
Abstract
Background:
Multiligamentous knee injuries (MLKIs) are devastating injuries with concomitant injuries that complicate treatment and recovery. Short-term studies have shown satisfactory patient outcomes after surgical treatment; however, evaluations of long-term outcomes remain scarce.
Purpose:
To evaluate long-term outcomes after surgically reconstructed MLKIs and further investigate the relationship between patient age on clinical outcomes.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 55 knees (age, 36 ± 11 years; 24% female subjects) who underwent surgical reconstruction for MLKI between 1992 and 2013 met the study inclusion criteria and were evaluated with postoperative patient-reported outcomes (PROs) including International Knee Documentation Committee (IKDC) score, Lysholm score, visual analog scale (VAS) for pain, Forgotten Joint Score, subjective improvement ratings and surgery satisfaction, and Tegner activity scores. PRO scores, revision, and conversion to arthroplasty were analyzed using descriptive statistics, linear regression, Wilcoxon rank-sum, and Fisher exact tests.
Results:
At final follow-up (mean, 15 ± 5 years; range, 10-31 years), 67% of the cohort reported subjective improvement in their knee, and 82% reported satisfaction with their surgery. Compared with preoperative scores, there were significant improvements in postoperative VAS pain at rest in the full cohort, age ≤30-year cohort, and age >30-year cohort (4 ± 1 vs 2 ± 2; 4 ± 1 vs 2 ± 3; 4 ± 1 vs 1 ± 2, respectively; P≤ .029 for all) but significant reductions in Tegner scores (6 ± 3 vs 4 ± 2; 7 ± 2 vs 5 ± 2; 5 ± 2 vs 3 ± 1; P≤ .003 for all). Younger patients had higher postoperative Tegner scores than older patients (5 ± 2 vs 3 ± 1, respectively; P = .003), but no other differences in PROs were observed based on age. At a mean 15-year follow-up, 3.6% of the cohort underwent revision ligament surgery and 10.9% required arthroplasty.
Conclusion:
The majority of the cohort reported modest subjective improvement and were satisfied with their surgery. Gradual but expected age-related decreases in Tegner scores were observed, and some patients demonstrated continued symptomatic and functional limitations, but mean PRO scores remained satisfactory. Revision surgery and conversion to arthroplasty were not commonly required.
Multiligamentous knee injuries (MLKIs) are caused by high-energy trauma, sporting accidents, and other mechanisms.4,9,32 MLKIs are defined as injuries to at least 2 of the 4 major ligaments of the knee: anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), posterolateral corner (PLC) including the lateral collateral ligament (LCL), and posteromedial corner (PMC) involving the medial collateral ligament (MCL). 17 The Schenck classification criteria for knee dislocations (KDs) categorizes dislocations based on injured structures, with a higher grade signifying a greater number of ligaments involved. 8
Despite a growing body of literature and generally accepted criteria for categorization of MLKIs, there remains a paucity of studies with the substantial sample size and extended follow-up to allow for long-term prognostication in this patient cohort. 21 Patients are also at risk of concomitant injuries to adjacent structures, including bone, menisci, and neurovascular structures, with high complication rates including arthrofibrosis in the postoperative period, which further complicate treatment and recovery. 12
In most instances, operative treatment of MLKI has been shown to be superior to nonoperative treatment for both functional and clinical outcomes.17,38 However, mid- to long-term studies have demonstrated heterogenous and, at times, poor outcomes in patients with surgically treated MLKIs, demonstrated by low patient-reported outcome (PRO) scores and increased rates of posttraumatic arthritis.17,38,41 Multiple contributing factors to these outcomes have been identified in previous studies, including mode of injury, surgical technique, obesity, concomitant injuries, patient demographics, and time to surgery.6,10,18,20,39
A previous study at our institution explored the relationship between one of these contributing factors, age, and patient outcomes at median 5-year follow-up, ultimately finding that younger patient age (≤30 years) at the time of injury and subsequent reconstructive surgery was predictive of superior clinical and functional outcome scores compared with patients >30 years of age at the time of surgery. 19 There are few long-term studies investigating this patient population; however, a recent series demonstrated poor postoperative PROs with an average International Knee Documentation Committee (IKDC) score of 62.1 ± 24.8 at mean 13.1-year follow-up compared with the age-matched normative score of 77.4 ± 23.3. 41 This study also showed moderate-to-severe posttraumatic arthritis in 100% of postoperative radiographs. 41 The complexity and variability in treatment of these injuries, in addition to the significant burden these injuries place on patients, necessitate further high-level investigation.
