
Abstract
Background:
Hip arthroscopy (HA) procedures have increased exponentially in recent years. Their effect on outcomes after subsequent total hip arthroplasty (THA) remains unclear.
Purpose:
To compare rates of complications and opioid claims after elective THA among patients with prior HA versus controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent THA were identified in the PearlDiver database. Arthroplasty performed for hip fractures and hip avascular necrosis were excluded. Within this population, patients with HA before arthroplasty (n = 3156) were propensity score matched 1:1 with controls on age, sex, US region, and several comorbidities. Rates of medical complications within 90 days and prosthesis-related complications within 2 years were queried. The number of patients with an opioid claim within 0 to 30 days and subsequent opioid claim(s) during the 90-day global period were obtained to assess rates of prolonged opioid use after arthroplasty. Rates of postoperative complications and opioid claims were compared using logistic regression.
Results:
Patients with prior HA exhibited significantly lower rates of readmission (5.6% vs 7.3%; odds ratio [OR], 0.72), pulmonary embolism (0.2% vs 0.6%; OR, 0.45), urinary tract infection (3.1% vs 4.0%; OR, 0.75), and blood transfusion (3.6% vs 6.1%; OR, 0.55). The prior HA cohort also exhibited a significantly lower rate of prosthetic joint infection at 1 year postoperatively (0.6% vs 1.3%; OR, 0.50). Rates of dislocation, periprosthetic fracture, mechanical complications, and aseptic revision arthroplasty were statistically comparable between the cohorts within 2 years. The prior HA cohort was significantly less likely to file persistent opioid claims after 30 days postoperatively, including between 31 and 60 days (27.2% vs 33.1%; OR, 0.74) and 61 to 90 days (16.2% vs 20.9%; OR, 0.71).
Conclusion:
After elective THA, patients with prior HA exhibited significantly lower rates of medical complications and prolonged opioid claims within 90 days and prosthetic joint infection at 1 year. Rates of all other prosthesis-related complications within 2 years were statistically comparable.
Over the past decade, utilization of hip arthroscopy (HA) for diagnosing and treating prearthritic diseases such as acetabular labral tears and femoroacetabular impingement syndrome has increased exponentially. 9,11,24 With over 70,000 procedures performed each year in the United States, 59 HA has been demonstrated to be a safe and effective treatment modality with expanding indications. 9,48,61 In addition, clinical and functional outcomes after HA continue to improve secondary to patient selection, surgeon experience, and advances in HA techniques and technology. 9
Despite the demonstrated efficacy of HA, some patients require eventual conversion to total hip arthroplasty (THA). A recent systematic review reported pooled rates of conversion to THA between 2.4% and 41.0% at a mean time of 46.9 to 96 months after HA, 42 though other analyses have reported shorter conversion times between 1.12 and 3.09 years. 27,43,44,67 Several risk factors for conversion to THA have been identified, including obesity, female sex, and HA performed at a low-volume HA center. 16,30,36,52,56,57 Prior studies have examined outcomes of THA following previous ipsilateral HA with variable results. Some analyses have reported patients with prior HA exhibit significantly increased risk of postoperative complications and revision surgery after THA, 25,44 whereas other studies have reported no differences in patient-reported outcomes or complication rates. 46 There are also minimal data on the effect of prior HA on pain and risk of prolonged opioid use after THA. 38 However, prior studies have been limited by small sample sizes, selection bias, and/or methodological design. Therefore, the true relationship between prior HA and outcomes following THA remains unclear.
Given the variable results and methodological limitations of prior studies, the purpose of this study was to compare rates of complications and opioid claims following elective THA for patients with prior HA versus matched controls. It was hypothesized that complication rates would be comparable between the cohorts and that opioid claim rates would be higher for patients with prior HA.
Methods
Database Information
Patient records were obtained from the PearlDiver Mariner Database (PearlDiver Technologies), a commercially available administrative claims database that contains medical records of 144 million patients across the United States between January 1, 2010, and September 30, 2020. The data set analyzed in this study, called “MHip,” contains a random sample of approximately 1.3 million patients with diagnoses and procedures localized to the hip. All health insurance payors are represented. Current Procedural Technology (CPT) and International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10), codes were used to identify relevant patients and outcomes. Institutional review board exemption was granted for this study, as the data analyzed were deidentified and compliant with the Health Insurance Portability and Accountability Act.
