
Abstract
Background:
Failure of hip arthroscopy procedures and the need for subsequent total hip arthroplasty (THA) have been estimated to be as high as 16%. Prior literature has shown that failed ipsilateral knee arthroscopy may have a negative impact on the functional outcome of subsequent total knee arthroplasty. To date, there is limited information regarding the impact of failed hip arthroscopy on the clinical outcomes of subsequent primary THA.
Purpose:
To compare clinical outcomes in primary THA between patients with and without prior arthroscopic hip surgery.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing primary THA with a history of ipsilateral hip arthroscopy were matched and compared in a 1:2 manner with patients undergoing primary THA without a history of hip arthroscopy. Patient-reported clinical outcomes were measured with the modified Harris Hip Score, the University of California–Los Angeles Activity Score, and 3 subscales from the Western Ontario and McMaster Universities Osteoarthritis Index (Pain, Stiffness, and Physical Function).
Results:
At a mean follow-up of 42 months, there was no significant difference in any of the outcome measures between the 58 study hips and 116 matched controls. Additionally, both groups exhibited an absolute change in outcome scores that exceeded the minimum clinically important difference.
Conclusion:
Prior ipsilateral arthroscopic hip surgery does not adversely affect the clinical outcome of subsequent THA.
Hip osteoarthritis is a debilitating disease affecting up to 27 million people in the United States. 14 Although the condition mainly affects the elderly, certain hip abnormalities—such as femoroacetabular impingement and development dysplasia of the hip—predispose to the development of osteoarthritis much earlier in life, potentially leading to disability for adolescents and young adults. 5,8,9 Hip arthroscopy has become a well-accepted practice for the diagnosis and treatment of certain prearthritic and early arthritic hip problems. 3 It has proven to be an effective, reproducible, and minimally invasive method for addressing nonstructural problems, such as traumatic acetabular labral tears and intrinsic tissue defects, as well as structural pathology, predominantly femoroacetabular impingement. 6,7,15,16 The clinical outcomes of hip arthroscopy procedures have significantly improved with the development of specialized instruments and surgical techniques. Hip arthroscopy has generally demonstrated similar efficacy when compared with open procedures, with sustained clinical improvement for most patients up to 10 years. 1,4,18
Despite these promising results, the role of arthroscopy for treatment of moderate to advanced intra-articular hip disease remains limited. 13,22 Hip osteoarthritis can progress and eventually require total hip arthroplasty (THA) for end-stage disease in spite of arthroscopic intervention. Many factors, such as existing degenerative change in the joint space or residual structural deformity, predispose to failure of arthroscopy. 2,19 Studies estimate the incidence of THA for osteoarthritis following arthroscopy to be approximately 16% after a mean 7-year follow-up, with the interval to THA inversely correlated with severity of osteoarthritis at the time of arthroscopy. 11
Despite the increasing number of patients undergoing THA following prior hip arthroscopy, there remains a paucity of literature on the effect of prior arthroscopic surgery of the hip joint on THA surgical complications and postoperative outcomes. Nam et al 17 examined a group of 43 patients who underwent metal-on-metal hip resurfacing arthroplasty following ipsilateral hip arthroscopy and compared them with a matched-control hip resurfacing arthroplasty cohort. The authors found no difference in range of motion, Harris Hip Score, University of California–Los Angeles (UCLA) Activity Score, Short Form–12 Health Survey (SF-12) score, or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score at the 1-year postoperative visit. Studies evaluating the impact of prior arthroscopic surgery on subsequent ipsilateral arthroplasty of the knee have shown mixed results. Issa et al 12 found no clinical or functional outcomes difference between 2 cohorts of patients undergoing total knee arthroplasty (TKA), 1 of which had prior ipsilateral knee arthroscopy. In contrast, studies by Werner et al 23 and Piedade et al 20 showed significantly higher rates of postoperative complications among patients undergoing TKA following prior ipsilateral knee arthroscopy when compared with control groups undergoing TKA without prior arthroscopic surgery. Haughom et al 10 recently found no significant difference in THA functional outcomes, as measured by the modified Harris Hip Score (mHHS), in a comparison of 42 patients with prior hip arthroscopy and controls (no arthroscopy).
The objective of the current study was to compare the clinical outcomes of primary THA between patients with (study group) and without (comparison group) previous arthroscopic hip surgery. Our hypothesis was that there will be no significant difference in clinical outcomes between the study and comparison cohorts.
