
Abstract
Background:
Anterior inferior iliac spine (AIIS) impingement is an important risk factor for revision hip arthroscopy. Although a morphological classification system is available, evaluating AIIS impingement with respect to joint kinematics remains a challenge.
Purpose:
To use computer simulation analysis to ascertain the prevalence of AIIS impingement before and after osteochondroplasty.
Methods:
A total of 35 joints from 30 cases (20 males and 10 females; average age: 43.3 ± 13.7 years) were analyzed. All joints had cam morphology and underwent hip arthroscopic osteochondroplasty. A three-dimensional model of each joint was constructed pre- and postoperatively. Joint kinematic simulation software (ZedHip®, Lexi, Tokyo) was used to identify the impingement point on the acetabular side and the incidence (expressed as a percentage) of AIIS impingement calculated. Radiographic and clinical evaluation was performed pre- and postoperatively.
Results:
AIIS impingement was observed postoperatively in six joints but preoperatively in only one joint. The rate of AIIS postoperative impingement was significantly higher than that of preoperative impingement. All impingement points were located on the inferior aspect of the AIIS apex. However, there were no significant differences between the AIIS impingement and non-impingement groups in terms of clinical outcome.
Conclusion:
The incidence of AIIS impingement after osteochondroplasty was 17% by computer simulation analysis. Osteochondroplasty may result in subsequent AIIS impingement.
Keywords
Introduction
Femoroacetabular impingement (FAI) is an important pathology of hip joint disorders, 1 particularly in young adults. Hip arthroscopy is a promising treatment option and is performed extensively. Osteochondroplasty for cam morphology is the most successful treatment for bony impingement associated with cam-type FAI.
In general, arthroscopic surgery for FAI has a good clinical outcome; however, some cases require revision. 2 One of the major factors associated with clinical failure is residual deformity after osteochondroplasty. 3 Removal of sufficient bone from a cam or pincer lesion is essential to avoid treatment failure. In addition to a cam or pincer lesion, impingement of the anterior inferior iliac spine (AIIS) can cause extra-articular hip impingement 4 and is a risk for revision surgery. 5 However, it is unclear how AIIS impingement occurs after osteochondroplasty for FAI. Moreover, it is not easy to verify AIIS impingement based on radiographic imaging or physical findings alone. Thus, computer simulation analysis of a three-dimensional (3D) model is a good method of identifying mechanical bony impingement at the AIIS and sub-spine area. 6
The clinical question is whether AIIS impingement may occur after osteochondroplasty. Here, we aimed to assess the prevalence of mechanical AIIS impingement after hip arthroscopic osteochondroplasty for FAI using computer simulation kinematic analysis. We then compared the short-term clinical results for patients with and without AIIS impingement.
Materials and methods
Patients
This retrospective cross-sectional study was approved by the local institutional review board and included 69 joints from 62 cases (average age: 46.3 ± 16.6 years) that underwent hip arthroscopic surgery from October 2013 to March 2017. Of these 69 joints, 15 joints with osteoarthritis (Tönnis grade 2 or higher), 11 joints without osteochondroplasty (7 with borderline developmental dysplasia of the hip (BDDH); 2 with definite DDH (center edge (CE) angle < 20°); and 2 with a labral tear without BDDH), 5 joints that had undergone hip osteotomy, and 3 joints without computed tomography (CT) data compatible with the simulation software were excluded. Therefore, 35 joints from 30 cases (20 males and 10 females; average age: 43.3 ± 13.7 years) were subjected to computer simulation and radiographic and clinical evaluation both preoperatively and postoperatively.
Definition of cam morphology and BDDH
Cam morphology was diagnosed as an alpha angle of ≥55° on cross-table lateral views, plus at least two of the following radiographic factors: a pistol grip deformity; a head neck offset ratio of ≤0.14; or herniation pits. BDDH was defined as an alpha angle of <55° and a CE angle of 20–24°. Pincer morphology was defined as a CE angle > 40° or a CE angle > 30° with an acetabular roof obliquity < 0, or a CE angle > 25° with a crossover sign.
Surgical techniques
Hip arthroscopic surgery was performed using a traction system with the patient in a supine position. Two portals (anterolateral and a mid-anterior) were used for labral repair and synovial debridement. Osteochondroplasty was performed for all joints based on information about cam morphology acquired from the preoperative simulated model. Capsular closure was performed for all joints.