Defining Patient Cohorts
A retrospective matched cohort study was conducted to evaluate the effect of HA procedures before elective THA on rates of postoperative complications and opioid claims. THA was defined by CPT-27130 and corresponding ICD-9/ICD-10 procedural codes. For the HA cohort, CPT-27132 (ie, conversion of previous hip surgery to THA) was also used to define THA. Only THA procedures performed before October 1, 2018, were eligible for inclusion to allow for a minimum 2-year follow-up in the database. Pediatric patients and patients with hip fractures, femoral head avascular necrosis, or local infectious processes on the same day as THA were excluded. Similar to previous studies, patients with prior hemiarthroplasty and those who underwent simultaneous bilateral THA, staged bilateral THA, or contralateral hemiarthroplasty during the 2-year follow-up were excluded to ensure complications tied back to the index THA. In addition, patients with end-stage renal disease or metastatic cancer were excluded.
Subsequently, the HA cohort was defined as patients who received THA and had a record of HA before THA. HA was defined using CPT codes for HA procedures paired with ICD-10 diagnosis codes for hip pathology with laterality specified (eg, left or right hip cartilage disorders, labral tears). Patients with bilateral hip pathology at the time of HA were excluded to help ensure ipsilaterality of the HA and THA procedures. The control cohort was defined as patients who received THA with no record of prior HA. Codes used to define all inclusion and exclusion criteria are available in Supplemental Table S1, available separately.
Demographic Data and Outcomes
Baseline demographic and clinical characteristics were obtained for all patients, including age, sex, body mass index (BMI), US region, mean Elixhauser Comorbidity Index (ECI) score, and rates of several comorbidities. ECI is a risk adjustment tool based on comorbidities defined by ICD diagnosis codes and is commonly used as a predictor of in-hospital mortality and resource use. 58 Using generic drug codes for the most commonly prescribed transdermal and oral opioid medications (Supplemental Table S2), the prevalence of at least 1 opioid claim within 1 year before THA was also queried for both cohorts to assess preoperative opioid exposure.
Rates of prosthesis-related complications were queried at 1 and 2 years after THA. Complications assessed included prosthetic joint infection (PJI), prosthetic dislocation, periprosthetic fracture, other mechanical complications, and aseptic revision THA. PJI was defined by diagnosis codes for hip PJI and other deep infectious processes paired with procedural codes to isolate cases of infection warranting surgical intervention and exclude superficial wound complications. Procedures for PJI included incision and drainage procedures, revision THA, explantation of the prosthesis, and insertion/removal of an antibiotic spacer. Other mechanical complications included implant loosening, stiffness, breakage, and other unspecified mechanical complications. Aseptic revision THA included implant removal, liner exchange, and revision of the femoral and/or acetabular components without concomitant antibiotic spacer insertion/removal or PJI diagnosis codes.
Rates of inpatient readmission and medical complications within the 90-day global postoperative period were queried. Medical complications assessed included deep vein thrombosis, pulmonary embolism (PE), urinary tract infection (UTI), acute kidney injury, and blood transfusion. The codes used to define complications are available in Supplemental Table S3.
To compare rates of prolonged opioid use after THA, generic drug codes for common opioid medications were used to quantify the number of patients who filed at least 1 opioid claim during each of the following postoperative time intervals: (1) 30 days, (2) 31 to 60 days, and (3) 61 to 90 days. Patients who filed opioid claims in later time intervals were only included if they had filed at least 1 claim in each previous time interval to assume persistent opioid use and that all identified opioid claims tied back to the index THA. Median cumulative morphine milligram equivalents (MMEs) prescribed on all opioid claims after the index THA procedure was obtained at 30 days, 60 days, and 90 days postoperatively. MME was calculated directly by the PearlDiver software by converting the total units of each opioid drug into MME using standard conversion factors as outlined by the Centers for Disease Control and Prevention. 19
Study Population
A total of 606,531 patients who underwent elective THA were identified, including 3156 (0.5%) patients with HA before THA (Figure 1). To reduce confounding bias, propensity score matching was performed at a fixed 1:1 ratio and a caliper 0.20 to achieve nearest neighbor matching without replacement. 2 The cohorts were matched on age, sex, US region, tobacco use, diabetes mellitus, depression, obesity, chronic kidney disease, dementia, and rheumatoid arthritis. Similar to prior studies, these variables were selected as many have been associated with complications after THA. 29,41,43,47,60,62

Flowchart illustrating identification of study cohorts. AVN, avascular necrosis; HA, hip arthroplasty; THA, total hip arthroplasty.
