
Abstract
Background
Femoral torsion can be evaluated from different femoral segments. The pathological thresholds for femoral torsion of different segments and the influence of segmental femoral torsion on patellofemoral alignment remain unknown.
Purpose
To compare femoral torsion between patients with recurrent patellar dislocation and healthy individuals, to determine the statistical physiological range and pathological thresholds of femoral torsion in different segments, and to investigate the influence of femoral torsion on patellofemoral malalignment.
Study Design
Cross-sectional study; Level of evidence, 3.
Methods
We retrospectively reviewed the records of patients with patellar dislocation who received surgical treatment in our department between 2019 and 2020. Healthy participants were recruited as the control group. The control patients were asymptomatic and had no history of lower extremity disorders. The differences in femoral torsion between the study and control groups were compared. The diagnostic capacity of femoral torsion in different segments and their correlation with patellar tilt were investigated. The mean value and 95% CI of femoral torsion in different segments were established using data from healthy volunteers.
Results
A total of 60 patients with patellar dislocation and 100 healthy volunteers were included in this study. The total, mid, and distal femoral torsion values differed significantly between the study and control groups (P < .01). Total femoral torsion had the highest diagnostic value (area under the receiver operating curve = 0.733). Total torsion (r = 0.432; P < .001), mid torsion (r = 0.242; P = .002), and distal torsion (r = 0.324; P < .001) showed significant correlations with patellar tilt. The pathological thresholds of excessive femoral torsion of the total, proximal, mid, and distal femoral segments were 24.73°, 46.68°, –6.55°, and 14.92°, respectively.
Conclusion
Patients with patellar dislocation had greater femoral torsion than healthy individuals in multiple femoral segments. Excessive mid, distal, and total torsion was associated with more significant patellar tilt.
Patellar dislocation is an injury with a complex etiology. Traumatic factors, skeletal deformities, and ligamental abnormities contribute to patellar dislocation. 1,26,27,29,30 Excessive femoral torsion is a risk factor for patellar dislocation and may lead to anterior knee pain, maltracking of the patella, and early cartilage degeneration postoperatively. 16,31,33 –35 However, the role of femoral torsion in the incidence and progression of patellofemoral disorders was poorly understood in recent decades.
In recent studies, an increasing number of surgeons have emphasized the role of femoral torsion and femoral derotation osteotomy (FDO) in patient evaluation and treatment of patellar dislocation. 26,28,30,32,33 Seitlinger et al 23 established the method of femoral torsion evaluation in different femoral segments and ascertained their contribution to total torsion. Current studies have confirmed the reliability of femoral torsion measurements in different segments. 7 In addition, abnormal mid torsion and distal torsion were correlated with trochlear dysplasia and tibial tubercle malposition. 19,26,30 The evaluation of femoral torsion in the proximal, mid, and distal femoral segments could provide surgeons with more information about the femoral deformity and help them to formulate the treatment plan.
To date, there is a lack of studies comparing the difference in segmental femoral torsion between patients with patellar dislocation and healthy individuals. Moreover, the physiological range and pathological thresholds of femoral torsion at different segments, as well as their influence on patellofemoral malalignment, remain unknown. Previous studies have focused on correcting the total torsion of the distal femur without evaluating the torsion of the segment. However, deformities in the proximal and mid sites of the femur can also contribute to excessive femoral torsion. Whether torsion of the proximal or mid sites of the femur can influence clinical outcomes remains unknown. Therefore, we should pay more attention to torsion at other femoral segments.
The purpose of this study was to compare segmental femoral torsion between patients with recurrent patellar dislocation and healthy individuals. Then, we determined the thresholds of femoral torsion in different segments based on the asymptomatic cohort that we recruited. Finally, we investigated the influence of femoral torsion in different segments on patellar tilt. We hypothesized that we would find significant differences in femoral torsion at different femoral segments between patients with patellar dislocation and healthy individuals and that the values of femoral torsion at different femoral segments would show a correlation with patellar tilt.
Methods
Study Population
The protocol for this study was approved by the ethics committee of our hospital, and informed consent was obtained from study participants. We retrospectively reviewed the data from 232 patients with patellar dislocation who were receiving surgical treatment in our department from January 2019 to January 2020. Patients with >1 of the following criteria were excluded from this study: first-time patellar dislocation (n = 21); patellar dislocation caused by car accidents or other high-energy force directly on the patella (n = 24); multiple-ligament rupture (n = 7); previous fracture or surgery of the lower limb (n = 26); and having no records of necessary clinical, operative, or radiological data (n = 6). The 6 patients without necessary data were excluded because they did not undergo the computed tomography (CT) examination from the hip to the knee joint at 1 time. After the application of exclusion criteria, 148 patients remained. Of these patients, 60 were randomly selected according to their admission date to the hospital.