Methods
A single-center case-control study was designed and approved by an institutional review board. A query was submitted through our prospective hip arthroplasty database, which includes 3640 patients and 4318 hips treated from December 1, 2000, through September 30, 2013. All patients within the database had been treated by 2 joint reconstruction surgeons at our institution (R.M.N., J.C.C.). We identified all patients who underwent primary THA following a single ipsilateral hip arthroscopy and who had at least 1 year of clinical follow-up for the THA. Patients were excluded for (1) a history of ipsilateral hip surgery besides hip arthroscopy prior to the primary THA, (2) previous ipsilateral hip fracture or traumatic injury, and (3) hip disease secondary to infection or rheumatologic disorders.
The arthroplasty database search identified 433 patients (477 hips) who had undergone any ipsilateral hip procedure prior to primary THA. Within this cohort, 74 patients (75 hips) had previous ipsilateral hip arthroscopy and were considered for study participation. Two patients were excluded for a diagnosis of inflammatory arthritis. One individual had undergone hip arthroscopy followed by THA in his hips bilaterally; in his case, only the first THA was included. Of the 72 patients (72 hips) who met the surgical inclusion parameters, 58 (80.6%) had a minimum 1-year follow-up with pre- and postoperative functional assessments completed. The study group of 58 patients was composed of 39 women (67%) and 19 men, with a mean age of 45 years (range, 19-65 years) at time of hip arthroscopy. No patients withdrew from the study.
Patients (hips) in the study group were matched 1:2 with patients in the primary THA group from the same hip arthroplasty database and surgical period based on the following criteria: age at time of THA (±3 years), body mass index (BMI; ±3 points), race, sex, and surgeon performing THA. The comparison group was limited to patients who had no history of ipsilateral hip procedures prior to the primary THA and who had completed at least 1 year of clinical follow-up. The researchers performing the matching (A.X., T.A.) were blinded to all outcome data of the study and control populations. The medical records of patients with previous arthroscopy were reviewed, when available, to identify details of the procedure, including surgical indication, treating surgeon, location, and date of surgery. There were 116 patients in the comparison (control) group.
The mean age at the time of primary THA was 48 years (range, 20-71 years) and 49 years (range, 19-73 years) for the study and control groups, respectively. The mean BMI at the time of surgery was 28.0 kg/m2 (range, 18.8-40.8 kg/m2) for the study group and 28.6 kg/m2 (range, 16.0-42.5 kg/m2) for the comparison cohort. There were no statistically significant differences in age, BMI, or follow-up durations between the study and control groups (Table 1).
Patient Characteristics a

a Data are presented as n (%) or mean ± SD (range).
The most common indications for hip arthroscopy included labral tear (22 patients, 37.9%) and femoroacetabular impingement with an associated labral tear (11 patients, 19%) (Table 2). Forty-three of the hip arthroscopy procedures done at our institution were performed by 1 of the 2 senior authors (R.M.N. or J.C.C.), and 17 arthroscopies were performed at outside hospitals. The mean time between arthroscopic hip surgery and primary THA was 28 months (range, 1-102 months). All subsequent primary THA surgery was performed by 1 of 3 arthroplasty surgeons in our group.
Indications for Hip Arthroscopy a

a FAI, femoroacetabular impingement.
All patients were assessed with a panel of self-reported clinical outcome measures, including the mHHS, UCLA Activity Score, and the WOMAC subscales for Pain, Stiffness, and Physical Function. The patient scores for these measures were initially obtained during the preoperative clinic visits prior to the THA. The outcome measures were repeated at the postoperative visit, with patients independently completing the questionnaires at their 1-year follow-up visit. All complications, as well as need for revision surgery, were obtained from review of the electronic medical records. The completion rates of preoperative functional questionnaires ranged between 84% and 98% in the study group and 86% and 98% in the control group. The study group had a mean follow-up duration of 3.2 years following primary THA (range, 1-10 years) and the comparison group, 3.5 years (range, 1-12 years). The mean ± SD interval between surgery and clinical appointments with questionnaire follow-up was 39 ± 27.5 months and 42 ± 34.7 months for the study and control groups, respectively.
Descriptive statistics were utilized to compare the demographic characteristics of both groups, as well as clinical hip scores and follow-up duration. Statistical analysis included the Student t test for continuous variables and the Fisher exact test for categorical variables. All probability values were 2-tailed, with P < .05 regarded as statistically significant.
