
Abstract
Background:
There is a paucity of literature on the effects of labral tear size on long-term patient-reported outcomes (PROs) and conversion to total hip arthroplasty (THA) after hip arthroscopy.
Purpose:
To understand the differences in hip arthroscopy survivorship and outcomes between patients with large labral tears (LLTs) and small labral tears (SLTs).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study included patients who underwent primary hip arthroscopy for symptomatic labral tears secondary to femoroacetabular impingement by a single surgeon from 2001 to 2013; they completed surveys for such PRO measures (PROMs) as the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Specific, 33-item International Hip Outcome Tool (iHOT-33), and pain relief. Patients ≤18 years of age, hip dysplasia LCEA <20°, and Tönnis grade ≥2 were excluded. Included patients were stratified into 2 cohorts: SLT (≤60°) and LLT (>60°).
Results:
In this study of 154 patients (48.7% female; mean ± SD age, 38 ± 10.8), there was a mean ± SD follow-up of 11.0 ± 2.4 years and body mass index of 26.1 ± 4.3 kg/m2. Women experienced a higher frequency of SLT than men (59.8% vs 40.2%; P = .003). Student t tests demonstrated that the SLT cohort experienced significantly better outcomes than the LLT cohort for mHHS, HOS-ADL, and iHOT-33. Multivariate linear regression analyses adjusting for demographic, radiographic, and intraoperative findings indicated that LLT size can predict worse long-term outcomes after hip arthroscopy for mHHS and HOS-ADL (P < .05). Kaplan-Meier estimates and weighted Cox regression demonstrated that the conversion rate to THA for LLT was significantly greater than that for SLT (hazard ratio, 7.92; 95% CI, 2.96-21.2; P < .0001).
Conclusion:
Those in the LLT cohort experienced a significantly greater conversion rate to THA than did the SLT cohort. Also, SLT size can independently predict better long-term outcomes on certain PROMs after primary hip arthroscopy.
A previous study published by Chahla et al 3 in the American Journal of Sports Medicine found that when comparing a cohort with “large labral tear” (LLT) size against a cohort with “small labral tear” (SLT) size, patients with SLTs experienced better 2-year patient-reported outcomes (PROs) after their index surgery.
This novel study presents a comparison of an LLT size and SLT size cohort, investigating differences in long-term PROs as well as THA-free survivorship, helping the field better understand how to preserve the hip joint. The acetabular labrum, cartilage lining the rim of the acetabulum, is an important anatomical component of the hip socket. The suction seal created by the acetabular labrum maintains the intra-articular synovial fluid and relative negative pressure necessary for the joint to withstand the significant forces associated with mobility. 22
Acetabular labral tears can result from an array of causes including repetitive movements, traumatic injury, and femoroacetabular impingement (FAI). 2 Though labral tears can be asymptomatic, symptomatic labral tears can cause debilitating hip pain and interfere with daily activities. The treatment plan for acetabular labral tears consists of conservative management followed by surgery to repair the torn labrum. 16 If left untreated, however, labral tears can accelerate the progression of degenerative change within the hip joint, leading to arthritis. 15
Past studies have only elucidated risk factors that may indicate the magnitude of a labral tear size and the effects of labral tear size on midterm PROs after hip arthroscopy. Patients who were older, male, and had an increased alpha angle were found to be at greater risk of a larger labral tear. 19 Furthermore, Chahla et al 3 analyzed 2-year PROs after hip arthroscopy for FAI, comparing a cohort with an LLT size of ≥2.5 cm against a cohort with an SLT size of <2.5 cm, and found that patients with SLTs experienced better PROs after their index surgery.
However, there is a paucity of literature on the effects of labral tear size on long-term outcomes and conversion to total hip arthroplasty (THA) after primary hip arthroscopy for repairing symptomatic acetabular labral tears. Therefore, this study's purpose was to investigate the association between labral tear size and (1) patient demographic characteristics, radiographic findings, and intraoperative variables; (2) long-term functional outcomes after primary hip arthroscopy for symptomatic labral tears secondary to FAI; and (3) the rate of conversion to THA.
We hypothesized that those with LLT would have poorer long-term outcomes than those with SLT and that SLTs portend significantly greater THA-free survivorship after hip arthroscopy secondary to FAI.
Methods
Patient Selection and Study Design
The study protocol was approved by an institutional review board with each patient providing consent.
This retrospective cohort study included patients who, after failing conservative treatment, underwent primary hip arthroscopy for symptomatic labral tears secondary to FAI by a single senior surgeon (S.D.M.). Patients were included if they underwent surgery between 2001 and 2013, optimizing the number of patients included in the study with ≥8-year follow up. Excluded patients did not provide consent, were ≤18 years of age, had Tönnis grade ≥2, hip dysplasia (lateral center-edge angle [LCEA] <20°), incomplete follow-up data, history of ipsilateral hip surgery or revision surgery before their senior surgeon completed primary hip arthroscopy for symptomatic labrum, or did not have a labral tear (Figure 1). Labral tear size can be measured through an array of methods including length in centimeters and clock times on a clockface, but degrees on a circle were used in this study for ease of visualization and analysis.6,8 Included patients were most evenly stratified into 2 cohorts: SLT (≤60°) and LLT (>60).