To establish the physiological range and pathological thresholds of femoral torsion at different segments, 100 volunteers without a history of lower extremity symptoms and injuries were recruited as the control group (Figure 1). To avoid the potential influence of anatomic differences between female and male patients on femoral torsion, the ratio of men to women in the control group was equal. Two orthopaedic surgeons (H.W., J.-K.Y.) from our department performed medical history inquiries and physical examinations of the volunteers to exclude participants who had obvious skeletal deformities and other potential lower limb disorders. Finally, to ensure the comparability between the study and control groups, we examined the control group data to ensure that there were no significant differences in age, sex, or examination of the knee joint.
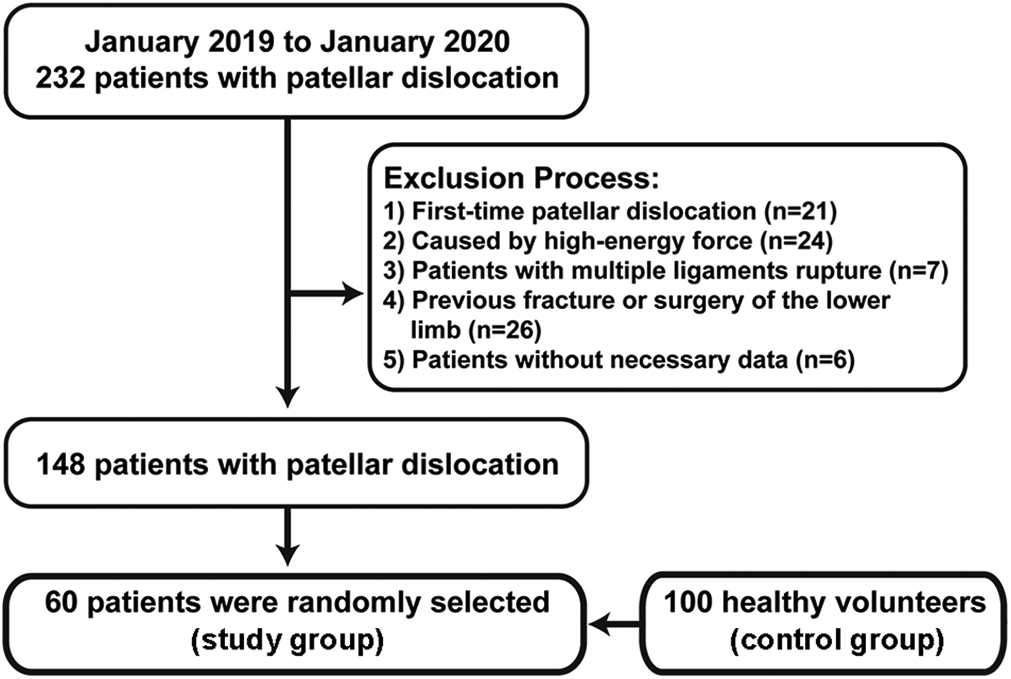
Flowchart showing the allocation of the study participants.
CT Examination
All patients diagnosed with patellar dislocation during the study period underwent preoperative CT scans from the hip to the knee joint, regardless of whether they had excessive femoral torsion. Patients and controls underwent CT examination using the same protocol. In patients with patellar dislocation, CT examinations were performed within 1 week before surgery for surgical planning. Images were obtained with a 64-slice spiral CT scanner (Siemens Healthcare). All patients underwent examinations in the supine position with the knee at full extension and with the foot positioned in the neutral position. The scanning range was from the anterosuperior iliac spine to 5 cm below the tibial plateau. The scanning parameters were as follows: slice thickness, 0.625 mm; pitch, 1.0; tube voltage, 130 kVp; tube current, 110 to 140 mAs; and matrix, 512 × 512 pixels. The field of view varied depending on whether 1 or both sides of the lower limb were examined, ranging from 220 to 450 mm. Acquired data were reformatted with a slice thickness of 5 mm; axial, coronary, and sagittal scanning were routinely performed.