The purpose of this study was to evaluate long-term outcomes after surgically reconstructed MLKI and to further investigate the relationship between patient age and clinical outcomes. We hypothesized that patients would demonstrate satisfactory outcome scores, reoperation and revision rates, and conversion to arthroplasty at long-term follow-up. In addition, we hypothesized that age would remain a durable predictor of outcomes in this cohort at extended follow-up.
Methods
After the study protocol received institutional review board approval, a previously defined, prospectively generated database of patients who underwent multiligamentous reconstruction from January 1, 1992, to December 31, 2013, was utilized to obtain extended follow-up. 19 Initially, 184 patients were identified in the prospective database for inclusion in the original study. Patients were excluded if there was (1) an isolated knee dislocation (KD) grade 1 injury involving only the ACL and MCL (n = 5), (2) <24-month follow-up (n = 10), and (3) lack of sufficient outcome scores or detailed surgical procedure (n = 46). This resulted in 125 KDs in 123 patients remaining. For the current study, patients were further excluded if (1) the time from surgery was <10 years (n = 3), (2) there was <10 years of final follow-up data (n = 61), or (3) patients did not provide consent (n = 6). Ultimately, 55 knees in 53 patients were included in this study (Figure 1). At the time of final follow-up, 16 knees had reached a clinical endpoint, which was defined as death (n = 8), conversion to arthroplasty (n = 6), or revision ligament surgery (n = 2), leaving 39 knees in 37 patients available for outcomes analysis.
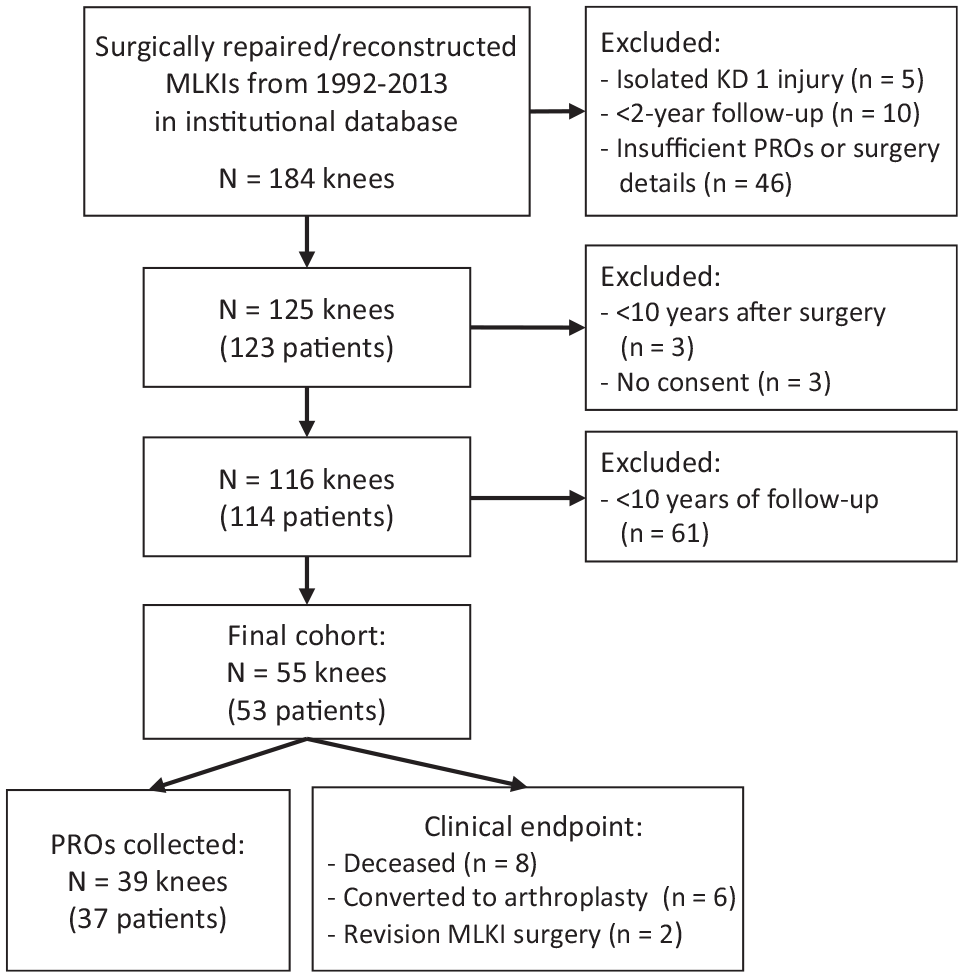
Patient selection flowchart. KD, knee dislocation; MLKI, multiligamentous knee injury; PRO, patient-reported outcome.