Computer simulation analysis
ZedHip® (Lexi, Tokyo) software was used for computer simulation analysis to identify the specific bony impingement point in each joint. Digital imaging and communication in medicine data for each patient were transferred to ZedHip, which then created a 3D model of the acetabulum and femoral head. The functional pelvic plane was used as a reference plane for the acetabulum, taking into consideration the pelvic tilt induced by the supine position. A reference plane for the femur was drawn according to the definition of the International Society of Biomechanics. 7 Briefly, the femoral head center was defined by four reference points. The femoral plane was then set with respect to two reference points: the center of the femoral head and the midpoint of the femoral condyle. Then, segmentation between the acetabulum and the femur was performed.
Identification of the impingement point
The impingement point on the acetabular side in each joint was identified preoperatively and postoperatively by the impingement simulation at the limb positions of maximum flexion, maximum internal rotation at 90° of flexion, maximum internal rotation at 45° of flexion, and maximum adduction at 90° of flexion. The location of the impingement point on the acetabular rim or AIIS region was defined as outlined in Figure 1. Radiographic AIIS type was evaluated according to the classification by Hetsroni et al. 8
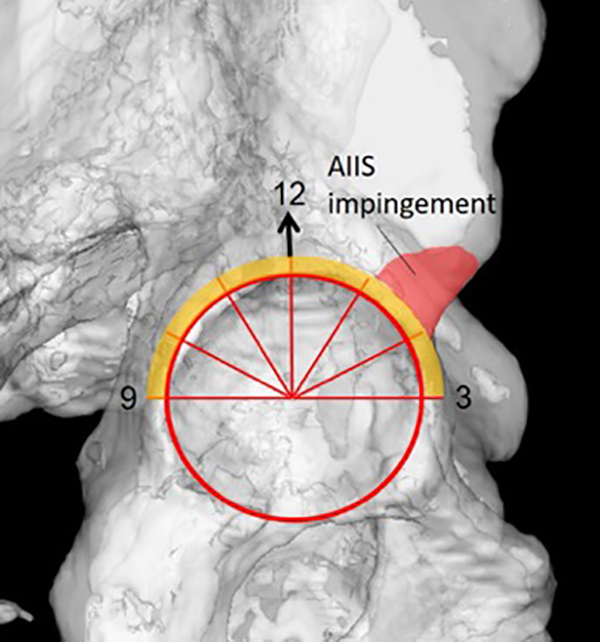
Defining the AIIS impingement area on a 3D model. AIIS impingement was diagnosed if the impingement point was located in the red zone (AIIS and sub-spinal area). Impingement on the rim (orange zone) is excluded. AIIS: anterior inferior iliac spine; 3D: three-dimensional.
Clinical evaluation
The non-arthritic hip scores and modified Harris hip scores were obtained before and at 12 months post-surgery. Hip pain (on visual analog scale) on the anterior impingement test was assessed at the same time points.
Radiographic evaluation
The alpha angle was measured in cross-table lateral views obtained pre- and postoperatively.
Statistical analysis
Occurrence of AIIS impingement, as defined by pre- and postoperative computer simulations, was assessed using the χ 2 test. Differences in patient characteristics and clinical outcome scores for the AIIS impingement and non-impingement groups were assessed using Student’s t-test.
Results
Thirty-five joints (26 cam-type FAI, 2 combined-type FAI, and 7 BDDH with cam morphology) were evaluated. Thus, all joints had cam morphology, with the average alpha angle being 63.4 ± 5.3°. After surgery, the average alpha angle was 47.5 ± 11.9°, a significant reduction (p < 0.001). Table 1 summarizes the location of impingement (in terms of a clock face) in each joint before surgery.
Distribution of bony impingement in the pelvis before surgery.

AIIS: anterior inferior iliac spine.
AIIS impingement was identified in one joint (3%) at 45° flexion and maximum internal rotation. Table 2 summarizes the location of impingement after surgery.
Distribution of bony impingement in the pelvis after surgery.

AIIS: anterior inferior iliac spine.
AIIS impingement was recognized in 6% by maximum flexion, 6% by 90° flexion and maximum internal rotation, and 9% by 45° flexion and maximum internal rotation.
Table 3 presents the overall incidence of AIIS impingement pre- and post-surgery. AIIS impingement occurred in six joints (17%) postoperatively. There was a significant difference in the incidence of AIIS impingement between the pre- and postoperation (p = 0.043) groups. Figure 2 shows the location of AIIS impingement in the pre- and postoperative 3D model.
Incidence of AIIS impingement pre- and post-surgery.

AIIS: anterior inferior iliac spine.