Femoral Torsion Measurement
The measurement of femoral torsion was performed on a CT scan according to the Seitlinger method. 23,26 A total of 4 lines were drawn to measure femoral torsion in different femoral segments. The first line passed through the center of the femoral head and femoral neck (Figure 2A). This line was drawn by overlapping 2 CT slices: One represented the slice with the largest diameter of the femoral head, and the other represented the first slice that showed the femoral neck. The second line passed through the center of the femur and the midpoint of the lesser trochanter (Figure 2B). The third line was drawn tangent to the posterior aspect of the distal femur just superior to the gastrocnemius attachment (Figure 2C). The fourth line was drawn tangent to the posterior femoral condyles in the most proximal CT slice that showed an intact Roman arch and the posterior femoral condyles (Figure 2D). The angle between the first line and the fourth was regarded as the total femoral torsion; the angle between the first line and the second was considered the proximal torsion; the angle between the second line and the third was considered the mid torsion; and the angle between the third line and the fourth was considered distal torsion. If the proximal line was internal rotation related to the distal line, the torsion value was considered positive.
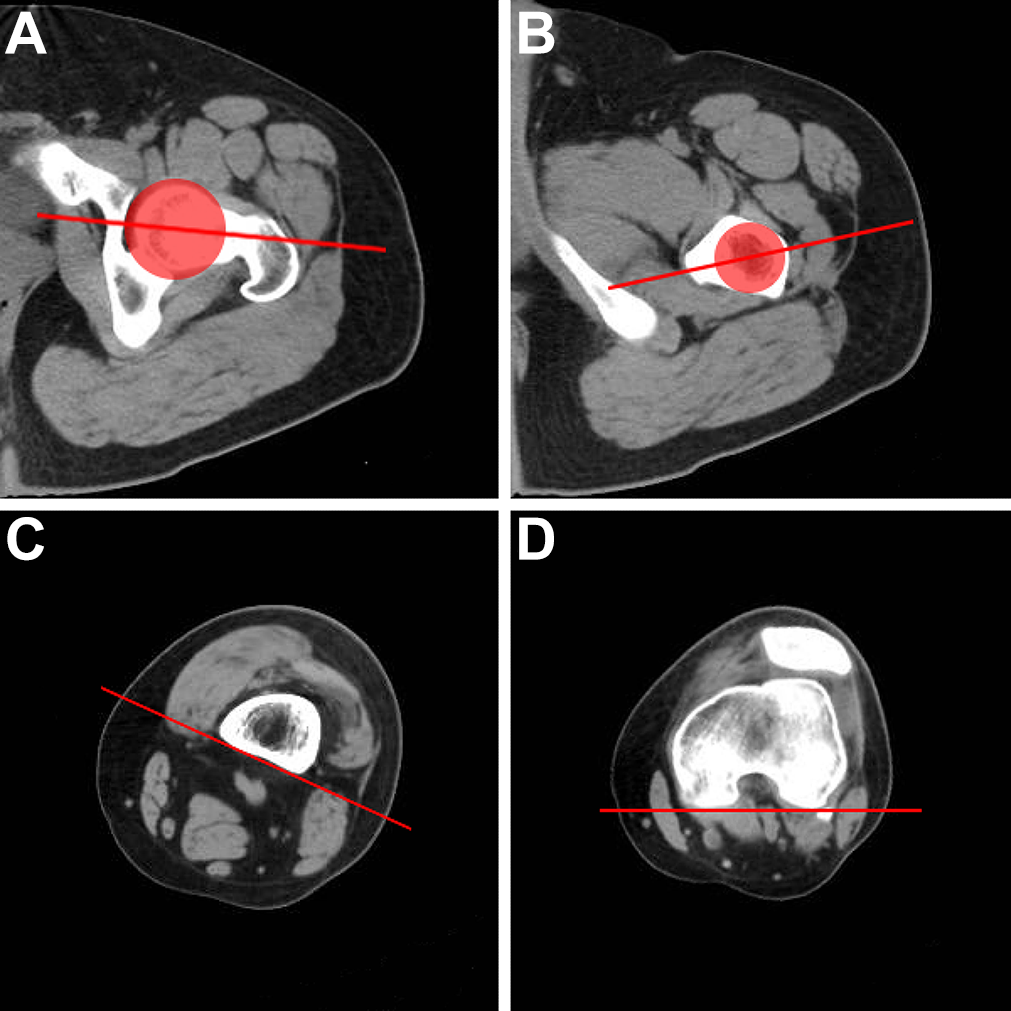
Measuring torsion on different left femoral segments. (A) The overlapping images of the CT slice with the largest diameter of the femoral head and the most proximal CT slice with visualization of the femoral neck. The first line passes through the center of the femoral head and femoral neck. (B) The most proximal CT slice shows an intact lesser trochanter. The second line passes through the center of the femur and the midpoint of the lesser trochanter. (C) The CT slice just superior to the attachment of the gastrocnemius. The third line is tangent to the posterior aspect of the femur. (D) The most proximal CT slice with an intact Roman arch and posterior femoral condyles. The fourth line is tangent to the posterior femoral condyles. CT, computed tomography.