Surgical Technique
All patients underwent surgical reconstruction of their MLKI as indicated by clinical and/or functional instability. This technique has been described previously in this cohort. 19 In brief, a surgical decision regarding whether to repair or reconstruct the injured ligament(s) was made at the time of surgery by the operating surgeons (B.A.L. and M.J.S.) but followed basic principles that had been established previously.14,16 In general, acutely injured knees with distally based avulsions of the MCL and/or LCL were repaired, and all other ligamentous injuries were reconstructed. Notably, there was evolution in the surgical techniques for repair and reconstruction during the study period, which has been described previously in the literature,2,7,24-26,28,29,35,40 and therefore, techniques were not consistent across the duration of the study. Soft tissue allografts and/or autografts were used when necessary to reconstruct combinations of ligamentous injuries. Standardized graft preparation, tunnel preparation, and graft fixation techniques were based on the operating surgeon's preferences. Neurovascular structure, cartilage, and meniscal injuries were evaluated and recorded before and during surgery.
Outcome Evaluation
PROs including IKDC; Lysholm scores; visual analog scale (VAS) for pain on a scale from 1 to 10, with 10 being worst pain (preoperatively and at follow-up); Forgotten Joint Score (FJS); subjective improvement compared with preoperatively (1 = significantly worse, 2 = mildly worse, 3 = unchanged, 4 = mildly improved, 5 = significantly improved); surgery satisfaction (1 = very satisfied, 2 = satisfied, 3 = neutral, 4 = dissatisfied, 5 = very dissatisfied); and Tegner scores (preinjury and at follow-up) were collected via phone call or the Research Electronic Data Capture online survey database web application (REDCap; Vanderbilt University) for all patients who had not reached a clinical endpoint.
Statistical Analysis
Demographic data were summarized as means with standard deviations or as a number and percentage of total. Newly collected postoperative PROs were also summarized, both for the entire cohort and in age-defined cohorts (≤30 vs >30 years at the time of surgery), and were then compared with preoperative PROs, between age-defined cohorts. The cutoff age of ≤30 years was chosen as it was close to the mean age and thus allowed for equal distribution of patients. In addition, this cutoff age was used previously for analysis in this cohort 19 ; thus, we were able to investigate the durability of the previously observed findings. Risk factors for conversion to arthroplasty were also investigated. Linear regression was used for relationships between continuous variables, Wilcoxon rank-sum (Mann-Whitney U) tests were used to compare continuous variables between groups, and Fisher exact tests were used to compare proportions of nominal outcomes between groups. All statistical tests were 2-sided, and P values <0.05 were considered statistically significant. Statistical analysis was performed using BlueSky software, Version 7.4.0 (BlueSky Statistics).