Location of AIIS impingement in each joint. Eight simulations (one preoperatively, seven postoperatively) performed for six joints identified the location of AIIS impingement. All impingement points were located on the inferior aspect of the AIIS apex (sub-spine region). AIIS: anterior inferior iliac spine.
Table 4 summarizes differences in the characteristics and clinical outcomes of the AIIS impingement and non-impingement groups.
Differences in the characteristics and postoperative clinical outcomes of the AIIS impingement and non-impingement groups.

AIIS: anterior inferior iliac spine; BMI: body mass index; VAS: visual analog scale; NAHS: non-arthritic hip score; mHHS: modified Harris hip scores.
There were no significant differences between the two groups in terms of characteristics or clinical outcome.
Figure 3 shows the radiographic findings and location of impingement in a representative case of postoperative AIIS impingement.
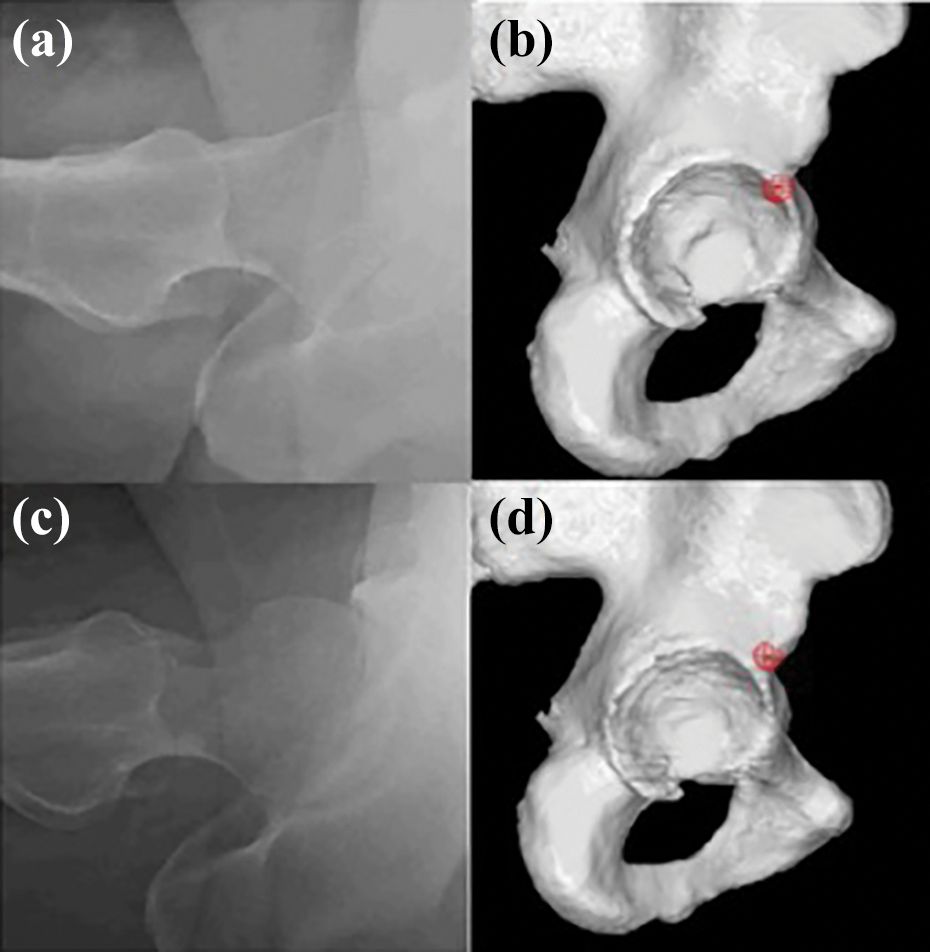
A representative case of AIIS impingement after osteochondroplasty. The case is a 45-year-old man with borderline dysplasia and cam morphology. (AIIS type 2, according to the Hetsroni classification). 8 The preoperative alpha angle was 60° (a), and the computer simulation identified the impingement point on the acetabular rim at the midway between the 1 o’clock and 2 o’clock positions. (b) After arthroscopic osteochondroplasty, the alpha angle was reduced to 54°. (c) Postoperative plain radiograph shows resected cam lesion. (d) Postoperative computer simulation identified the AIIS impingement. AIIS: anterior inferior iliac spine.