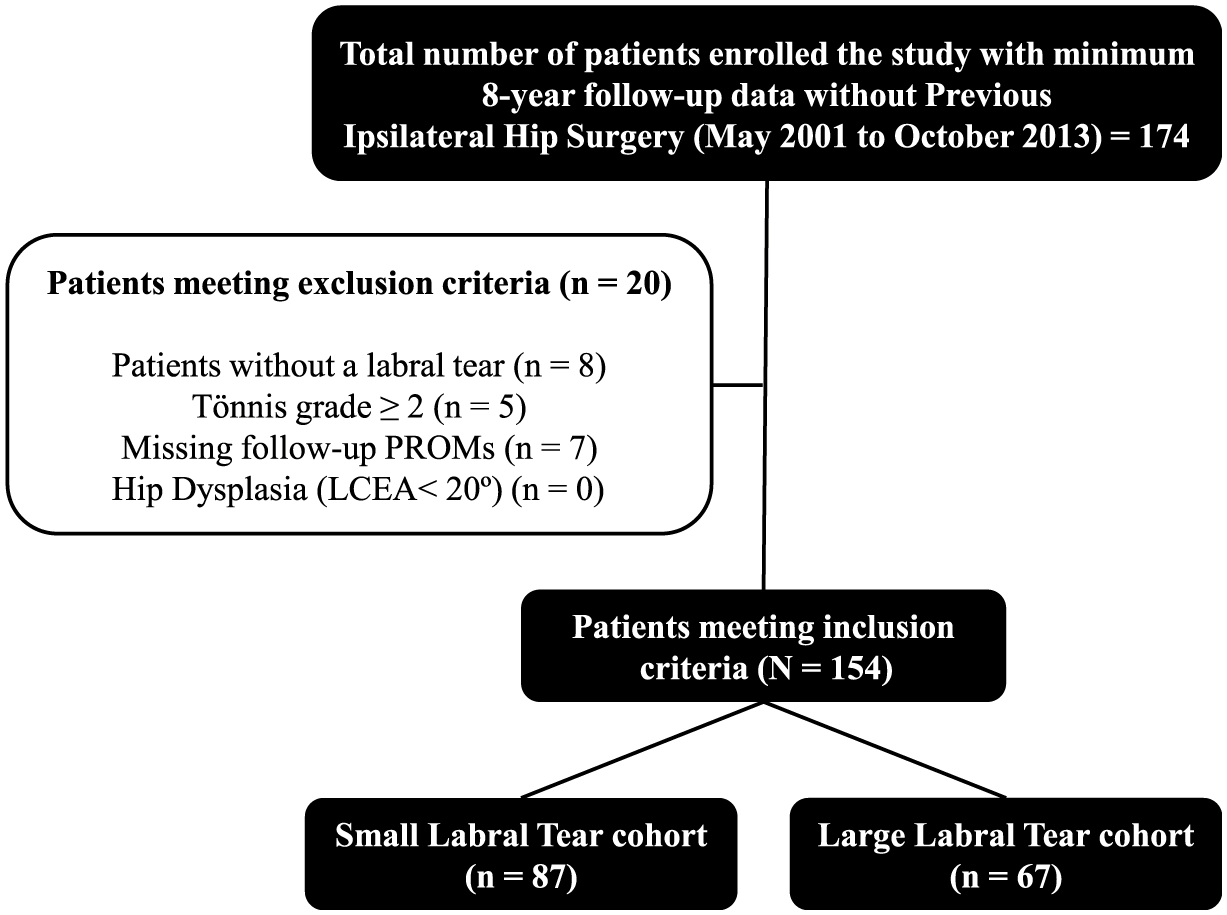
CONSORT (Consolidated Standards of Reporting Trials) diagram. LCEA, lateral center-edge angle; PROM, patient-reported outcome measure.
Postoperative PRO Measure Collection
Patients were retrospectively surveyed about their postoperative outcomes, resulting in variable follow-up times. For the patients that did not convert to THA, 4 PRO measures (PROMs) were evaluated: the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL); Hip Outcome Score–Sports Specific (HOS-SS), and 33-item International Hip Outcome Tool (iHOT-33). Pain was evaluated by the visual analog scale (VAS). Because of the retrospective nature of this study, the clinical relevancy of outcomes was measured via the Patient Acceptable Symptom State (PASS). Patient satisfaction was also evaluated in the distributed patient survey. The data for other variables such as conversion to THA were collected manually through chart review of each enrolled patient's electronic medical record.
Abbreviated Surgical Technique
Each patient in the study was operated on by a single attending surgeon (S.D.M.).1,4,13,17,21,23 In summary, patients were oriented in a supine position on a hip distraction table (Smith & Nephew) with a gel-padded perineal post. The puncture capsulotomy technique was utilized in the establishment of the 4 portal sites: anterolateral, anterior, midanterior, and Dienst. Based on individual patient anatomy, portal sites occasionally required extension. Necessity of capsular closure was determined based on the final portal size. The use of electrocautery was limited to prevent elevated intra-articular cartilage temperatures. Traction times were minimized to prevent neurovascular injuries as well. The surgeon opted for labral debridement if the labral tear was hypoplastic, degenerative, or involving <50% of the labral width; labral repair was selected if there existed adequate, healthy labral tissue for suture fixation or if the tear was complex with extension into the chondrolabral junction. Cam lesions and pincer lesions were concomitantly addressed via femoroplasty and acetabuloplasty, respectively. Dynamic examination and visualization from the peripheral compartment after traction was released allowed the senior surgeon to evaluate the integrity of the labrum, the suction seal, and potential for residual impingement. Patients did not receive prophylactic treatment for heterotopic ossification.
Postoperative Rehabilitation
All patients followed the senior surgeon's 5-phase patient-guided postoperative rehabilitation protocol. In order to prevent deep vein thrombosis, patients were prescribed 81 mg aspirin daily for 3 weeks after surgery. Until 6 weeks after surgery, patients were told weightbear as tolerated with crutches and maintain a foot flat, stiff-legged gait on the operative leg. Additionally, patients were told to keep a level pelvis, as limping could result in additional stresses on the labral repair site. Once 6 weeks had passed, the patient could slowly wean off crutches and begin using a stationary bike at low resistance with the seat high to reintroduce motion but avoid stress caused by strengthening. At 10 weeks, patients were allowed to begin using an elliptical trainer as tolerated, increasing exercise time while being cognizant of any pain or discomfort in the hip. Light swimming without flutter kicking and with the use of a buoy board, as necessary, was also permitted. Light twisting activities, including golf, and strengthening exercises such as short arc leg presses and hamstring curls at high repetition and low weight were permitted at 4 months. After 6 months postoperatively, patients were allowed to resume full impact-loading activities.