Results
Patient Demographics and Injury Characteristics
The mean age of the 55 knees was 35.5 ± 11.2 years, and 23.6% were female. A total of 44 (80.0%) injury patterns were classified as KD grade ≥3 (Table 1). In this cohort, 46 (83.6%) of MLKI reconstruction surgeries were primary surgeries, and 9 (16.4%) were revision surgeries. More than half of all injuries (58.2%) were characterized as being high energy. Concomitant meniscal, cartilage, peroneal nerve, and popliteal injuries were seen in 58.2%, 30.9%, 25.5%, and 10.9% of knees, respectively. The 3 most common injury patterns were ACL/PCL/MCL/LCL (21.8%), ACL/PCL/LCL (30.9%), and ACL/PCL/MCL (25.5%), which were also the most common ligament combinations receiving surgical intervention, making up 16.4%, 18.2%, and 21.8% of surgeries, respectively (Table 2). A total of 21 knees (38.2%) had concomitant meniscal procedures performed at the time of surgery, including 1 knee in which both a partial medial meniscectomy and partial lateral meniscectomy was performed (Table 3). Time from initial injury to surgery was variable across the cohort, with a median time of 82 days (range, 5-5109 days).
Demographic and Injury Characteristics (N = 55 knees) a
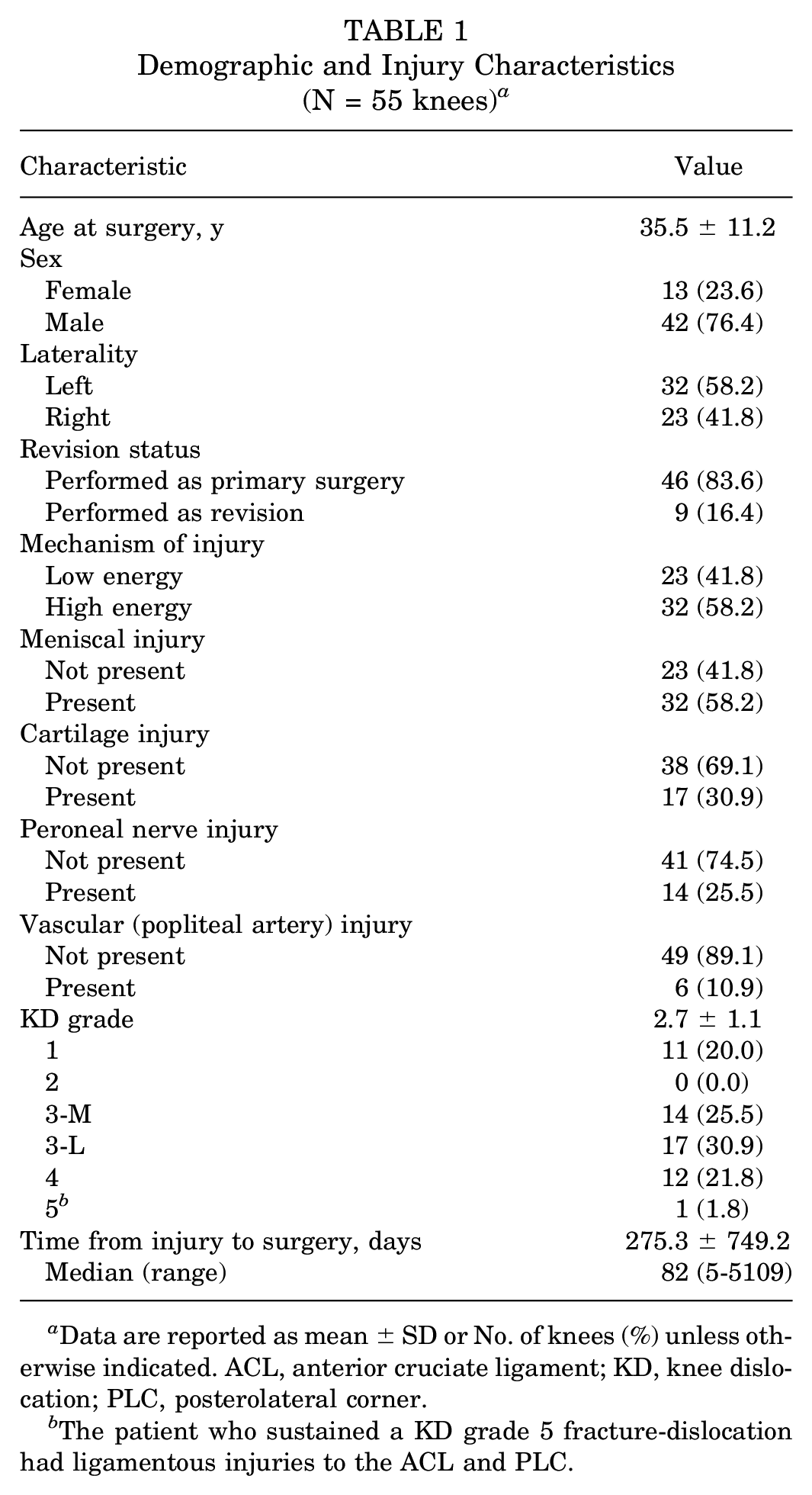
Data are reported as mean ± SD or No. of knees (%) unless otherwise indicated. ACL, anterior cruciate ligament; KD, knee dislocation; PLC, posterolateral corner.