After matching, all 3156 patients with prior HA were matched 1:1 with 3156 controls without a record of HA before THA (Table 1). Mean time between HA and THA in the prior HA cohort was 2.17 ± 1.87 years. Patients with prior HA had a significantly higher mean ECI score (3.50 vs 3.28; P = .001). The distribution of BMI also differed, though only 35.6% of included patients had available BMI data. Within 1 year before THA, 2171 (68.8%) patients with prior HA and 2112 (66.9%) controls had at least 1 opioid claim (P = .118).
Baseline Demographic Data and Clinical Characteristics for the Matched Cohorts a

a Boldface P values indicate statistically significant difference between groups (P < .05). BMI, body mass index; ECI, Elixhauser Comorbidity Index; HA, hip arthroplasty.
b Region data were available for 99% of patients in both cohorts.
c BMI data were available for 1096 (34.7%) patients in the prior HA cohort and 1153 (36.5%) patients in the control cohort.
d Patient count reported as “-1” by PearlDiver since the true size is <11. A cohort size of 5 (median between 1 and 10) was assigned in such instances.
e At least 1 prescription claim for an opioid medication within 1 year before total hip arthroplasty.
In the 3156 patients with prior HA, 5570 HA procedures were billed for (Table 2). The most common procedures were debridement (42.8%), femoroplasty (34.7%) and CPT-29999 indicating an “unlisted arthroscopy procedure” (27.7%). CPT-29999 is used to bill for various HA procedures including, but not limited to, repair of gluteus medius or minimus tears, recalcitrant trochanteric bursitis, and femoral neck osteoplasty. 20
Breakdown of Hip Arthroscopic Procedures in the Prior HA Cohort a

a CPT, Current Procedural Technology; ICD, International Classification of Diseases, Ninth Revision (ICD-9) and Tenth Revision (ICD-10); HA, hip arthroscopy.
b All identified patients with a record of CPT-29999 underwent an unlisted arthroscopic procedure for hip pathology defined via ICD-9/10 diagnosis codes.
Statistical Analysis
Statistical analyses were performed using R statistical software (Version 4.1.0; R Project for Statistical Computing, Vienna, Austria) integrated within the PearlDiver software and Microsoft Excel (Microsoft, Redmond, WA, USA) with an α level set to .05. Categorical variables were compared using chi-square analysis and continuous variables were compared using the Welch t test or the Mann-Whitney U test. Rates of postoperative complications were compared via multivariable logistic regression controlling for age, sex, BMI, and ECI. Odds ratios (ORs) and corresponding 95% CIs were calculated for each outcome. To further investigate the effect of age, subgroup analyses of postoperative complication rates were performed for patients aged younger and older than the mean age observed in both cohorts: (1) 18 to 55 years and (2) 56 years and older.
Rates of postoperative opioid claims were compared with logistic regression adjusting for age, sex, BMI, ECI, and preoperative opioid exposure within 1 year before THA. A subgroup analysis was also performed for patients from both cohorts without opioid exposure (ie, opioid-naïve) within 1 year before THA. Median cumulative MMEs prescribed within 30, 60, and 90 days postoperatively was compared using the Mann-Whitney U test.
Results
Complications
Within 90 days postoperatively, patients with prior HA exhibited significantly lower rates of inpatient readmissions (5.6% vs 7.3%; OR, 0.72 [95% CI, 0.59-0.89]), PE (0.2% vs 0.6%; OR, 0.45 [95% CI, 0.20-0.96]), UTI (3.1% vs 4.0%; OR, 0.75 [95% CI, 0.57-0.98]), and blood transfusions (3.6% vs 6.1%; OR, 0.55 [95% CI, 0.43-0.70]). Significantly lower rates of readmission, PE, UTI, and blood transfusions were also found for patients with prior HA in a subgroup analysis of patients aged 18 to 55 years (P < .05 for all). Among patients aged 56 years or more, only rates of blood transfusion were significantly lower in the prior HA cohort. The rates of postoperative complications at 90-day, 1-year, and 2-year follow-up are outlined in Appendix Table A1.
At 1 year postoperatively, rates of PJI were significantly lower in the prior HA cohort (0.6% vs 1.3%; OR, 0.50 [95% CI, 0.28-0.84]). The same result was found in a subgroup analysis of patients aged 18-55 years (0.5% vs 1.5%; OR, 0.37 [95% CI, 0.19-0.65]), while among patients aged ≥56 years, rates of PJI at 1-year follow-up were not significantly different between the cohorts. Rates of PJI at 2 years and all other prosthesis-related complications at both 1 and 2 years were also not significantly different between the cohorts.