Demographic, Radiographic, and Intraoperative Data Collection
The relevant demographic and radiographic variables for which data were collected prior to surgery were age in years, body mass index (BMI), sex, race, Area Deprivation Index (ADI), LCEA, Tönnis angle, alpha angle, joint space (lateral, central, and medial), crossover sign, posterior wall sign, ischial spine sign, and type of FAI (none, cam, pincer, or both). Relevant intraoperative variables were traction time, Tönnis grade, chondral treatment, labral treatment (debridement vs repair), Beck classification of labral damage and transition zone (chondrolabral junction) cartilage, Outerbridge classification of articular cartilage, presence of a chondral flap, and type of FAI treatment (none, acetabuloplasty, femoroplasty, femoroacetabular osteoplasty). Notably, labral tear size was quantified intraoperatively. Radiographic variables were measured by trained clinical researchers.
Statistical Analysis
Statistical analysis was completed on a consecutive cohort of patients. A power analysis was conducted based on the available sample size. LLTs comprise approximately 45% of the senior author's (S.D.M.) practice. Relative hazards for conversion to THA between 1.6 and 2 were considered clinically meaningful. Assuming 45% prevalence of LLT, a sample size of 144 would provide 80% power to detect a relative hazard of 1.6 at an alpha level of .05. Alternatively, a sample size of 66 would provide 80% power to detect a relative hazard of 2 at an alpha level of .05. Descriptive statistics including means and standard deviation for continuous variables and frequency and proportion for categorical variables were calculated to characterize the study groups. Student t tests were used to obtain unadjusted comparisons between outcomes and continuous variables between cohorts. Categorical variables were compared using chi-square tests and Fisher exact tests based on the frequency of patients in each relevant category. Multiple variable linear regression was used to determine and adjust for relevant demographic, radiographic, and intraoperative covariates when comparing PROMs across cohorts. Unadjusted Kaplan-Meier survival and risk tables were created to visualize and calculate the difference in the rate of conversion to THA between the LLT and SLT cohorts (unadjusted hazard ratio [HR]). A multivariate model was fit to obtain HRs for tear size adjusted for known predictors conversion to THA. This included Tönnis grade, sex, and age. Given the event rate of 29 conversions to THA, a penalized Cox regression model (Firth penalized likelihood) was used. The results of the model are presented as HRs with corresponding 95% CIs. A P value <.05 was established as the threshold for statistical significance. All statistical analyses were completed using R Version 4.4.1 (R Foundation for Statistical Computing).
Results
Patient Demographics
In this study of 154 patients (48.7% female; mean ± SD age, 38 ± 10.8 years), there was a mean ± SD follow-up of 11.0 ± 2.4 years and BMI of 26.1 ± 4.3 kg/m2 (Table 1). Most patients in this study were White (96.4%).
Patient Demographics a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). ADI, Area Deprivation Index; BMI, body mass index; LLT, large labral tear; SLT, small labral tear.
Indicates whether there is a significant difference between the number of females in SLT vs LLT and same for males.
In the LLT cohort, patients were older (mean ± SD, 40.6 ± 11.6 years vs 35.4 ± 10.0 years; P = .003). Women experienced a higher frequency of SLT than men (59.8% vs 40.2%; P = .003). There were no significant differences between the SLT and LLT cohorts, respectively, in regard to length of follow-up (11.1 ± 2.5 years vs 10.9 ± 2.2 years; P = .67), BMI (25.5 ± 4.7 kg/m2 vs 26.7 ± 3.8 kg/m2; P = .10), and ADI (17.9 ± 14.5 vs 18.2 ± 14.4; P = .88) (Table 1).
Radiographic Parameters
Comparing radiographic findings, the LLT cohort had significantly greater alpha angles on average (mean ± SD, 64.8°± 18.7° vs 50.7°± 15.3°; P < .001) and incidence of posterior wall sign (70.1% vs 29.9%; P = .01) than those in the SLT cohort (Table 2). Furthermore, there were significantly more patients with mixed-type FAI lesions in the LLT cohort in comparison with the SLT cohort (22.4% vs 6.9%; P = .001). There were no significant differences between the 2 cohorts for LCEA, Tönnis angle, joint space (medial, central, and lateral), crossover sign, and ischial spine sign (all P≥ .05).
Radiographic Findings a

Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). FAI, femoroacetabular impingement; LCEA, lateral center-edge angle; LLT, large labral tear; SLT, small labral tear.
Adjusted residuals >2 indicating statistical significance.
Procedures Performed and Intraoperative Findings
The mean tear size of the SLT and LLT cohorts, respectively, was 52.8°± 13.1° and 91.8°± 15.8° (P < .001). The traction time (in minutes) during surgery was significantly greater for the LLT cohort versus the SLT cohort (60.5 ± 17.7 minutes vs 57.3 ± 15.2 minutes; P = .04) (Table 3).