The patient who sustained a KD grade 5 fracture-dislocation had ligamentous injuries to the ACL and PLC.
Number of Injuries and Surgeries by Ligament a

Data are reported as No. of knees (%). ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner; PMC, posteromedial corner.
Concomitant Meniscal Procedures at Time of MLKI Surgery a
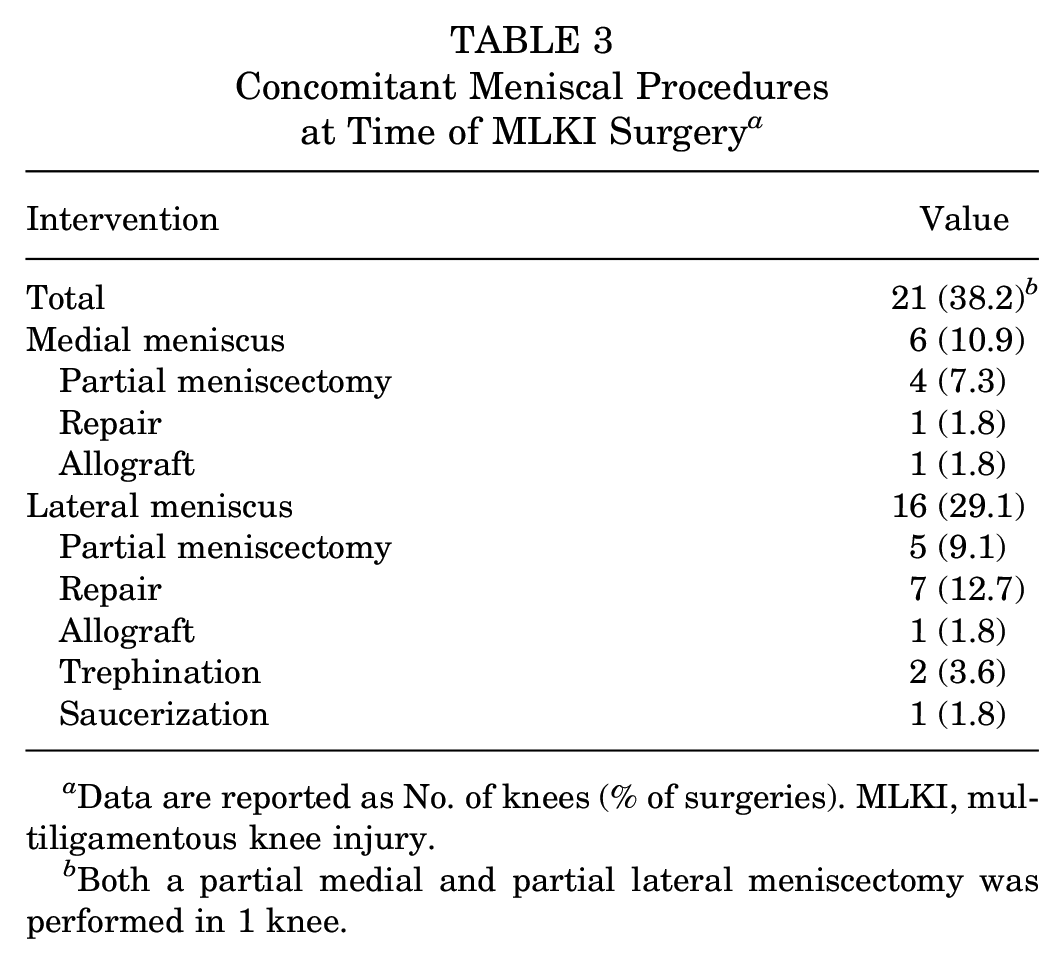
Data are reported as No. of knees (% of surgeries). MLKI, multiligamentous knee injury.