Patellar Tilt
The patellofemoral malalignment was quantified by patellar tilt measurement. The patellar tilt value is the angle between the line along the largest width of the patella and the tangent line of the posterior femoral condyles. 33 The tangent line of the posterior femoral condyles was the same as the fourth line in the femoral torsion measurement (Figure 3).

The method of measuring patellar tilt on the left knee. The patellar tilt angle was defined as the angle of (A) the tangent line of the posterior femoral condyles and (B) the largest width of the patella.
Measurements of Parameters
All measurements were performed by 2 surgeons (Z.X., Y.S.) with >10 years of sports medicine clinical practice. All measurements were simultaneously performed in a blinded and randomized fashion to determine interobserver reliability. To evaluate the intraobserver reliability, the senior surgeon (H.W.) reexamined all the measurements after 4 weeks. The average values measured by the 2 observers were used for comparison.
Statistical Analysis
All data were entered into SPSS software (Version 24.0; IBM) for statistical analysis. The intraclass correlation coefficients (ICCs) were calculated to evaluate the inter- and intraobserver reliabilities of the measurements. ICC values ranged from 0 to 1, and an ICC value >0.75 indicated excellent agreement. After the Kolmogorov-Smirnov test confirmed the normal distribution of all parameters, the differences between the study group and the control group were analyzed using unpaired t tests. Receiver operating characteristic (ROC) curves were generated to compare the capacities of segmental femoral torsion in distinguishing patients and healthy individuals. Pearson correlation analysis was performed to evaluate the contribution of femoral torsion in different segments to the total torsion and patellar tilt. The physiological range and pathological thresholds for femoral torsion in different segments were determined according to the mean and standard deviation of measurements (mean ± 1.96 SD) derived from healthy volunteers. P < .05 was considered significant.
To determine the suitable sample size of this study, G*Power software (Version 3.1.9.4) was applied to perform power analysis. A priori power analysis based on an effect size of 0.8 determined a sample size of 70 participants. At least 35 patients in each group were adequate to detect significant differences with a power of 95% and an α = .05.
Results
The detailed characteristics of the study and control groups are presented in Table 1. There were no significant differences between the groups.
Comparison of the Study and Control Groups a

a Data are presented as mean ± SD or No. Bold P values indicate statistically significant difference between groups (P < .05).
b If the proximal line was internally rotated as related to the distal line, the torsion value was considered positive.
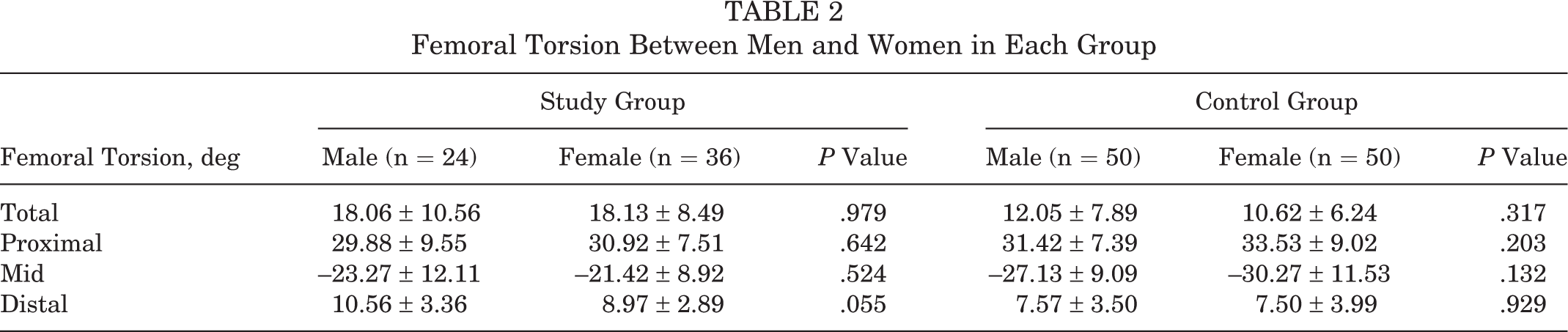
The total, mid, and distal femoral torsion measurements in the study group were significantly higher than those of the control group (P < .01) (Table 1). The results showed no significant difference in proximal torsion between the study group (30.50° ± 8.33°) and the control group (32.47° ± 7.95°) (P = .188). Moreover, there was no significant difference in the value of femoral torsion of different femoral segments between male and female patients (Table 2). All the measurements of femoral torsion at different levels showed excellent agreement in terms of inter- and intraobserver reliability, with ICCs >0.914 (Table 3).