Discussion
Here, a computer simulation predicted that AIIS impingement may occur in approximately 17% of joints after arthroscopic osteochondroplasty. Also, the results suggest that AIIS impingement may occur after actual osteochondroplasty for FAI cases. The implication is that AIIS impingement may occur after osteochondroplasty, even in cases in which AIIS impingement did not exist preoperatively.
Pan et al. were the first to report a case of extra-articular hip impingement due to hypertrophic AIIS, which was treated by open surgical resection. 9 Since then, arthroscopic treatment of AIIS impingement has been reported by Larson et al. 10 This group reported three cases of AIIS or sub-spine impingement, which they treated with arthroscopic decompression. In addition, identification of AIIS or sub-spine impingement is an important factor for a satisfactory outcome after revision hip arthroscopic surgery. 5 Sporting activities such as soccer may induce development of AIIS morphology. 11 Thus, we need to recognize the existence of AIIS impingent pathology in certain cases, although its clinical prevalence is not clear. Indeed, Balazs et al. report that AIIS morphology is similar in both symptomatic and asymptomatic individuals. 12 This means that, in some cases, AIIS morphology is asymptomatic. Thus, radiographic assessment of AIIS morphology is not a reliable method on which to base the decision to treat.
Radiographic evaluation has a role to play in screening for abnormal AIIS morphology 13 ; however, such static modalities are not a reliable means of diagnosing actual bone impingement. Therefore, several studies used dynamic computer simulation analyses to identify the impingement point 6,14 or predict range of motion. 15 For instance, the impingement point on the femoral side in cam-type FAI is distributed across various regions. 14 Previous studies did not focus on the impingement point on the acetabular side. Hetsroni et al. 8 were the first to use CT imaging and 3D simulations to examine AIIS impingement. They classified AIIS morphology into three types based on the relationship between the distal extension of the AIIS and the anteroposterior acetabular rim on CT images. This classification system is a simple and reasonable way to assess AIIS morphology related to impingement, that is, type III AIIS is associated with a higher risk of AIIS impingement. In fact, simulation studies showed that the flexion angle in type III AIIS was significantly lower than that observed in other AIIS types. 8 However, the cohort examined herein contained no cases with type III AIIS. By contrast, we identified AIIS impingement even in type I cases. Thus, both morphology and dynamic assessment are important factors to consider when identifying AIIS impingement.
It is important to note that we used computer simulation to evaluate the incidence of AIIS impingement after arthroscopic osteochondroplasty. Although we identified only one joint with AIIS impingement before surgery, the prevalence of AIIS increased after surgery. With respect to cam morphology, impingement usually occurs before AIIS impingement. However, increased range of motion (ROM) after osteochondroplasty might result in subsequent AIIS impingement. Actually, we confirmed certain improvement of ROM after cam resection by computer simulation in most of cases. Although we did not identify significant differences of clinical outcome between those with and without AIIS impingement, the follow-up period is limited and only one case with AIIS impingement after surgery suffered recurrence of severe hip pain at 6 months. Although this case showed excellent improvement of ROM at 3 months after surgery, this improvement might result in subsequent AIIS impingement. To the contrary, rest of the cases might not achieve enough improvement of ROM till AIIS impingement occur. Thus, it should be noted that AIIS impingement may occur after a sufficient improvement in ROM post-osteochondroplasty in FAI cases. We identified the location of impingement point on the acetabular rim. In maximum flexion and maximum internal rotation at 90° of flexion (a position that commonly induces symptoms of AIIS impingement), the impingement point in the majority of cases was located between 1 o’clock and 2 o’clock. This “anterolateral region” is located just below the AIIS/sub-spine area. This may be the cause of AIIS impingement after osteochondroplasty. This is reasonable given that isolated AIIS impingement can occur even in the absence of FAI. 16
The study has several limitations. First, this is a simulation study based on CT data; therefore, it is impossible to evaluate impingement caused by soft tissue. Because the AIIS is an attachment point for the rectus femoris muscle, 17 impingement of the rectus femoris may occur before bony impingement. In this case, the computer simulation may underestimate the prevalence of AIIS impingement. Furthermore, joint kinematics were limited (i.e. flexion, adduction, and internal rotation). Other studies should use 3D motion analysis to examine AIIS impingement that may occur during daily or sporting activities.
In conclusion, we used computer simulation to investigate the prevalence of AIIS impingement both before and after arthroscopic osteochondroplasty. The incidence of AIIS impingement increased significantly after osteochondroplasty, resulting in an overall prevalence of approximately 17%.
Footnotes
Acknowledgements
The authors would like to thank Mirai Takahashi for help with the computer simulation study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.