Both a partial medial and partial lateral meniscectomy was performed in 1 knee.
Long-term Outcomes
PRO scores were obtained for the 39 surviving native knees at a mean postoperative follow-up of 15.2 ± 4.8 years (range, 10-31 years) (Tables 4 and 5). Mild or significant improvement was reported in 26 of the 39 knees (66.7%) compared with preoperatively, while 12 (30.8%) reported mild or significantly worse conditions. At final follow-up, VAS for pain at rest had improved significantly from 3.9 ± 1.4 preoperatively to 1.7 ± 2.2 postoperatively (P < .001). There was also a significant decrease in Tegner score from preinjury to postoperatively (5.8 ± 2.5 vs 4.0 ± 1.6, P < .001). The majority of patients (26 of 35 knees; 74.3%) reported preference for their nonsurgically reconstructed knee over their surgically reconstructed knee; however, reports of being either being satisfied or very satisfied with their surgery were found in 32 of the 39 knees (82.0%).
Postoperative Outcomes Overall and by Age Group a

Data are reported as mean ± SD or No. of knees (%). Boldface P values indicate statistically significant difference between age groups (P < .05). FJS, Forgotten Joint Score; IKDC, International Knee Documentation Committee; VAS, visual analog scale.
Comparison between ≤30- and >30-year cohorts.
Comparison between preinjury and final follow-up scores.
IKDC and Lysholm Scores by Concomitant Injury and KD Grade a

Data are reported as mean ± SD. Boldface P value indicates statistically significant difference between groups (P < .05). IKDC, International Knee Documentation Committee; KD, knee dislocation; PRO, patient-reported outcome.
Effect of Patient Age on Outcomes
Linear regression analysis revealed 0.08-point and 0.05-point reductions in preinjury and postoperative Tegner scores, respectively, for every additional year of age at the time of MLKI surgery (P = .017 and .022). The cohort was then divided into age groups for further analysis: patients ≤30 years (n = 19) and >30 years (n = 20) at the time of surgery (Table 4). Both the ≤30- and >30-year age groups experienced significant improvements in VAS pain at rest from pre- to postoperatively (P = .029 and <.001, respectively), as well as significant decreases in Tegner scores from preinjury to postoperatively (P = .003 and <.001, respectively). Notably, patients ≤30 years had significantly higher postoperative Tegner scores than those >30 years (4.7 ± 1.6 vs 3.3 ± 1.4, P = .003), but no statistically significant difference was seen in preinjury Tegner scores between groups (P = .058). Finally, there were no significant differences in the proportions of improvement ratings, knee preference, or surgery satisfaction between the age groups (P≥ .144 for all).
Analysis of Risk Factors for Conversion to Arthroplasty
Further analyses of the 55 knees showed that a greater proportion of patients aged >30 years converted to arthroplasty compared with patients aged ≤30 years (P = .034) and that patients who converted to arthroplasty had higher KD grades at the time of MLKI surgery than those who did not (P = .043) (Table 6). Notably, when age was treated as a continuous variable, this relationship was no longer significant (P = .205), and when KD grade was treated as a factor variable instead of continuous variable the relationship was no longer significant (P = .138). Regarding the 2 knees that had undergone revision ligament reconstruction surgeries at the time of follow-up, 1 knee - in a patient who was 33.3 years old at the time of primary surgery - underwent revision PCL reconstruction 1.2 years after primary surgery. This patient reported a long history of smoking and never achieved satisfactory results after his first surgery. The other knee, in a patient 19.2 years old at the time of primary surgery, underwent revision ACL, PCL, and MCL reconstructions 16.8 years after the primary MLKI reconstruction at an age of 35.9 years. This patient did remarkably well for over a decade and was able to engage in competitive sports, including volleyball, before he started experiencing worsening instability with daily activities. Regarding arthroplasty, average time to conversion was 12.0 ± 4.9 years from the time of MLKI surgery, with a mean age of 39.5 ± 6.3 years at the time of MLKI surgery and 51.5 ± 6.0 years at the time of arthroplasty.
