
Abstract
Background:
Recurrent patellar dislocation in children and adolescents is a multifactorial condition associated with anatomic risk factors such as patella alta, trochlear dysplasia, and torsional deformities of the lower limb. Although medial patellofemoral ligament reconstruction (MPFLR) is the standard approach, undetected torsional abnormalities may compromise outcomes. While computed tomography (CT) offers precise femoral torsion (FT) and tibial torsion (TT) evaluation, its widespread use is constrained by cost and radiation exposure.
Purpose:
To evaluate whether conventional radiographic parameters can predict excessive lower limb torsion in patients undergoing MPFLR.
Study Design:
Cohort Study (Diagnosis); Level of evidence, 3.
Method:
The authors retrospectively analyzed 104 knees (70 patients) evaluated using CT for FT, TT, and combined torsion (FT+TT) between December 2016 and December 2023. Radiographic measures included the Caton-Deschamps index, congruence angle, sulcus angle, and patellar tilt angle. FT and TT were categorized as <20°, 20° to 30°, or >30°, and FT+TT as <40°, 40° to 50°, or >50°. Receiver operating characteristic (ROC) analysis and multivariate regression were used to assess the diagnostic performance of radiographic variables.
Results:
The patellar tilt angle was significantly associated with FT (r = 0.24; P = .015) and FT+TT (r = 0.27; P = .009). ROC analysis showed the highest predictive accuracy for patellar tilt angle, with an area under the curve of 0.629 for FT >20°, 0.653 for FT >30°, and 0.665 for FT+TT >50°. A threshold of 20° was identified across categories. Body mass index (β = −0.461; P = .019) and patellar tilt angle (β = 0.222; P = .021) were independent predictors of FT (adjusted R2 = 0.102).
Conclusion:
This study showed that although patellar tilt angle demonstrated the highest predictive value among evaluated parameters, its diagnostic accuracy was limited and insufficient to replace cross-sectional imaging. Comprehensive preoperative evaluation of lower limb torsion remains critical for minimizing residual instability and improving outcomes after MPFLR.
Keywords
Recurrent patellar dislocation is among the most common acute knee disorders in children and adolescents.2,11 Patella alta, trochlear dysplasia, and lower limb torsion are key anatomic risk factors.2,12,21 Medial patellofemoral ligament reconstruction (MPFLR) is a widely accepted surgical intervention 7 ; however, unrecognized torsional deformities may lead to persistent instability or suboptimal postoperative outcomes.16,17
Computed tomography (CT) is the most accurate modality for evaluating lower limb torsion, allowing for measurement of femoral torsion (FT) and tibial torsion (TT). 10 However, whole-limb CT involves increased radiation exposure—approximately 2.5 to 3.0 mSv per scan—and costs 300 to 600 US dollars, limiting its routine use, especially in younger patients. 10 Recent prospective studies have demonstrated that magnetic resonance imaging (MRI)–based torsion measurement provides equivalent reliability and validity to CT while avoiding ionizing radiation. 5 Nevertheless, MRI is relatively time-consuming and may be contraindicated in patients with metallic implants. Although CT remains more practical for routine preoperative assessment and in situations where rapid imaging is required, the absence of standardized CT criteria further contributes to variability in preoperative assessments.
Previous studies using CT imaging have reported correlations between patellar tilt angle, tibial tubercle–trochlear groove (TT-TG) distance, and femoral anteversion in patients with recurrent patellar dislocation. 6 However, these studies primarily evaluated relationships among measurements evaluated on CT, rather than assessing whether conventional radiographic findings could predict torsional deformities. Thus, in this study, we aimed to evaluate whether conventional radiographic parameters could predict excessive lower limb torsion in patients undergoing MPFLR. We hypothesized that conventional radiographic parameters, such as the sulcus angle and patellar tilt angle, would correlate with and predict excessive lower limb torsion in patients with recurrent patellar dislocation.
Methods
Ethics Statement
The study procedures adhered to the ethical standards of the institutional and/or national research committee and the principles of the 1964 Declaration of Helsinki and its later amendments or comparable standards. All patients provided written informed consent, and the study was approved by the ethics committee of Hirosaki University (approval No. 2014-229).