Postoperative Opioid Claims
Patients with prior HA were significantly less likely than patients without prior HA to file opioid claims beyond 30 days postoperatively (Figure 2). Despite a similar proportion of patients filling at least 1 opioid prescription within the first 30 days after THA (71.5% vs 73.8%; P = .109), patients with prior HA were significantly less likely to file a subsequent opioid claim between 31 and 60 days (27.2% vs 33.1%; OR, 0.74 [95% CI, 0.66-0.84]) and another opioid claim between 61 and 90 days (16.2% vs 20.9%; OR, 0.71 [95% CI, 0.61-0.81]) (Table 3). Median cumulative MMEs prescribed within 30 days postoperatively was significantly lower for patients with prior HA (823 vs 900; P = .008) (Table 4).

Rates of prolonged opioid claims during the 90-day global postoperative period. Statistically significant difference compared with no prior HA. *P < .01, **P < .001. HA, hip arthroplasty.
Comparison of Proportion of Patients With at Least 1 Opioid Claim Between 0 and 30 Days, 31 and 60 Days, and 61 and 90 Days After THA a
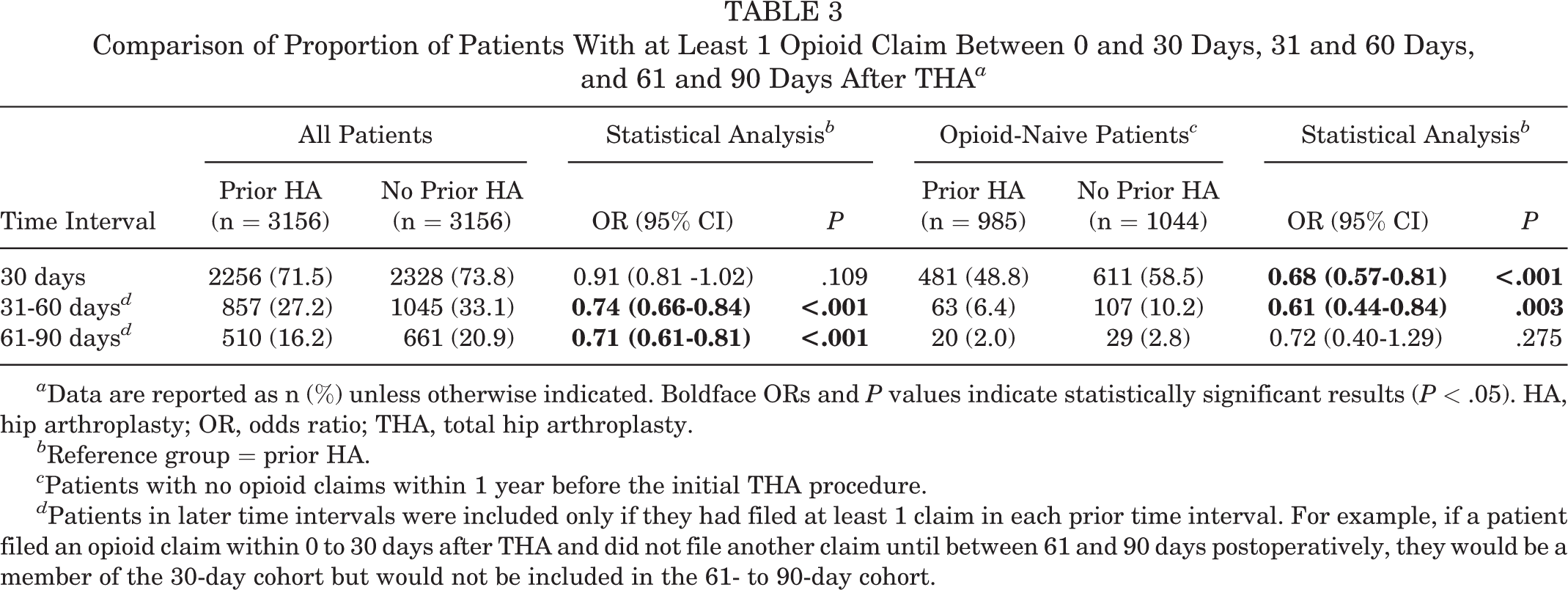
a Data are reported as n (%) unless otherwise indicated. Boldface ORs and P values indicate statistically significant results (P < .05). HA, hip arthroplasty; OR, odds ratio; THA, total hip arthroplasty.
b Reference group = prior HA.
c Patients with no opioid claims within 1 year before the initial THA procedure.
d Patients in later time intervals were included only if they had filed at least 1 claim in each prior time interval. For example, if a patient filed an opioid claim within 0 to 30 days after THA and did not file another claim until between 61 and 90 days postoperatively, they would be a member of the 30-day cohort but would not be included in the 61- to 90-day cohort.