Analysis of Risk Factors for Conversion to Arthroplasty Using Nonparametric Testing (N = 55 knees) a

Data are reported as mean ± SD or No. of knees (%). Boldface P values indicate a statistically significant difference between groups (P < .05). KD, knee dislocation.
In addition, there were 5 knees (9.1%) that had undergone nonarthroplasty, nonrevision reoperation at the time of final follow-up. Of these reoperations, 4 were arthroscopic procedures with partial medial meniscectomies, debridement, and/or loose body removals. The final procedure was a manipulation under anesthesia with synovectomy and capsular release. The mean time from primary surgery to reoperation for these subsequent surgeries was 5.4 ± 4.4 years.
Discussion
The purpose of our study was to evaluate long-term outcomes after surgical treatment of MLKI as well as to evaluate the relationship between patient age and clinical outcomes at this timepoint. PROs remained consistent at minimum 10-years’ postoperative follow-up, and the effects of age on MLKI postoperative outcomes were nondurable at this extended follow-up timepoint. To our knowledge, these results represent one of the largest cohorts of MLKI patients treated surgically and contribute to the current understanding of MLKI patient outcomes that informs treatment, management, and patient counseling.
In this study, survey respondents overall reported subjective postoperative improvement in their knee and satisfaction with their surgery at long-term follow-up. However, patients continued to report mild-to-moderate pain in their knees, reductions in activity levels, and frequent awareness of their knee due to symptoms and/or functional limitations. There is a paucity of literature describing outcomes for this patient population at long-term follow-up; however, our results demonstrated PRO scores to similar previously published studies.22,41 To our knowledge, only 4 other studies with minimum 10-year follow-up of MLKI repair or reconstruction have been published to date. The earliest of these studies, published in 2011 by Noyes et al, 23 looked at 14 patients with a mean age of 24.4 years; however, this study was specifically looking at posterolateral femorofibular reconstruction after MLKI in patients with chronic instability and did not report on any of the same PROs as the present study. Next was a case report published by Schenck et al 31 in 2014 on 2 patients who underwent MLKI reconstruction and were evaluated for 22 years postoperatively. At the time of final follow-up, the patients reported IKDC scores of 81 and 92 and Lysholm scores of 90 and 94. The small sample sizes and variance in patient populations and surgical approach makes these first 2 studies difficult to analyze alongside the present study. However, 2 more recent studies lend themselves to such a comparison. A Norwegian study published by Moatshe et al 22 in 2017 reported on 65 patients at mean 13.1-years’ follow-up. In this study, median Tegner score was 4, mean Lysholm score was 84, and mean IKDC was 73. While Tegner scores appear similar between our studies, the Lysholm and IKDC scores appear higher in the 2017 study; the reason for this difference is not fully understood at this time. Notably, approximately 10% less of the Norwegian study population sustained a high-energy injury than in our study, which may explain some of the difference in PROs. More recently, a 2022 retrospective study by Zhang et al 41 reported on 11 MLKI patients who underwent repair or reconstruction at mean 13.1-year follow-up. In this study, mean Tegner score decreased from 7.6 to 4.5, mean Lysholm score was 64.3, and mean IKDC score was 62.1, which more closely reflect our findings. 41
Previous studies have also shown significantly decreased PROs in patients with concomitant articular, meniscal, and vascular injuries, although no difference has been shown in patients with concomitant peroneal nerve injury.13,15,27 The present study was not powered to investigate these factors, however. Of note, initial management of these traumatic knee injuries and any index surgeries before ligamentous reconstruction were not reported routinely, and it is of particular clinical interest to identify the impact of initial management on long-term outcomes. Overall, the results of our study fall within the range of expected PRO scores as presented in the 2 most comparable studies to date; however, our study does report the findings of the longest mean follow-up study internationally and the largest cohort of surgically treated MLKI patients in the United States.