Femoral Torsion Between Men and Women in Each Group
Inter- and Intraobserver Reliability of the Measurements

a An intraclass correlation coefficient >0.75 indicates excellent agreement.
The results of the ROC curve analysis showed that total femoral torsion had the highest diagnostic capacity, with an area under the curve (AUC) of 0.733. The diagnostic capacities of mid and distal torsion showed only a slight difference, with AUCs of 0.651 and 0.661, respectively. Proximal torsion did not show a significant difference between patients and healthy individuals, so we did not perform a ROC curve analysis for this parameter (Figure 4).

Receiver operating characteristic curves of total, mid, and distal femoral torsion. AUC, area under the curve.
The results of the Kolmogorov-Smirnov test showed that the values of femoral torsion in each of the 4 levels were distributed normally. Therefore, the mean and standard deviation of the data in the control group (mean ± 1.96 SD) were used to calculate the physiological range and pathological thresholds for excessive femoral torsion at different femoral segments. The pathological threshold values of excessive total, proximal, mid, and distal femoral torsion were 24.73°, 46.68°, –6.55°, and 14.92°, respectively (Table 4). In the control group, the proportion of patients whose femoral torsion in any segment exceeded this range was <5%.
Physiological Range and Pathological Thresholds of Femoral Torsion at Different Segments

Total (r = 0.432; P < .001), mid (r = 0.242; P = .002), and distal (r = 0.324; P < .001) femoral torsion showed significant correlations with patellar tilt. Total femoral torsion was significantly correlated with proximal (r = 0.243; P = .02) and mid (r = 0.578; P < .001) femoral torsion. Proximal femoral torsion was significantly correlated with mid femoral torsion (r = –0.554; P < .001). Femoral torsion in other segments was not statistically correlated (Figure 5).

Correlation of femoral torsion between different segments and their contribution to patellofemoral malalignment. (A) Correlation between total torsion and proximal torsion. (B) Correlation between total torsion and mid torsion. (C) Correlation between mid torsion and proximal torsion. (D) Correlation between patellar tilt and total torsion. (E) Correlation netween patellar tilt and mid torsion. (F) Correlation between patellar tilt and distal torsion.
Discussion
The most important finding of this study is that patients with patellar dislocation have greater femoral torsion in the total, mid, and distal femoral segments. The pathological threshold values for excessive femoral torsion at different femoral segments were established according to this finding, which provides the theoretical basis for torsion region determination, surgical indication, and postoperative radiological evaluation. Moreover, femoral torsion in the total, mid, and distal femoral segments positively correlated with patellar tilt, suggesting that patellofemoral malalignment was not simply influenced by torsion between the proximal and distal femoral segments. The torsion of the mid and distal femoral segments also contributes to patellofemoral malalignment.
We established the physiological range and pathological thresholds of femoral torsion in different segments in 100 healthy individuals. The previous studies included only a small sample of patients, which is insufficient to obtain statistical significance or convincing results. Moreover, this is the first study that confirms the influence of mid and distal femoral segments on patellofemoral malalignment. The present study provided a theoretical basis for pre- and postoperative evaluation and suggested issues for further investigation.