Procedures Performed and Intraoperative Findings a
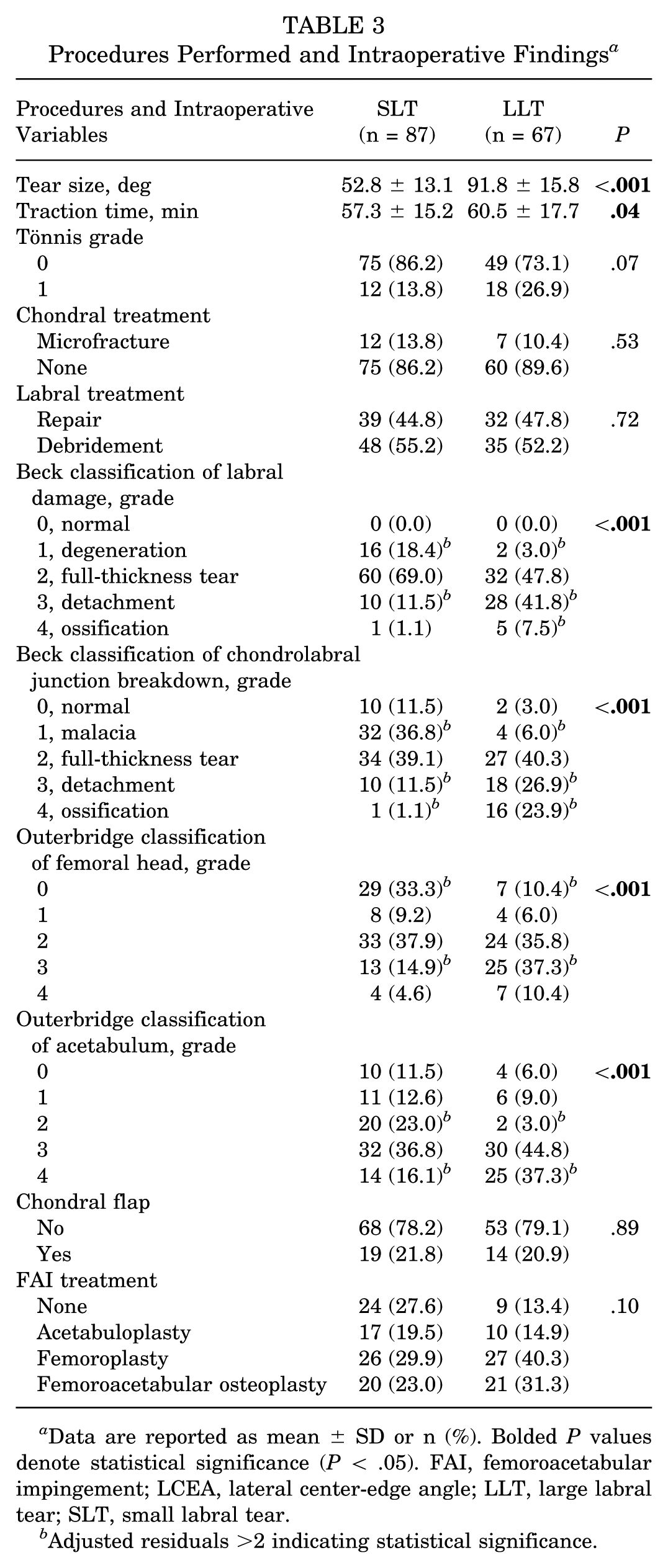
Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). FAI, femoroacetabular impingement; LCEA, lateral center-edge angle; LLT, large labral tear; SLT, small labral tear.
Adjusted residuals >2 indicating statistical significance.
When scoring labral damage by the Beck classification system, there was a significantly greater proportion of patients in the LLT cohort than the SLT cohort with grade 3 (detachment) (41.8% vs 11.5%; P < .001) and grade 4 (ossification) (7.5% vs 1.1%; P < .001). Furthermore, there was a significantly greater frequency of patients in the SLT cohort than the LLT cohort with grade 1 (degeneration) (18.4% vs 3.0%; P < .001). When scoring chondrolabral junction breakdown by the Beck classification system, there was a significantly greater frequency of patients in the LLT cohort than the SLT cohort with grade 3 (detachment) (26.9% vs 11.5%; P < .001). In addition, there was a significantly greater frequency of patients in the SLT cohort than the LLT cohort with grade 1 (malacia) (36.8% vs 6.0%; P < .001).
Grading of the femoral head with the Outerbridge classification system demonstrated the presence of a significantly higher frequency of grade 3 in the LLT cohort in comparison with the SLT cohort (37.3% vs 14.9%; P < .001) and a significantly greater frequency of grade 0 joint cartilage damage in the SLT cohort as opposed to the LLT cohort (33.3% vs 10.4%; P < .001). For the acetabulum, the Outerbridge classification system indicated a significantly higher frequency of grade 2 in the SLT versus the LLT cohort (23.0% vs 3.0%; P < .001) but a significantly lower frequency of grade 4 joint cartilage damage in the SLT cohort versus the LLT cohort (16.1% vs 37.3%; P < .001). There were no significant differences between cohorts for chondral treatment, Tönnis grade, labral treatment, presence of a chondral flap, and FAI treatment.
Cohort-Wise PROMs and PROM PASS Analysis
Bivariate analyses excluding the patients that underwent THA demonstrated that the SLT cohort experienced significantly better outcomes than the LLT cohort for mHHS (88.6 ± 12.4 vs 83.4 ± 14.8; P = .04), HOS-ADL (92.0 ± 10.4 vs 87.2 ± 14.5; P = .03), and iHOT-33 (78.1 ± 21.9 vs 69.4 ± 24.2; P = .047) (Table 4). There was no significant difference in outcomes between the SLT and LLT cohorts for HOS-SS.