Median Cumulative MMEs Prescribed on All Opioid Claims Filed by Patients at 30 Days, 60 Days, and 90 Days After THA a

a Data are reported as median (interquartile range). Boldface P value indicates statistically significant difference between groups (P < .05). HA, hip arthroplasty; MME, morphine milligram equivalent; THA, total hip arthroplasty.
b Patients with no opioid claims within 1 year before the initial THA procedure.
c Patients in later time intervals were only included if they had filed at least 1 claim in each prior time interval. At each follow-up, MME values represent median total MMEs prescribed on all claims filed by patients since the date of the index THA.
In a subgroup analysis of opioid-naïve patients, patients with prior HA were significantly less likely to file an opioid claim within the first 30 days after THA (48.8% vs 58.5%; OR, 0.68 [95% CI, 0.57-0.81]). Rates of at least 1 subsequent opioid claim between 31 and 60 days were also significantly lower in the prior HA cohort (6.4% vs 10.2%; OR, 0.61 [95% CI, 0.44-0.84]), although rates of further opioid claims between 61 and 90 days were statistically comparable (2.0% vs 2.8%; OR, 0.72 [95% CI, 0.20-1.29]). Median cumulative MMEs prescribed was not significantly different at any follow-up during the global period.
Discussion
Volume of hip preservation procedures including HA has increased exponentially in recent decades with the possibility of prolonging the development of end-stage osteoarthritis and consequential need for THA. 14 The principle of repairing early-stage degenerative lesions is well established in knee arthritis, 39 and, therefore, it is theorized that arthroscopic interventions may yield similar results in the hip. For example, femoroacetabular impingement has been heavily correlated with early osteoarthritis, 4,40 and favorable functional outcomes have been reported following HA. 21,34 However, the efficacy of HA in actually preventing progression to end-stage osteoarthritis is unclear. 3 ,32, 37
For patients who require conversion to THA, the relationship between prior HA and risk of adverse outcomes after THA remains unclear. Malahias et al 44 examined 2-year outcomes of THA in patients with Medicare who underwent prior HA performed for osteoarthritis and found that rates of all-cause revision THA, PJI, dislocation, and loosening were significantly higher relative to matched controls. Increased complication risk has been attributed to scar formation, heterotopic ossification, and abnormal tissue planes following HA, which can lead to implant malpositioning and poor soft tissue tensioning during THA. 49,64,68 Capsular repair during HA may also influence outcomes. Hip capsulotomy without repair can cause increased hip range of motion with resultant instability, leading to increased risk of poor functional outcomes, conversion to THA, and prosthetic dislocation. 1,8,50
However, several studies have reported no differences in clinical 13,31 or patient-reported functional outcomes after THA for patients with and without prior HA. 26,27,51 In an analysis of 1940 patients with prior HA, Lemme et al 43 reported no significant differences in rates of PJI, periprosthetic fracture, or other mechanical complications compared with matched controls. In the present analysis, patients with prior HA exhibited a significantly lower rate of PJI within 1 year and comparable rates of prosthesis-related complications within 2 years compared with controls. With respect to PJI, our results may differ from those of Lemme et al based on differences in how PJI was defined. Lemme et al used diagnosis codes to define PJI whereas we used both diagnosis and procedural codes, the latter having demonstrated superior sensitivity and positive predictive value in validation studies. 35 Our results may differ from those of Malahias et al 44 because their patient population was markedly older (82% were >65 years at the time of THA, whereas 54% of our population was <56 years), exclusively insured by Medicare, and limited to patients with osteoarthritis at the time of HA. Older age and osteoarthritis have been established as predictors of both HA failure and adverse outcomes after conversion to THA. 12,15,18,63 The marked differences in our results compared with an analysis limited to older patients who underwent HA for osteoarthritis may support the conclusions made in previous studies regarding the limited utility of HA in patients with significant osteoarthritis. 15,18,44,63,66 Nonetheless, these data suggest that prior HA is not universally associated with increased rates of short-term prosthesis-related complications after conversion to THA relative to age-, sex-, and comorbidity-matched controls without prior HA. Future studies are needed to characterize the effect of prior HA on longer-term outcomes of conversion THA.