Participants
This retrospective study included 104 knees (70 patients) with lateral patellar instability—with or without recurrent dislocation—that underwent isolated MPFLR between December 2016 and December 2023 at Hirosaki University. In this study, only patients who underwent isolated MPFLR were included; no concomitant procedures such as tibial tubercle osteotomy or trochleoplasty were performed. Contraindications of isolated MPFLR included high-grade trochlear dysplasia (Dejour type D), significant patellofemoral osteochondral lesions (ie, Outerbridge grade 3 or 4), and skeletal immaturity. 7 Preoperative demographic data, including age, sex, and body mass index (BMI), were obtained retrospectively from medical records.
Surgical Management
MPFLR was performed using FiberTape and knotless SwiveLock anchors (Arthrex).7,20,21,24 FiberTape was anchored to the medial patella and femur (Schöttle point) with the knee at 90° of flexion. Based on our previous biomechanical and clinical findings, fixation was performed at 90° of knee flexion to prevent excessive patellofemoral contact pressure while maintaining appropriate medial stability. 19 Final arthroscopic evaluation confirmed appropriate tracking. Postoperative rehabilitation emphasized early restoration of range of motion and quadriceps activation. Patellar setting and straight leg raise exercises were initiated immediately after surgery. Weightbearing was allowed as tolerated, and jogging was typically permitted at approximately 8 weeks postoperatively. No knee braces or orthotic devices were used. All patients followed the same standardized rehabilitation protocol. Return-to-sport clearance was determined individually through consultation between the surgeon and rehabilitation team, although no formal objective return-to-sport criteria (eg, limb symmetry index testing) were applied.
Radiographic Measurements
Radiographic assessments were performed on weightbearing anteroposterior, lateral, and Laurin views with the knee flexed at 30°. All measurements were obtained using PACS software (ShadeQuest/ViewR; Fujifilm Medical Co) by 2 independent observers (K.I. and H.K.I.), with a precision of 0.1° for angles and 0.1 mm for distances. On the Laurin view, the sulcus angle was defined as the angle formed by 2 lines drawn from the deepest point of the trochlear groove to the most anterior aspects of the medial and lateral femoral condyles. 9 The congruence angle was measured as the angle between the bisector of the sulcus angle and a line extending from the trochlear groove to the apex of the patellar ridge, with lateral deviation designated as positive and medial deviation as negative. 23 The patellar tilt angle was measured as the angle between a line connecting the most anterior points of the medial and lateral femoral condyles and a second line across the maximal transverse width of the patella. 4 On the lateral radiograph, the Caton-Deschamps (CD) index was calculated as the ratio of the distance from the inferior end of the patellar articular surface to the anterior superior angle of the tibial plateau to the length of the patellar articular surface (Figure 1). 14

Radiographic measurements. (A) The sulcus angle is formed by lines drawn from the deepest point of the trochlear groove to the most anterior aspects of the medial and lateral femoral condyles. (B) The congruence angle is measured between the bisector of the sulcus angle and a line from the trochlear groove to the apex of the patellar ridge. (C) The patellar tilt angle is defined as the angle between a line connecting the most anterior points of the femoral condyles and another line across the maximal transverse width of the patella. (D) The Caton-Deschamps index is the ratio of the distance from the inferior end of the patellar articular surface to the anterior superior angle of the tibial plateau (solid line) to the length of the patellar articular surface (dashed line).
Lower Limb Torsion Evaluation
As previously reported, 17 FT and TT were measured using anatomic reference lines (Figure 2). FT was defined as the angle between a line through the femoral head and neck and a line tangent to the posterior femoral condyles. TT was the angle between a line along the posterior tibial plateau and a line connecting the centers of the medial and lateral malleoli. Combined torsion was the sum of FT and TT (FT+TT). Based on a previous study, 7 patients were classified according to each parameter as follows: FT was divided into <20°, 20° to 30°, and >30°; TT was divided into <20°, 20° to 30°, and >30°; and FT+TT was divided into <40°, 40° to 50°, and >50°.