Minimum 8-Year PROMs a
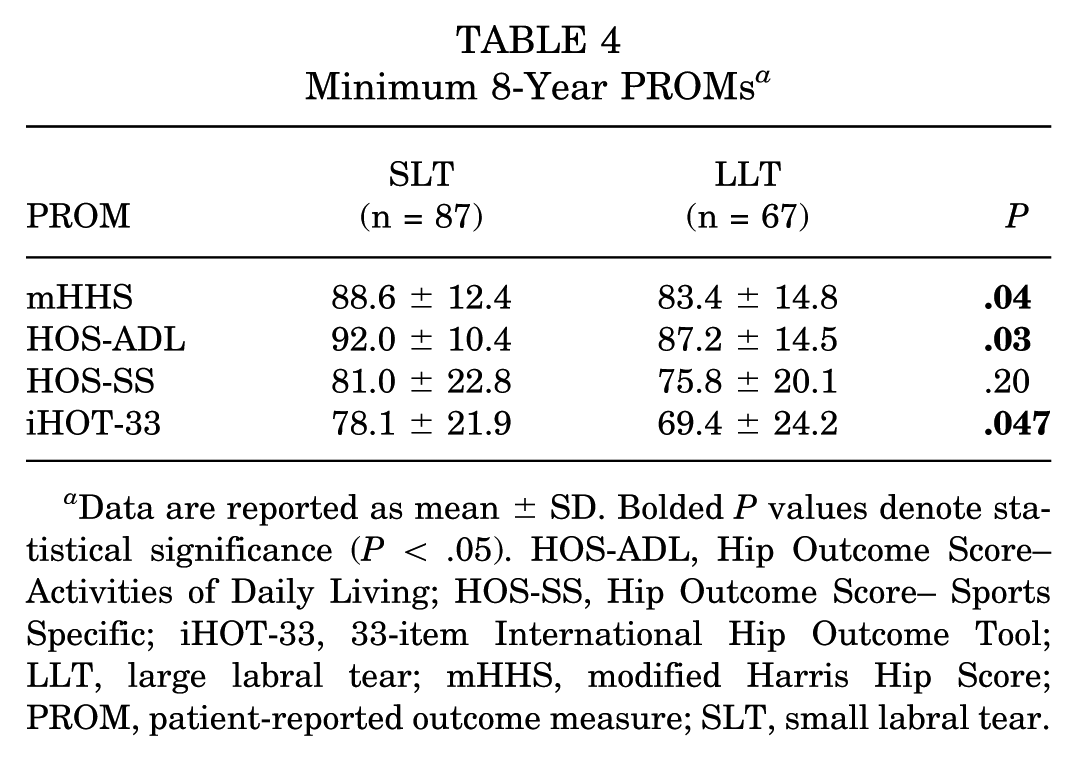
Data are reported as mean ± SD. Bolded P values denote statistical significance (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score– Sports Specific; iHOT-33, 33-item International Hip Outcome Tool; LLT, large labral tear; mHHS, modified Harris Hip Score; PROM, patient-reported outcome measure; SLT, small labral tear.
To elucidate the effect of covariates on the differences in functional outcomes between the SLT and LLT cohorts, a multiple variable linear regression analysis adjusting for labral tear size, age, BMI, sex, Tönnis grade, LCEA, and debridement versus repair was used (Table 5). Labral tear size was a significant independent predictor of functional outcomes for mHHS (β = 5.8; 95% CI, 0.4 to 11.2; P = .03) and HOS-ADL (β = 4.82; 95% CI, 0.4 to 9.2; P = .03). Interestingly, for HOS-ADL, though LCEA was a significant independent predictor, labral tear size was a stronger predictor (β = 4.82 vs 0.33). A Tönnis grade of 1 was a significant independent predictor of worse functional outcomes for both HOS-SS (β = −15.54; 95% CI, −26.5 to −4.6; P = .006) and iHOT-33 (β = −11.61; 95% CI, −23.0 to −0.3; P = .045).
Multiple Variable Linear Regression Analysis of PROMs a
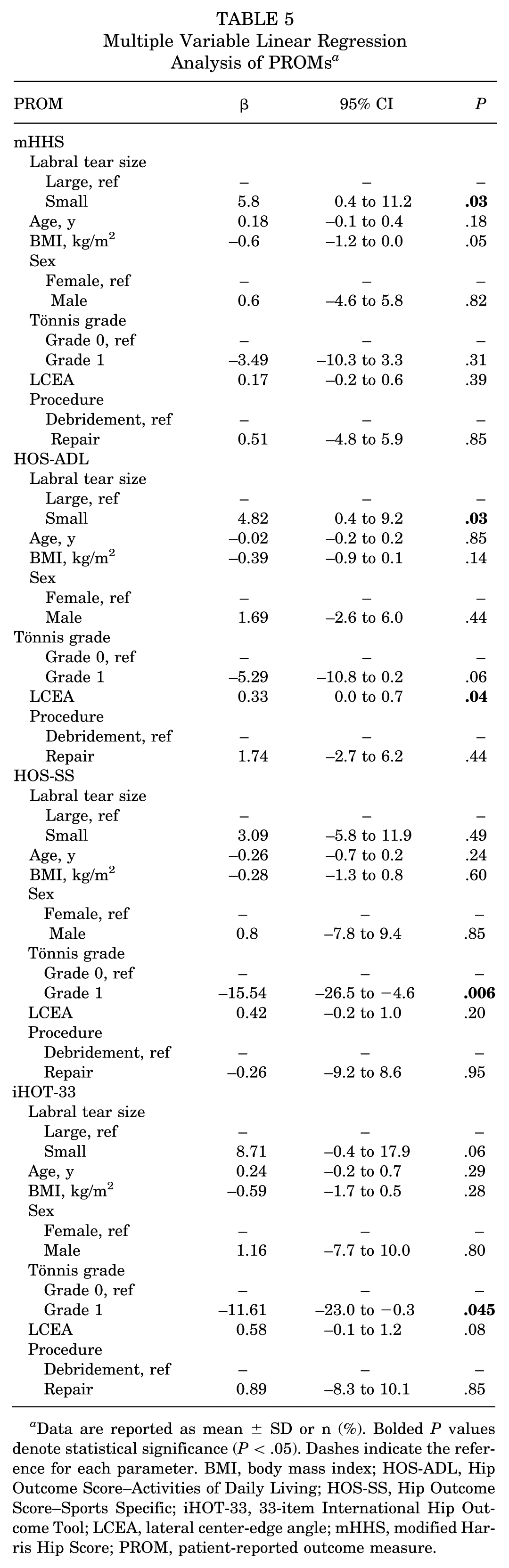
Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). Dashes indicate the reference for each parameter. BMI, body mass index; HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Specific; iHOT-33, 33-item International Hip Outcome Tool; LCEA, lateral center-edge angle; mHHS, modified Harris Hip Score; PROM, patient-reported outcome measure.