The present analysis also found significantly lower or statistically comparable rates of medical complications within 90 days postoperatively among patients with prior HA relative to matched controls. Significantly lower rates of PE, UTI, and transfusions differs from prior studies reporting similar rates of these complications between patients with prior HA and controls. 13,43,67 Patients with prior HA also exhibited a significantly lower rate of readmissions, which may be secondary to higher short-term rates of medical complications and PJI in the control cohort. Patient selection for HA may also influence rates of medical complications as most patients undergoing HA are generally young, with presumably high activity levels. 69 It is possible that quicker return to activity and higher postoperative activity levels in the prior HA cohort were associated with lower rates of PE and UTI. Prolonged immobilization after surgery is a known risk factor for thrombotic events, 28 while early activity is a key preventative strategy. Conversely, patient factors associated with lower activity levels such as increased age, obesity, and certain neurological pathologies, such as sciatic nerve palsy, are relative contraindications to HA and may increase complication risk after THA. 10,33,54,62 However, as the cohorts were matched on age, obesity, and several comorbidities, the factors underlying the differences in rates of medical complications between the cohorts are unclear.
Previous analyses have compared postoperative pain levels after THA for patients with and without prior HA using patient-reported data. Konopka et al 38 reported that prior HA was associated with significantly lower Western Ontario and McMaster Universities Osteoarthritis Index pain scores and patient satisfaction after THA. However, in this study, patients with prior HA exhibited significantly lower rates of prolonged opioid claims after the first 30 days following THA. Given that both cohorts exhibited comparable rates of preoperative opioid use, it is possible that this result was driven by the significantly higher cumulative MMEs prescribed to the control cohort within the first 30 days postoperatively. Conversely, in the subgroup analysis of opioid-naïve patients, cumulative MMEs prescribed during the first 30 days and rates of persistent opioid claims after 60 days were statistically comparable between the cohorts. Numerous analyses have demonstrated that higher amounts of opioids prescribed in the acute postoperative period significantly increases risk of prolonged use. 5,55 These data highlight the importance of performing a comprehensive preoperative assessment of opioid exposure and tolerance, as opioid prescribing after elective arthroplasty can increase risk of prolonged dependence, especially in patients with opioid use before arthroplasty. 6,7,53 Though not optimal for managing arthritic pain, 17 opioids are still commonly prescribed before patients seek arthroplasty. 65 In addition, as previous work has demonstrated no association between the magnitude of opioid consumption and patient satisfaction scores following total joint arthroplasty, 22,23 minimizing MMEs prescribed postoperatively and maximizing utilization of multimodal analgesia protocols are paramount to decrease risk of chronic opioid dependence after THA.
Limitations
There are several limitations to this study. As the “MHip” data set within the PearlDiver database includes only a random sample of patients from a specific population with claims during a certain time period within the United States, sampling bias is present. In addition, given the limited time frame of data available in the database, patients with HA procedures before 2010 could not be identified, which limits the prior HA cohort to only patients with conversion to THA in the short to medium term after HA. Conversely, it is also possible that patients who received HA before 2010 could have been included in the control cohort. However, as recent analyses have reported mean times to conversion THA between 1.12 and 3.09 years, 27,43,44,67 the effect of this limitation is likely minimal.
With the complex nature of medical billing, there is a possibility of coding bias through manual entry of diagnosis/procedural codes. This limitation is mitigated by the large, nationally representative population of included patients such that the potential effect is likely minimal and equally affects both cohorts. Diagnostic indications for HA were defined with ICD-10 diagnosis codes exclusively to ensure the HA and THA procedures were ipsilateral; consequently, some eligible patients with prior HA may have been excluded if they received an ICD-10 diagnosis without laterality specified (eg, M16.10 indicates “unilateral primary osteoarthritis, unspecified hip”). In addition, granular information such as radiographic data at the time of HA/THA, surgical approach used for THA, and operative time were unavailable. Therefore, it was not possible to assess the severity of pathology warranting HA and the progressive arthritic changes leading to THA, match patients based upon radiographic data and surgical approach, or investigate possible differences in operative time. Nonetheless, through application of exhaustive exclusion criteria including THA performed for hip fractures or avascular necrosis, it is very likely that all included patients underwent elective THA.