Measurement of femoral torsion and tibial torsion on computed tomography axis cuts. Femoral torsion was determined by the angle formed between (A1) a line passing through the center of the femoral head and neck and (A2) a second line tangent to the posterior femoral condyles. Tibial torsion was measured using the angle between (B1) a line tangential to the posterior edge of the tibial plateau and (B2) a second line connecting the centers of the medial and lateral malleoli.
All CT-based measurements were performed using ShadeQuest. Interobserver reliability was tested by 2 independent reviewers in 40 randomly selected patients. To assess intraobserver reliability, 1 observer (K.I.) repeated the measurements for the same subset of patients 4 weeks after the initial evaluation. Reliability was classified as excellent (ICC, >0.75), fair to good (ICC, 0.40-0.75), or poor (ICC, <0.40). The values used in this analysis were not averaged between observers.
Statistical Analysis
Statistical analysis was conducted using SPSS software (Version 29.0; IBM). Continuous variables are summarized as means and standard deviations and categorical variables as frequencies. The Shapiro-Wilk test was used to assess data normality.
Spearman rank correlation was used to analyze associations among alignment parameters. Receiver operating characteristic (ROC) analysis assessed the predictive performance of radiographic parameters (CD index, congruence angle, sulcus angle, and patellar tilt angle) for excessive lower limb torsion. The false-positive fraction was plotted against the true-positive fraction, and the cutoff value was defined at the point of maximum slope—the nearest point to true positive. The area under the curve (AUC) was used to determine diagnostic accuracy. Univariate and multivariate linear regression analyses were performed to identify predictors of lower limb torsion. Independent variables included age, BMI, CD index, congruence angle, sulcus angle, and patellar tilt angle. A stepwise method was used for multivariate analysis, and adjusted R2 values indicated model fit. Statistical significance was set at a P value <.05.
Results
There were 32 male knees and 72 female knees, with a mean age of 17.3 ± 5.6 years (range, 11-39 years) and mean BMI of 24.3 ± 4.9 kg/m2 (range, 16-38 kg/m2). Intraclass correlation coefficients (ICC, 2.1) demonstrated excellent reliability: 0.821 (95% CI, 0.539-0.818; P < .001) for FT and 0.793 (95% CI, 0.492-0.700; P < .001) for TT. 14 Intraobserver reliability was determined to be excellent, with ICC values of 0.894 (95% CI, 0.812-0.945) for FT and 0.865 (95% CI, 0.768-0.932) for TT. Patients were classified according to FT, TT, and FT+TT. A total of 43 knees exhibited FT <20°, 34 had FT between 20° and 30°, and 27 had FT >30°. For TT, 45 knees demonstrated TT <20°, 48 had TT between 20° and 30°, and 11 had TT >30°. Regarding FT+TT, 42 knees had FT+TT <40°, 50 had FT+TT between 40° and 60°, and 12 had FT+TT >50° (Table 1).