There were no significant differences between the PASS rates of either the SLT or the LLT cohort for all PROMs (Table 6).
Minimum 8-Year PROM PASS Rates a

Data are reported as n (%). Bolded P values denote statistical significance (P < .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Specific; iHOT-33, 33-item International Hip Outcome Tool; LLT, large labral tear; mHHS, modified Harris Hip Score; PASS, Patient Acceptable Symptom State; PROM, patient-reported outcome measure; SLT, small labral tear.
The statistics completed on the outcome data did not include data from the patients who converted to THA.
Pain Levels and Satisfaction Analysis
Patients reported similar preoperative and postoperative VAS pain scores across the SLT and LLT cohorts (Table 7). Additionally, patient satisfaction across both the treatment and the regimen was not significantly different between both cohorts. Similarly, there was no significant difference between the frequency of patients who would opt of a repeat hip arthroscopy surgery for repairing symptomatic labral tears.
Pain Levels and Satisfaction Rates a
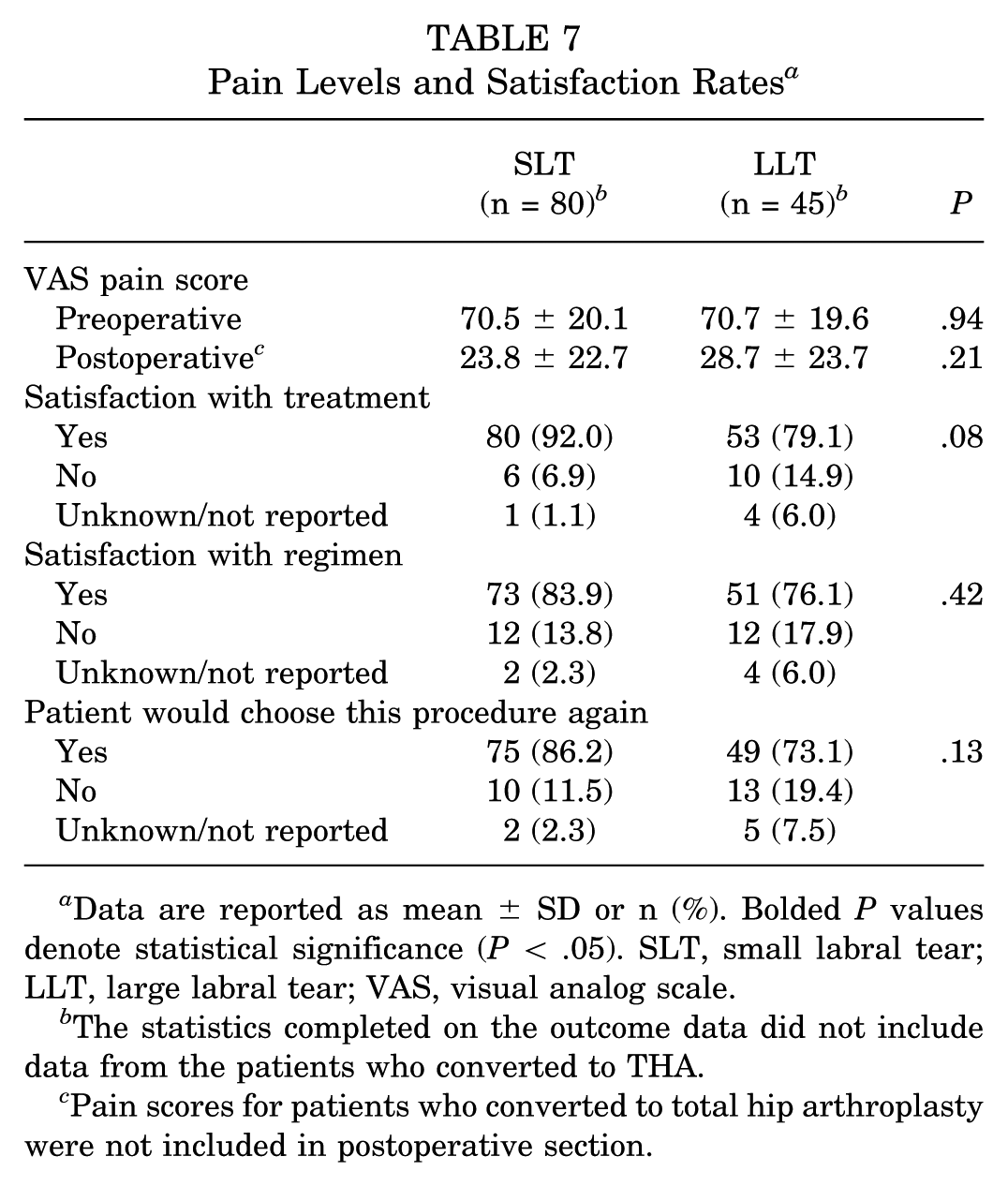
Data are reported as mean ± SD or n (%). Bolded P values denote statistical significance (P < .05). SLT, small labral tear; LLT, large labral tear; VAS, visual analog scale.
The statistics completed on the outcome data did not include data from the patients who converted to THA.
Pain scores for patients who converted to total hip arthroplasty were not included in postoperative section.