Functional outcomes data and patient activity levels were also unavailable in the database, preventing complete characterization of postoperative outcomes. Surgeon HA procedure volume and rates of capsular repair during HA were also unavailable in the database, which may affect outcomes. 8,45 In addition, although researchers can quantify rates of readmission after a defined start point, the PearlDiver software does not provide conclusive information on reasons for readmission. Therefore, it was not possible to further investigate the significantly higher rate of readmission in the control cohort though this result may be secondary to higher rates of medical complications and PJI in the short term. Although propensity score matching and multivariable logistic regression were used to control for confounding bias, these factors and other unknown confounders could have influenced the results. BMI data were also unavailable for all included patients and therefore the adjustment for BMI was incomplete.
With respect to the analysis of postoperative opioid claims, an important limitation is that claims data do not contain information regarding how much of an opioid prescription is actually consumed by patients, nor does it provide information on opioids obtained without an associated insurance claim. Furthermore, only outpatient (ie, postdischarge) drug claim information is available in PearlDiver. Therefore, opioids administered during surgery, in the postanesthesia care unit, or postoperatively via a patient-controlled anesthesia pump before discharge are not captured in the database and could have influenced the results. In addition, it is possible that some patients were prescribed opioids for pain unrelated to the THA procedure. This limitation was mitigated by requiring patients with opioid claims in later time intervals to have filed consecutive opioid claims in each previous 30-day interval to be recognized as having prolonged use. Another limitation is that other possible therapeutic interventions that may be performed before THA (eg, steroid injections) were not evaluated. Last, the use of intraoperative nerve blocks and other non-opioid analgesics after THA were not assessed, and their effect on opioid claim rates is unknown.
Conclusion
Compared with matched controls, patients with HA before THA exhibited significantly lower rates of medical complications and prolonged opioid claims during the 90-day global period and PJI within 1 year postoperatively. Rates of all other prosthesis-related complications were statistically comparable between the cohorts within 2 years. These data suggest prior HA is not associated with increased short-term rates of complications or prolonged opioid use following eventual total hip arthroplasty.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671221126508.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221126508 - Is Prior Hip Arthroscopy Associated With Higher Complication Rates or Prolonged Opioid Claims After Total Hip Arthroplasty?: A Matched Cohort Study
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221126508 for Is Prior Hip Arthroscopy Associated With Higher Complication Rates or Prolonged Opioid Claims After Total Hip Arthroplasty?: A Matched Cohort Study by Bailey J. Ross, Ryan J. Wortman, Olivia C. Lee, Alfred A. Mansour, Wendell W. Cole and William F. Sherman in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted June 30, 2022; accepted July 27, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.A.M. has received education payments from Medinc and hospitality payments from Organogenesis and Stryker. W.F.S. has received honoraria from Encore Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Tulane University (ref No. 2021-925).
APPENDIX
Rates of Postoperative Complications at 90-Day, 1-Year, and 2-Year Follow-up

| Complication | Prior HA |