Patient Data and Radiographic Parameters a
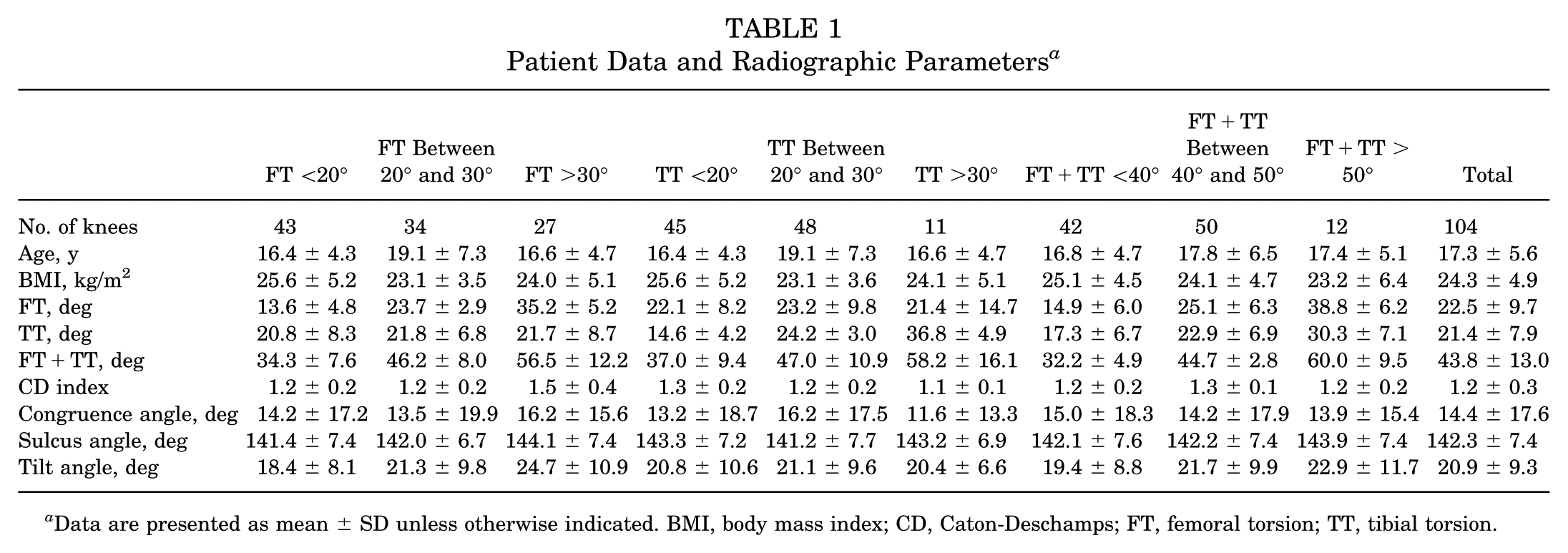
Data are presented as mean ± SD unless otherwise indicated. BMI, body mass index; CD, Caton-Deschamps; FT, femoral torsion; TT, tibial torsion.
Spearman rank correlation revealed a strong positive correlation between FT and FT+TT (r = 0.79; P < .001) and a moderate correlation between TT and FT+TT (r = 0.67; P < .001). The patellar tilt angle was significantly associated with FT (r = 0.24; P = .015) and FT+TT (r = 0.27; P = .009). However, neither the CD index nor the sulcus angle showed significant correlations with torsional measurements (Table 2).
Correlations Among Alignment Parameters a

Statistical analysis was conducted using the Spearman rank correlation coefficient. Spearman rank correlation revealed significant associations between FT and FT+TT (r = 0.79; P < .001), TT and FT+TT (r = 0.67; P < .001), patellar tilt angle and FT (r = 0.24; P = .015), and patellar tilt angle and FT+TT (r = 0.27; P = .009). *P < .05; **P < .001. CD, Caton-Deschamps; FT, femoral torsion; TT, tibial torsion.
ROC analysis identified the patellar tilt angle as the most predictive radiographic parameter for excessive FT. The AUC for predicting FT >20° was 0.629 (P = .026; cutoff = 19°; 95% CI, 0.521-0.736), and for FT >30°, the AUC was 0.653 (P = .019; cutoff = 20°; 95% CI, 0.538-0.768). For predicting FT+TT >50°, the AUC was 0.665 (P = .009; cutoff = 20°; 95% CI, 0.551-0.779) (Table 3).
ROC Analysis of Radiographic Predictors for Excessive Lower Limb Torsion a

When using the patellar tilt angle as a predictor, the AUC was 0.629 (P = .026; 95% CI, 0.521-0.736) for predicting FT >20° and 0.653 (P = .019; 95% CI, 0.538-0.768) for predicting FT >30°. The patellar tilt angle also exhibited the highest discriminatory performance among the evaluated parameters for identifying FT+TT >50°, with an AUC of 0.665 (P = .009; 95% CI, 0.551-0.779). *P < .05. AUC, area under the curve; CD, Caton-Deschamps; FT, femoral torsion; ROC, receiver operating characteristic; TT, tibial torsion.
Multivariate linear regression identified BMI (β = −0.461; P = .019) and patellar tilt angle (β = 0.222; P = .021) as independent predictors of FT (adjusted R2 = 0.102) (Table 4). The estimated FT was calculated using the following equation: FT = 29.3 – 0.461 × BMI + 0.221 × patellar tilt angle. No independent predictors were identified for TT or FT+TT.