Understanding the Conversion to THA
There was a significant difference in the proportion of patients who underwent THA in the duration of the study follow-up period between the SLT and the LLT cohorts, with 32.8% of the LLT cohort and 8.0% of the SLT cohort undergoing THA (P < .001). At 10 years, the survivorship of patients in the SLT cohort was substantially better (97.7%; 95% CI, 94.6%-99.9%) than that of the LLT cohort (67.6%; 95% CI, 57.0%-80.1%).
For those that underwent THA, patients in the LLT cohort underwent THA significantly sooner than those in the SLT cohort (8.4 ± 3.6 years vs 10.9 ± 2.8 years; P < .001).
The unadjusted Kaplan-Meier survival analysis demonstrated that the conversion rate to THA for patients in the LLT cohort was significantly greater than those in the SLT cohort (HR, 7.92; 95% CI, 2.96-21.2; P < .0001) (Figure 2).

Unadjusted (Kaplan-Meier) survival curves and risk table visualizing the rate of conversion to total hip arthroplasty (THA) for the small labral tear (SLT) cohort with tear size ≤60° and large labral tear (LLT) cohort with tear size >60°.
Upon identifying relevant covariates, weighted Cox regression was utilized to calculate the adjusted HRs for conversion to THA. The adjusted HR for LLTs was 5.92 (P < .001), 2.25 (P < .001) per 10-year increase in age, and 2.32 (P = .04) per 1 unit increase in Tönnis grade. Labral tear size, age, and Tönnis grade were all found to be independent predictors of long-term conversion to THA after primary hip arthroscopy for symptomatic labral tears secondary to FAI (Table 8).
Weighted Cox Regression Adjusting for Patient Characteristics for Conversion to THA a
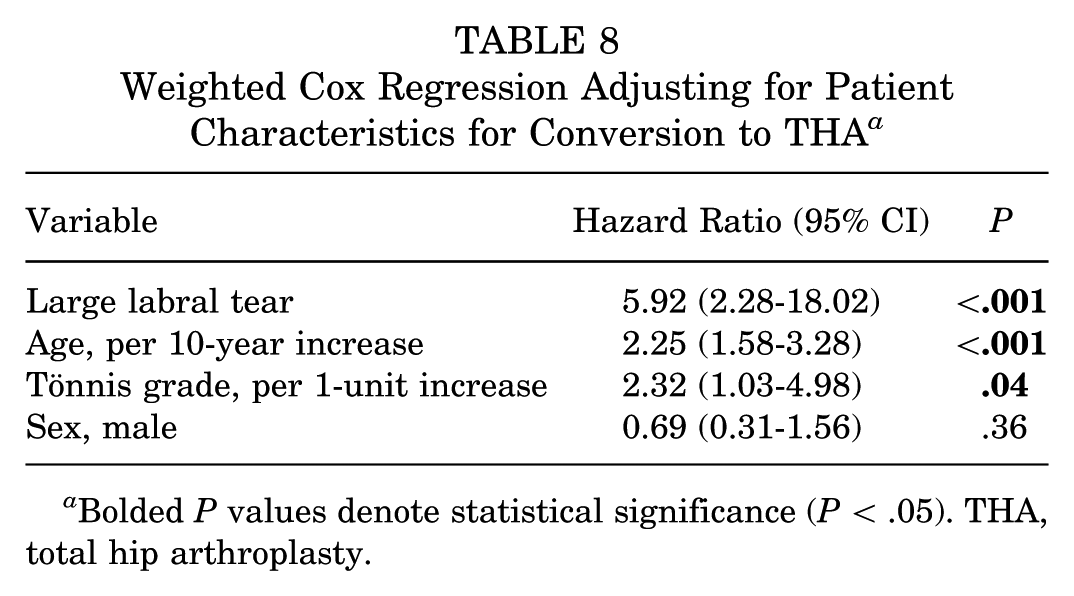
Bolded P values denote statistical significance (P < .05). THA, total hip arthroplasty.
Discussion
Along with finding significant differences in patient demographic characteristics, radiographic findings, intraoperative variables, and ≥8-year outcomes, the present study elucidates a novel understanding that labral tear size correlates significantly with a patient's duration of THA-free survivorship. After adjusting for relevant covariates, labral tear size is a stronger independent predictor of conversion to THA than a 10-year increase in age or a 1-unit increase in Tönnis grade.
Although commonly considered a primary indicator for hip arthroscopic surgery, acetabular labral tear size has not been extensively studied in the context of understanding long-term outcomes after surgery as well as THA-free survivorship, an area this study thoroughly investigated in a large cohort with a ≥8-year follow-up. The present study found that the LLT cohort had a significantly higher age (40.6 ± 11.6 years) than the SLT cohort (35.4 ± 10.0 years), similar findings to a prior study by Redmond et al, 19 which found that age was correlated with labral tear size. Additionally, this study's finding that men had a significantly higher frequency of LLTs than women aligned with a study completed by Lindner et al 11 understanding sex-based differences in symptomatic labral tear presentation; male patients had a significantly larger mean labral tear size when compared with female patients. Given that a predominant cause of acetabular labral tears is FAI, our findings that a higher frequency of those with SLT have no FAI and that a higher frequency of those with LLT have both cam and pincer lesions can be expected. The mean alpha angle for the LLT group is significantly greater than that of the SLT group, surpassing the finding outlined by Lin et al 10 that an alpha angle >57° portends an increased incidence of labral tears and, most relevant to this study, larger tear size. Findings consistently demonstrated that those in the LLT cohort experienced significantly greater frequency of labral damage and chondrolabral junction breakdown via the Beck classification and acetabulum and femoral head by the Outerbridge classification. This contributes to the understanding that labral tears of greater magnitude can lead to a compromised hip suction seal, resulting in more significant pathologies within the joint and increasing the rate of arthritic change.