No Prior HA |
Statistical Analysis b | |
|---|---|---|---|---|
| OR (95% CI) | P | |||
| 90-Day Follow-up | ||||
| Inpatient readmission | 178 (5.6) | 231 (7.3) |
|
|
| Age 18-55 years | 99 (5.8) | 132 (7.7) |
|
|
| Age ≥56 years | 79 (5.5) | 99 (6.8) | 0.76 (0.56-1.04) | .082 |
| DVT | 13 (0.4) | 5 (0.2) c | 1.49 (0.64-3.67) | .377 |
| Age 18-55 years | 5 (0.3) c | 5 (0.3) c | 1.81 (0.6-6.02) | .314 |
| Age ≥56 years | 5 (0.3) c | 5 (0.3) c | 1.03 (0.24-4.36) | .971 |
| PE | 5 (0.2) c | 20 (0.6) |
|
|
| Age 18-55 years | 5 (0.3) c | 11 (0.6) |
|
|
| Age ≥56 years | 5 (0.3) c | 9 (0.6) | 0.67 (0.22-1.88) | .474 |
| AKI | 38 (1.2) | 40 (1.3) | 0.95 (0.60-1.25) | .796 |
| Age 18-55 years | 10 (0.6) | 14 (0.8) | 0.70 (0.30-1.59) | .409 |
| Age ≥56 years | 28 (1.9) | 26 (1.8) | 1.08 (0.63-1.88) | .795 |
| 90-Day Follow-up | ||||
| UTI | 99 (3.1) | 127 (4.0) |
|
|
| Age 18-55 years | 47 (2.7) | 66 (3.9) |
|
|
| Age ≥56 years | 52 (3.6) | 61 (4.2) | 0.82 (0.56 -1.20) | .312 |
| Transfusion | 114 (3.6) | 192 (6.1) |
|
|
| Age 18-55 years | 59 (3.5) | 107 (6.3) |
|
|
| Age ≥56 years | 55 (3.8) | 85 (5.9) |
|
|
| 1-Year Follow-up | ||||
| PJI | 20 (0.6) | 40 (1.3) |
|
|
| Age 18-55 years | 9 (0.5) | 25 (1.5) |
|
|
| Age ≥56 years | 11 (0.8) | 15 (1.0) | 0.69 (0.31-1.51) | .364 |
| Periprosthetic fracture | 19 (0.6) | 22 (0.7) | 0.82 (0.44-1.53) | .544 |
| Age 18-55 years | 7 (0.4) | 6 (0.4) | 1.06 (0.35-3.31) | .926 |
| Age ≥56 years | 12 (0.8) | 16 (1.1) | 0.72 (0.33-1.53) | .409 |
| Dislocation | 83 (2.6) | 70 (2.2) | 1.13 (0.82-1.57) | .470 |
| Age 18-55 years | 48 (2.8) | 47 (2.7) | 1.02 (0.62-1.42) | .932 |
| Age ≥56 years | 35 (2.4) | 23 (1.6) | 1.50 (0.89-2.59) | .137 |
| Mechanical complication | 73 (2.3) | 60 (1.9) | 1.21 (0.85-1.71) | .289 |
| Age 18-55 years | 42 (2.5) | 34 (2.0) | 1.18 (0.75-3.04) | .656 |
| Age ≥56 years | 31 (2.1) | 26 (1.8) | 1.20 (0.71-2.05) | .511 |
| Aseptic revision THA | 86 (2.7) | 68 (2.2) | 1.30 (0.94-1.80) | .113 |
| Age 18-55 years | 47 (2.7) | 43 (2.5) | 1.05 (0.68-1.61) | .836 |
| Age ≥56 years | 39 (2.7) | 25 (1.7) | 1.55 (0.94-2.61) | .092 |
| 2-Year Follow-up | ||||
| PJI | 37 (1.2) | 46 (1.5) | 0.80 (0.51-1.25) | .334 |
| Age 18-55 years | 21 (1.2) | 29 (1.7) | 0.74 (0.46-1.31) | .262 |
| Age ≥56 years | 16 (1.1) | 17 (1.2) | 0.90 (0.44-1.80) | .782 |
| Periprosthetic fracture | 21 (0.7) | 26 (0.8) | 0.77 (0.42-1.37) | .393 |
| Age 18-55 years | 8 (0.5) | 7 (0.4) | 1.04 (0.37-2.99) | .946 |
| Age ≥56 years | 13 (0.9) | 19 (1.3) | 0.66 (0.32-1.33) | .256 |
| Dislocation | 92 (2.9) | 82 (2.6) | 1.08 (0.80-1.47) | .633 |
| Age 18-55 years | 54 (3.2) | 54 (3.2) | 1.00 (0.64-1.39) | .996 |
| Age ≥56 years | 38 (2.6) | 28 (1.9) | 1.34 (0.82-2.22) | .252 |
| Mechanical complication | 113 (3.6) | 98 (3.1) | 1.16 (0.88-1.53) | .297 |
| Age 18-55 years | 72 (4.2) | 58 (3.4) | 1.22 (0.85-1.74) | .280 |
| Age ≥56 years | 41 (2.8) | 40 (2.8) | 1.04 (0.67-1.63) | .872 |
| Aseptic revision THA | 117 (3.7) | 97 (3.1) | 1.27 (0.96-1.68) | .094 |
| Age 18-55 years | 68 (4.0) | 57 (3.3) | 1.18 (0.82-1.71) | .384 |
| Age ≥56 years | 49 (3.4) | 40 (2.8) | 1.23 (0.81-1.90) | .347 |
a Data are reported as n (%) unless otherwise indicated. Boldface ORs and P values indicate statistically significant results (P < .05). AKI, acute kidney injury; DVT, deep vein thrombosis; HA, hip arthroplasty; OR, odds ratio; PE, pulmonary embolism; PJI, prosthetic joint infection; THA, total hip arthroplasty; UTI, urinary tract infection.
b Reference group = prior HA.
c Patient count reported as “-1” by PearlDiver since the true size is <11. In such instances, if the cohort size was unable to be inferred, a patient count of 5 (median between 1 and 10) was assigned. However, the PearlDiver software uses the real patient counts during statistical analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.