The most evident finding of this study is that total, mid, and distal torsion was greater in patients with patellar dislocation than in healthy individuals. The ROC curve suggested that the total torsion measurement has the highest capacity to distinguish patients with and without patellar dislocation, and the mid and distal femoral torsion also has a good diagnostic capacity with an area under the curve >0.65. Excessive femoral torsion is reported as a risk factor for patellar dislocation. 3,10,15 Therefore, increased femoral torsion warrants the consideration of FDO in patients with patellar dislocation. 8,11,17,32 –34 Although the measurements of femoral torsion have proven to be helpful in treating these kinds of patients, the pathological threshold for these measurements has remained controversial for decades. 7,12,22,24,25 In addition, previous studies failed to offer a suitable femoral level for osteotomies. 2,5,20,26 In the present study, we compared the differences in femoral torsion between patients with patellar dislocation and healthy individuals. The results of our study showed that excessive femoral torsion most frequently presented in the total, mid, and distal femoral segments in patients with patellar dislocation (P < .01). However, there was not a significant difference in proximal femoral torsion between patients and healthy individuals (P = .188). These results suggested that sites of the mid and distal femur may be suitable levels for osteotomy. These results make us wonder whether the performance of osteotomy in regions with abnormal femoral torsion could achieve a better clinical outcome. Therefore, the establishment of the physiological range of femoral torsion of the femoral segments is crucial for future investigation.
Nelitz et al 21 found that femoral torsion >20° was considered a moderate risk factor for patellofemoral instability. In comparison, femoral torsion >25° was a severe risk factor. They believed that in patients with total femoral torsion >25°, FDO should be recommended to correct the excessive rotational deformity of the lower limb. However, they could not provide statistical evidence for using this value as an indication for surgery. In the present study, the Kolmogorov-Smirnov test was used to evaluate the distribution of the included parameters. The mean and standard deviation of the measurement in 100 healthy volunteers were used to calculate the physiological range and pathological thresholds for femoral torsion in different femoral segments. The results regarding total torsion in this study are consistent with Nelitz and colleagues’ findings that total femoral torsion >25° is the indication for FDO in patients with patellar dislocation. This study established the physiological range and pathological thresholds for femoral torsion in different femoral segments. A possible implication of this study could be the extended clinical indication of the FDO procedure. The establishment of pathological thresholds in proximal, mid, and distal femoral segments can help surgeons identify the region of femoral torsion in patients with patellar dislocation. Whether patients with uncorrected segmental femoral torsion would affect postoperative outcomes needs to be investigated.
In current studies, most authors evaluate femoral torsion by calculating the angle between a line parallel to the center of the femoral neck and a line tangent to the posterior femoral condyles. 11,13,14,24,31,33 However, Seitlinger et al 23 suggested that torsion of the femur originates from different femoral segments. They established a method to evaluate femoral torsion and concluded that femoral torsion at 3 levels contributes to total femoral torsion. The Seitlinger et al study included only 30 healthy individuals. Given the insufficiency of the sample size, that study failed to establish pathological thresholds for excessive proximal, mid, and distal torsion, so it was difficult to evaluate femoral torsion in different segments. In the present study, the pathological thresholds of segmental femoral torsion were calculated using healthy participants with a suitable sample size, which makes up for the deficiency of the previous study.
Another relevant finding of this study was that excessive total femoral torsion, mid femoral torsion, and distal torsion are related to patellar tilt. The angle of patellar tilt indicates the alignment of patellofemoral joints. 9,18 The patellar tilt was increased in patients with patellar dislocation and returned to normal after isolated medial patellofemoral ligament reconstruction or combined procedures. 6,33 The tilt of the patella can be affected by multiple anatomic factors in patients with patellar dislocation. Cilengir et al 4 reported that trochlear dysplasia, tibial tubercle lateralization, and patellar tendon angle contributed to abnormal patellar tilt. The results of the present study indicated that abnormal torsion in the mid and distal femur is also a contributor to patellofemoral malalignment.
Limitations
A limitation of this study was that we could not ascertain that the participants in the control group were all within the normal range of femoral torsion, although detailed medical history inquiries and physical examinations of every healthy volunteer were performed to exclude patients with lower limb disorders. To reduce the impact of this bias on our study, we recruited a total of 100 healthy volunteers.
Conclusion
Patients with patellar dislocation had greater femoral torsion than healthy individuals in multiple femoral segments. Excessive mid, distal, and total torsion was associated with more significant patellofemoral malalignment. The pathological thresholds of excessive femoral torsion of total, proximal, mid, and distal femoral segments were 24.73°, 46.68°, –6.55°, and 14.92°, respectively.
Footnotes
Final revision submitted June 12, 2022; accepted July 24, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Peking University Third Hospital Cohort Construction Project (grant BYSYDL2021001), the Beijing Natural Science Foundation (grant J210011), and the Foundation From Peking University Health Science Center (0714-EMTC-02-00897). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital (approval No. IRB00006761-M2021423).