At ≥8-year follow up, results demonstrated significantly different outcomes between the SLT and LLT cohort for mHHS (88.6 ± 12.4 vs 83.4 ± 14.8; P = .04), HOS-ADL (92.0 ± 10.4 vs 87.2 ± 14.5; P = .03), and iHOT-33 (78.1 ± 21.9 vs 69.4 ± 24.2; P = .047) with the SLT cohort consistently showing better postoperative outcomes. mHHS, HOS-ADL, and iHOT-33 all commonly assess functional outcomes with regard to daily living whereas HOS-SS, which was shown to not have a significant difference between the SLT and LLT cohorts, focuses specifically on a patient's ability to partake in certain athletic activities.9,12,14 HOS-SS has largely been analyzed in studies focused on athletes ranging in ability from recreational to professional athletes, as in a recent study completed by Owens et al. 18 Therefore, when administered to a patient population with some who may not participate in any sports or athletic activities, those patients cannot accurately quantify their athletic ability after surgery as they have no context to respond from, potentially masking differences between cohorts. The PASS rates between cohorts were similar for all evaluated PROMS, indicating that no matter a patient's labral tear size, there remains considerable potential for symptom relief after hip arthroscopy for repairing symptomatic acetabular labral tears. When evaluating labral tear size via magnetic resonance imaging preoperatively, LLTs are not necessarily a contraindication for hip arthroscopic surgery, as this procedure can still bring substantive benefit to the patient. This finding is a slight departure from the 2-year outcomes published by Chahla et al, 3 which found that the SLT cohort had greater odds of achieving PASS for mHHS than did the LLT cohort. Similarly, pain relief quantified by the VAS, patient satisfaction with the treatment and regimen, and whether the patient would choose the same procedure again had no significant difference across cohorts, indicating that along with symptom and pain relief, patients also had a positive perception of the surgery and their experience no matter the size of their labral tear.
While intraoperative findings do not solely dictate a reasonable and comprehensive treatment plan for labral tears, understanding the influence of key variables such as labral tear size on long-term patient outcomes and its influence on survivorship after hip arthroscopy surgery can be valuable. This present study is the first to evaluate how labral tear size can affect the rate of conversion to THA. The weighted Cox regression demonstrated that even when adjusting for significant covariates such as age and Tönnis grade, being in the LLT cohort yielded over twice the rate of conversion to THA as opposed to a 10-year increase in age or a single-unit increase in Tönnis grade. Men had a lower rate of conversion compared with women. While this did not reach statistical significance, the inclusion of sex in the model produced results (less risk for men) that fit with current understanding of risk for conversion. Further, including sex in the model, despite the lack of statistical significance, improved the estimation of labral tear size, Tönnis grade, and age, as it allows these variables to be properly adjusted for sex-based differences. Additionally, the finding that the LLT cohort exhibited a greater frequency of grades 3 and 4 chondrolabral junction breakdown supports the findings of Dean et al 5 that worse chondrolabral junction breakdown will result in increased likelihood of THA conversion. Several factors, including the extent of cartilage damage and labral tear size, are accounted for when opting for labral repair/reconstruction versus debridement, but it is difficult to conclude from the results of this study whether more aggressive attempts at labral repair/reconstruction can compensate for the differences seen between those with LLT and SLT. 20 Several studies including one analyzing 5-year follow-up outcomes after hip arthroscopy by Domb et al 7 have identified age and Tönnis grade as significant predictors of outcomes and conversion to THA over time, making it exceedingly interesting that the present study analyzing long-term follow-up finds labral tear size to be an even more influential predictor.
Limitations
This study has several limitations. First, this study utilized a retrospective patient registry resulting in an inability to compare patient postoperative outcomes at the latest follow-up time point with their baseline function. However, this did not disrupt our ability to effectively characterize patient conversion to THA and the relative significance of other covariates. Second, the senior surgeon's surgical technique has varied since the time at which patients included in this study had their respective procedure, as currently, patients primarily receive labral repairs with capsular autograft augmentation as opposed to debridement. Also, even though all patients in this study were operated on by the same senior surgeon, the diversity in patients enrolled augmented the validity of our findings. Even so, this study's findings remain largely unaffected, as this comes with any study analyzing long-term outcomes for a surgical procedure in a constantly evolving field. Third, as this is a retrospective cohort study, the analysis presents associations between findings and postoperative outcomes without suggesting causation. With this in mind, we actively accounted for covariates wherever possible, ensuring a thorough analysis via targeted statistical analyses such as multiple variable linear regression analysis. Fourth, while PROM analyses were conducted only including the outcomes of patients who did not convert to THA, we believed that these data were worth sharing to understand postoperative outcomes between groups prior to THA conversion. Last, there is a chance that as the mean age of the LLT cohort was older than the SLT cohort, surgeons may be more biased towards offering THA earlier to LLT patients. Future studies could include examining a larger patient population size across different surgeons utilizing different techniques. Subanalysis for each individual technique observing outcomes and comparative rates for conversion to THA based on patient labral tear size could indicate how best to increase longevity of hip arthroscopy for symptomatic labral tears. Finally, the event rate was low (n = 29 conversions), which may raise concern of overfitting. To reduce the risk of an overfit, penalized regression models were fit to correct bias.
Conclusion
Primarily, those in the LLT cohort experienced a significantly greater conversion rate to THA than the SLT cohort but experienced no significant difference in pain relief. Also, labral tear size can independently predict certain long-term PROs after primary hip arthroscopy. Evaluating labral tear size can factor into identifying candidates who might benefit from additional measures to potentially prevent early conversion to total hip arthroplasty.
Footnotes
Acknowledgements
The authors thank the Conine Family Fund for Joint Preservation for their continued research support.
Final revision submitted November 24, 2025; accepted November 30, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study protocol was approved by the institutional review board of Mass General Brigham Integrated Health Care System (No. 2011P000053).