterns of the LCL. Moreover, suture augmentation of the MCL was only performed in about half of the cases reported here, which weakens the generalizability of the results.
Anteroposterior stability was assessed with clinical examination, KT-1000 measurements, and stress radiographs. The problem in KD is that the neutral position cannot be determined clinically if alterations of both ACL and PCL do exist. Therefore, clinical (anterior and posterior drawer test) and KT-1000 absolute measures often differ from radiographic measures, and this is also the case in our study. 1 Most prior studies reported only the results of the manual measurement methods. 16 This can be misleading, as suggested by our results of a higher anteroposterior translation measured on stress radiographs. The stress radiographs and their interpretation were formerly developed to assess isolated ACL or PCL injuries. In case of KD, the comparison of the absolute anterior and posterior translation might not be enough. Therefore, we also calculated the maximal anteroposterior translation, which represents the sum of anterior and posterior translation. The side-to-side difference regarding this value can be used as a parameter for overall anteroposterior stability after KD surgery. In this study, a significant increase in maximal anteroposterior translation of 11 mm was detected. Heitmann et al 20 reported a maximum anteroposterior translation of 6 mm on stress radiographs using a similar surgical technique. One reason for the considerably higher values in our study might lie in a learning curve for this augmentation technique, because the study contains the very first patients treated with this technique. Another reason might be that their values for anterior translation are underestimated because measurements were performed in 90° of flexion, whereas our measurements were performed in 20° of flexion. However, no reference data exist to interpret this finding in terms of OA prediction or correlation between clinical outcomes.
In terms of functional recovery, Engelen-van Melick et al 9 came to the conclusion that an LSI between 80% and 90% is considered normal, because it represents the range available in uninjured people. Considering this, our cohort reaches this range for the extension with mean of 81%, only scarcely surpassing it; however, with regard to flexion, our cohort reaches this range with a mean 92%. In this regard, 59% of our patients had adequate strength to return to sports after recovering from this severe injury. With regard to the hop tests, the mean value of those in our cohort who performed the test is also above the required range (93%). Only 55% of our patients felt confident enough to perform the hop tests, which weakens the generalizability of these results. Reasons might lie in the older age of the patients, a decreased confidence in the injured knee (ACL-RSI scale), and persisting ligamentous instability. We are not aware of other studies reporting hop tests after surgical treatment of KD, which makes comparability difficult.
The postoperative MRI evaluation revealed an intact PCL, MCL, and LCL in all cases, whereas the ACL was absent in 27% of the cases. This suggests a general morphologic success of the surgical intervention, especially regarding PCL treatment, because all patients included had a PCL rupture and were treated with primary repair and suture augmentation. The ACL was also torn or absent in all patients, and primary repair and suture augmentation was performed in 91% of patients. However, a failure rate of 10% was observed, which is less compared with studies reporting failure rates of around 20% in isolated ACL primary repair and augmentation. 39 A reason for the ACL failures might be the rehabilitation protocol and brace with anterior translation, which mainly focuses on healing of the PCL. Nevertheless, ACL augmentation in KD seems to have a better healing rate than in isolated ACL injuries. Augmentation of the LCL cannot be adequately assessed from our data, as it has only been performed in 1 case. Regarding the MCL, about half of the lesions were treated with repair only (proximal or distal avulsions), whereas in the other half, repair with additional augmentation (intraligamentous ruptures) was performed. Our results lie within the known success rates for MCL repair and/or augmentation of 88% to 100% in the context of KD. 11
A significant increase of OA was found for all compartments of the knee, which probably displays the natural course after a KD described by other authors. 17 However, most outcome studies after KD treatment do not report radiological outcome. Therefore, there are no good outcome data comparing OA development after different treatment methods for KD. It is known from ACL injuries that reconstruction does not prevent OA and that even the hypothesis that it is slowing down its progression has not been sufficiently proven. 12 Nevertheless, Park grade 4 lesions of 36% in the medial and 41% in the lateral compartment are concerning at 4 years postoperatively. Therefore, long-term outcome data including radiological (MRI) analysis are needed to compare the results of different surgical techniques and to decide preoperatively which surgical technique should be used.
Limitations
The main limitation of this study is that a subgroup analysis to detect risk factors for worse outcomes could not be performed with sufficient power due to the limited number of included cases in each subgroup. Moreover, a direct comparison with primary reconstruction is not possible because no matched cohort undergoing this procedure was available. In this regard, it is known that primary reconstruction cannot always prevent OA, 40 but a direct comparison of the 2 techniques would be favorable. Another limitation is that there is some discrepancy between objective results (residual laxity, OA progression) and subjective outcome (good outcome scores and daily function). In our cohort of patients (mean age 45, no athletes) the main goal is to restore function of the knee for normal activities of daily living (ADL). Therefore, we decided to emphasize the good subjective results, which are indicated by good PROMs. If this cohort had been an ACL reconstruction group or young athletes, the results could not be interpreted as satisfying. Another fact complicating the interpretation of the results is that low-energy KDs are known to achieve better postoperative activity scores. 8 However, in this group of middle-aged patients with severe knee injuries, we believe it is legitimate to state that satisfying results can be achieved using primary repair and suture augmentation.
Conclusion
Primary repair and suture augmentation seems to be associated with higher rates of secondary surgeries when compared with primary ligament reconstructions. However, it results in satisfactory clinical outcomes, despite persistent radiologic instability and significant increase of OA. Therefore, primary repair and suture augmentation of ACL, PCL, and MCL seems to be a viable option for KDs as a ligament-saving procedure. This technique allows the return to activities of daily living without subjective instability in most nonathletic patients. Secondary ligament reconstructions should be performed if relevant instability persists to decrease the risk of secondary meniscal and cartilage damage.
Supplemental Material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671221132555#supplementary-materials
Supplemental Material
Supplemental Material, sj-docx-1-ojs-10.1177_23259671221132555 - Treatment of Knee Dislocation With Primary Repair and Suture Augmentation: A Viable Solution
Supplemental Material, sj-docx-1-ojs-10.1177_23259671221132555 for Treatment of Knee Dislocation With Primary Repair and Suture Augmentation: A Viable Solution by Andreas Hecker, Florian Schmaranzer, Christoph Huber, Jonas Maurer, Rainer J. Egli, Sophie C. Eberlein and Frank M. Klenke in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank Scilla Dozio for her assistance with MRI and radiographic imaging.
Final revision submitted July 31, 2022; accepted August 10, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Kantonale Ethikkommission Bern (ref No. 2020-00912).