Results
The baseline patient-reported outcomes showed that prior to primary THA, there was no significant difference between the study and control groups in the mHHS, the WOMAC-Pain, -Stiffness, and –Physical Function scores, or the UCLA Activity Score (Table 3). At final clinical follow-up after primary THA, there was no significant difference in any of the outcome scores between the groups (Table 4). Additionally, when the absolute change (delta) in pre- to postoperative outcome scores was examined, the study and control groups demonstrated no statistically significant differences (Table 5). In both groups, the absolute change in outcome scores exceeded the minimum clinically important difference, and the difference in the delta between the study and control groups was less than the minimum clinically important difference for each outcome score measured. The mean operative time for patients undergoing THA with prior hip arthroscopy was 90.3 ± 21.5 minutes, as compared with 88.2 ± 31.7 minutes for patients without prior hip arthroscopy (P = .647).
Preoperative Outcomes Scores a
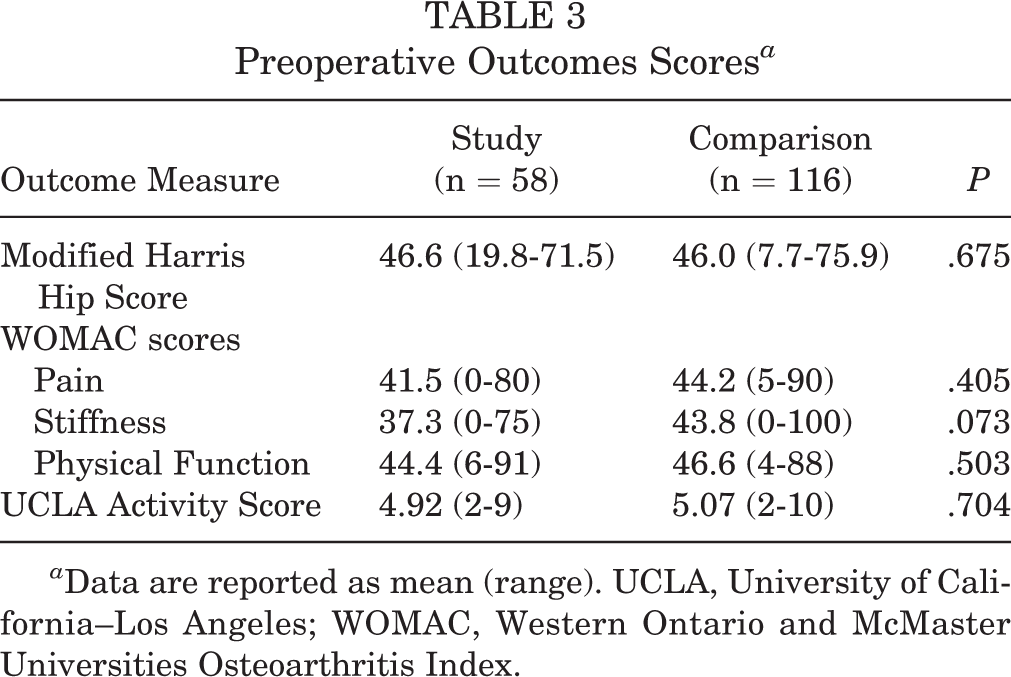
a Data are reported as mean (range). UCLA, University of California–Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Postoperative Outcomes Scores a

a Data are reported as mean (range). UCLA, University of California–Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Absolute Change in Outcomes Scores a

a MCID, minimum clinically important difference; UCLA, University of California–Los Angeles; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Few complications occurred in either patient group. The study group had 4 complications (6.9%). Two patients developed deep vein thrombosis in the acute postoperative period. Neither patient required hospital readmission, and both were treated with medical therapy and recovered fully without incident of pulmonary embolus or other associated morbidity. Two patients experienced dislocation of the THA (8 and 39 days postoperatively). Both cases were managed with closed reduction and abduction bracing, and neither patient had experienced recurrent dislocation at the most recent follow-up. There was 1 postoperative complication in the comparison group (0.9%), in which a patient developed a deep infection of the THA requiring explant with antibiotic spacer placement, a course of intravenous antibiotics, and staged replantation of all components. Postoperative complications were analyzed with the Clavien-Dindo classification, which was shown to be adaptable to orthopaedic patients undergoing hip surgery. 21 In the study group, 2 complications were classified as grade 2, as they deviated from the standard postoperative course but were managed with outpatient pharmacologic or nonoperative treatment, while the 2 dislocations were grade 3, requiring sedation and procedural treatment. 21 The lone complication in the comparison group was also grade 3.