Univariate and Multivariate Analyses of the Predictors of FT a

Multivariate linear regression analysis identified BMI (β = −0.461; P = .019) and patellar tilt angle (β = 0.222; P = .021) as independent predictors of FT. BMI, body mass index; CD, Caton-Deschamps; FT, femoral torsion.
Discussion
The principal finding of this study was that the patellar tilt angle was significantly associated with both FT and FT+TT and demonstrated the strongest predictive value among the radiographic parameters analyzed. Although identified as an independent predictor of FT in multivariate analysis, its discriminative ability remained limited, with AUC values of 0.629 for FT >20° and 0.653 for FT >30°.
CT remains the gold standard for assessing lower limb torsion due to its high accuracy and reproducibility. However, concerns regarding radiation exposure persist. 10 MRI provides a radiation-free alternative with comparable accuracy and is particularly suitable for pediatric patients or those requiring repeat imaging. 5 EOS biplanar radiography offers a low-dose alternative with near-CT accuracy and 3-dimensional reconstruction capabilities. 1 Nonetheless, routine use of these imaging modalities is not always feasible due to insurance constraints, radiation considerations, and health care costs.
Lower limb torsion plays a critical role in patellar stability. Excessive FT increases lateralizing forces on the patella, predisposing patients to recurrent instability and suboptimal outcomes after isolated MPFLR.15,20,25 Normal FT in adults typically ranges from 15° to 25°, whereas TT ranges from 20° to 40°.13,18 Deviation beyond these values may necessitate corrective osteotomy rather than soft tissue reconstruction alone. 22
It has been shown that patients with recurrent patellar dislocation have greater patellar tilt angles compared with healthy individuals (29° vs 15°). 8 An increased patellar tilt angle is often associated with other anatomic abnormalities, such as an elevated TT-TG distance and excessive FT on CT. 6 It has also been shown that patients with recurrent patellar dislocation have a mean patellar tilt angle, FT, and TT-TG distance that are significantly higher than those in healthy controls (approximately 11°, 30°, and 9 mm vs 6°, 22°, and 6 mm, respectively; P < .001). 6 Furthermore, patellar tilt angle positively correlated with both FT (r = 0.53) and TT-TG distance (r = 0.39). While these findings are consistent with our results, the present study expands on prior work by evaluating FT and TT simultaneously and establishing cutoff values for excessive torsion—areas that have been underexplored in previous research. Despite its clinical relevance, the predictive power of the patellar tilt angle was limited. Therefore, although a tilt >20° should raise clinical suspicion for excessive FT, it cannot replace direct torsional measurements via advanced imaging. Although BMI showed a statistically significant negative association with FT, the underlying mechanism remains uncertain. However, this finding aligns with previous observations suggesting that increased mechanical loading in adolescents with higher BMI may accelerate the physiological reduction of FT during growth. 3 Overall, whether patients require whole-limb CT or MRI remains debated; however, selective use in patients with pronounced patellar tilt or other clinical indicators may offer a balanced approach.
This study has some limitations. First, the predictive model for FT exhibited only modest explanatory power (adjusted R2 = 0.102), indicating that additional anatomic or clinical factors not included in this study, such as 3-dimensional bone morphology, soft tissue characteristics, or demographic variations, may also influence FT and should be considered in future analyses. Second, the retrospective and single-center nature of the study may limit generalizability. Nonetheless, these findings suggest that although the patellar tilt angle provides useful screening information, it is insufficient as a stand-alone diagnostic marker. Preoperative torsional evaluation remains essential for patients with recurrent patellar instability, as unrecognized deformities may compromise MPFLR outcomes. Future research should focus on refining predictive models through integration of radiographic, clinical, and biomechanical data and evaluating the role of low-dose or artificial intelligence–based imaging workflows to enhance diagnostic precision while minimizing harm.
Conclusion
Our study showed that although patellar tilt angle demonstrated the highest predictive value among evaluated parameters, its diagnostic accuracy was limited and insufficient to replace cross-sectional imaging. Comprehensive preoperative evaluation of lower limb torsion remains critical for minimizing residual instability and improving outcomes after MPFLR.
Footnotes
Final revision submitted December 8, 2025; accepted December 13, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Hirosaki University Ethics Committee (approval No. 2014-229).