Our study also reported a 3.6% rate of revision ligament surgery, 10.9% rate of progression to arthroplasty, and 9.1% rate of nonarthroplasty, nonrevision reoperation, resulting in an overall rate of 23.6% of patients progressing to some form of subsequent operation after MLKI repair or reconstruction. The rate of reoperation in our cohort was within the range of what has been previously reported in the literature, which varies from approximately 10% to 40%.5,16,33 Notably, we found a very low rate of revision ligament surgeries in our cohort, 1 isolated revision PCL reconstruction and 1 revision ACL, PCL, and MCL reconstruction at 1.2 and 16.8 years after primary MLKI reconstruction, respectively, with the majority of reoperations for management of osteoarthritis progression. This suggests that failure after MLKI surgery is likely not related to recurrent ligamentous issues but rather to overall progressive degeneration of the affected joint. There is a lack of robust information describing general rates of reoperations or arthroplasty after MLKI, particularly at extended follow-up timepoints; however, it is well documented that significant proportions of patients sustaining traumatic knee injuries or undergoing knee ligamentous surgeries will go on to develop significant osteoarthritic changes.1,22,30,34,36
Our second aim was to determine the durability of the effect of age on patient outcomes. Previous findings showed that young patient age (≤30 years) was predictive of superior clinical and functional outcome scores; however, data presented in the current study suggest that this difference is no longer significant more than 10 years after the initial operation. 19 This may be due in part to decreased levels of patient activity and physical demand with advancing age, which may function to essentially equalize expectations and performance goals across all patients, making there less likely to be a difference in reported function scores or limitations.3,37 In addition, this regression to the mean over time may represent nonlinear changes in posttraumatic arthritis development, which could potentially lead to young patients with previously nonarthritic knees developing symptomatic posttraumatic arthritis over the course of ≥10 years to the point where their knees are more similar to those of the patients in the older cohort who were more likely to have pre-existing osteoarthritis at the time of injury. 11
Overall, our findings suggest that, on average, patients have a predictable, stable postoperative course, without progressive worsening of their knee with prolonged follow-up in most cases, and that, at extended follow-up, there will be no significant difference in outcomes scores related to age at the time of injury and surgery in patients who have not required subsequent surgical interventions. Given the overall limited amount of published literature on patient outcomes after MLKI surgery; the lack of standardized treatments, definitions, and outcome scoring across research; and the high variability in patient injuries, demographics, outcomes, and experiences, it is difficult to compare outcomes across different studies. 3
Limitations
Our study is not without limitations. The relatively small sample size may have underpowered the study and accounted for the lack of significance observed in our cohort comparisons. The patients lost to follow-up may have also introduced bias in terms of the patients ultimately analyzed in the study. Given the retrospective nature of data collection in the present study, specific details of individual patients’ index procedures or graft types were not readily available. Finally, there was a lack of preoperative outcome scores for comparison, and no established guidelines for either minimal clinically important difference or Patient Acceptable Symptom State for most outcome scores in MLKI patients and given such a heterogeneous patient population. Finally, given the duration of the study period, there was an evolution in surgical techniques that introduced possible inconsistencies in surgical treatment across the cohort. In addition, the data collection methods used to maximize follow-up length were not amenable to collection objective knee stability testing, physical examination findings, or radiographs to evaluate for posttraumatic arthritis progression at the time of final follow-up.
Conclusion
The majority of the study cohort reported modest subjective improvement and were satisfied with their surgery. Gradual, but expected, age-related decreases in Tegner scores were observed, and some patients demonstrated continued symptomatic and functional limitations, but mean PRO scores remained satisfactory. Revision surgery and conversion to arthroplasty were not commonly required.
Footnotes
Final revision submitted July 9, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: research support was received from the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950) and from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. M.H. has received education payments from Medwest Associates and Smith & Nephew and hospitality payments from Medical Device Business Services. A.J.K. has received a grant from DJO; consulting fees from Arthrex, JRF Ortho, and Responsive Arthroscopy; nonconsulting fees from Arthrex; royalties from Arthrex; and honoraria from JRF Ortho and MTF Biologics. M.J.S. has received education payments from Arthrex, consulting fees from Arthrex, nonconsulting fees from Arthrex, royalties from Arthrex, and hospitality payments from Stryker. B.A.L. has received consulting fees from Arthrex and Smith & Nephew; nonconsulting fees from Arthrex, Smith & Nephew, and Linvatec; and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (reference No. 07-004018).