Discussion
In recent years, there has been increasing interest in the diagnosis and treatment of hip disease among adolescents and young adults. Consequently, arthroscopic hip surgery has gained traction as an effective, reproducible, and less invasive method of diagnosing and treating prearthritic and early arthritic hip problems. Hip arthroscopy is employed in dealing with nonstructural problems associated with disorders of the hip joint and hip region, as well as structural problems such as femoroacetabular impingement. Advancement in instrumentation and techniques has improved the efficacy of hip arthroscopy, with most patients experiencing clinical improvement following arthroscopic surgery. 1,4,18
Despite the increasing success of hip arthroscopy, >15% of patients who undergo arthroscopic hip surgery will undergo subsequent THA. 19 Results from prior studies evaluating TKA in the setting of prior arthroscopic surgery are conflicting, with some showing increased rates of venous thrombosis, infection, and stiffness if TKA is performed within 6 months of knee arthroscopy and others finding no difference in outcomes. 20,23 Additionally, a prior case-control study utilizing a single patient-reported outcome measure showed no functional difference at short-term follow-up among patients undergoing THA after ipsilateral hip arthroscopy. 10 Our study aimed to determine the effects of prior ipsilateral hip arthroscopy on the clinical outcomes of primary THA. An understanding of the symptoms, function, and postoperative complications of patients undergoing primary THA after previous hip arthroscopy, as compared with those without prior arthroscopy, will provide data for clinical decision making and improved management of surgeon/patient expectations. Our findings are based on data obtained from a larger cohort of patients with a longer mean follow-up, as compared with prior studies.
Our findings indicated no significant differences in the postoperative outcome scores between the study and control populations. Additionally, there were no significant differences in the absolute change in outcome scores between the study and control cohorts across all reported outcome measures. Finally, based on the standard deviation and sample size, this study has an observed power of 92.1% to detect a clinically significant difference of 15 minutes of operative time between the study and control groups, and no significant difference was noted. While the body of current literature is incomplete, some proposed concerns about arthroscopic hip surgery prior to THA include complications in the exposure as a result of scar tissue, increased infection risk owing to prior surgery, and the potential of encountering hardware that may make THA more difficult. However, our results show that at early to midterm follow-up, prior arthroscopic hip surgery did not negatively affect the clinical outcome of patients undergoing subsequent ipsilateral THA and that patients undergoing THA after prior ipsilateral hip arthroscopy can expect to experience the same degree of improvement in function as those without prior arthroscopy.
There are limitations to this study inherent to its retrospective design. Selection bias may have been introduced during the matching of the study and control populations, despite the blinding of researchers to the clinical outcome scores. The study also lacked completion of all outcome measures by all patients at the pre- and postoperative visits. However, with a mean 91% completion rate of all pre- and postoperative forms, the effect of this limitation is minimized. This study was not powered to evaluate the impact of the various prearthroscopy diagnoses (femoroacetabular impingement, labral tear, etc) on the outcome of THA. The database evaluated in this study spans 14 years, during which the technology and understanding of hip arthroscopy procedures have evolved. As seen with any new procedure, the clinical decision to pursue hip arthroscopy and the surgical techniques involved vary over time. Clinical outcomes also improve with the operative experience of the surgeon. In the case of hip arthroscopy, continued data collection and future research will mitigate this learning curve effect.
Conclusion
The findings of this study, consisting of early to midterm follow-up with multiple patient-reported outcome measures, illustrate that prior ipsilateral arthroscopic hip surgery does not adversely affect the clinical outcomes of primary THA. These findings provide important information that may aid surgeons in the decision-making process when evaluating a patient for hip arthroscopy; they might also allow for a more informed discussion with patients regarding the impact of hip arthroscopy on a possible future THA and the expected clinical outcomes of THA after failed arthroscopic treatment.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Curing Hip Disease Fund. J.A.H. has received educational support from Smith & Nephew. J.J.N. is a consultant for Ceterix Orthopaedics, Smith & Nephew, and Zimmer; is a paid speaker/presenter for the Pediatric Research in Sports Medicine Society and Zimmer; receives research support from Zimmer and Smith & Nephew; and has received educational support from Elite Orthopedics. R.M.N. has received research support from Biomet, DePuy, Medical Compression Systems, Smith & Nephew, and Stryker; consulting fees from Biocomposites, Blue Belt Technologies, Cardinal Health, DePuy, Ethicon, Halyard Health, Medical Compression Systems, Medtronic, Microport, Mirus, Smith & Nephew, and St Jude Medical; educational support from Arthrex and Elite Orthopedics; nonconsulting fees from Zimmer Biomet; royalties from Microport; and hospitality payments from Pacira Pharmaceuticals. J.C.C. receives research support from Smith & Nephew and Zimmer, is a consultant for Microport Orthopedics, and receives royalties from Wolters Kluwer Health–Lippincott Williams & Wilkins. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Washington University School of Medicine Human Research Protection Office.