
Abstract
Background:
Recurrent patellar dislocation (RPD) is a common condition, particularly in adolescents, with several anatomic factors, such as increased femoral torsion, contributing to its development. Accurate assessment of these factors is essential for effective diagnosis and treatment planning.
Purpose:
To examine the correlation between femoral torsion and RPD and to measure the level of torsion using magnetic resonance imaging (MRI).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 212 individuals were initially screened. Of these, 22 patients (31 femurs) who satisfied the inclusion criteria were included in the final analysis as the study group. The control group consisted of 28 patients (28 femurs) without a history of RPD. MRI measurements were conducted across 3 distinct axial sections. Supratrochanteric torsion (STT) value, infratrochanteric torsion (ITT) value, and femoral anteversion were analyzed utilizing T2-weighted turbo spin-echo sections. The distribution of the variables was determined using the Kolmogorov-Smirnov test. The independent-samples t test and chi-square test were used to analyze quantitative independent data. The Fisher exact test was used when the conditions appropriate for the chi-square test were not met.
Results:
The mean femoral anteversion was higher in the patellar dislocation group, with a statistically significant difference (20.1 ± 3.8 vs 11.5 ± 1.8; P = .0001). The mean STT was significantly greater in the patellar dislocation group (41.3 ± 7.6 vs 35.2 ± 3.1; P = .0002). The mean ITT values were comparable between the groups (22.7 ± 2.8 vs 23.7 ± 2.3; P = .14).
Conclusion:
Our results indicate that increased femoral anteversion in RPD originates from the supratrochanteric region of the femur. Future large-scale studies, specifically focusing on the relationship between femoral anatomic variables and patellar instability, could yield significant insights into this matter.
Recurrent patellar dislocation (RPD) is a condition associated with the broader concept of patellar instability, which is primarily observed in adolescent patients.6,8 Female adolscents aged 10 to 17 appear to be the group with the highest risk.3,11 Despite the identification of factors such as alterations in patellar height, trochlear dysplasia, and the rotational malalignment of both the femur (increased anteversion) and the tibia (lateralization of tibial tubercule) as important factors in the causation of RPD, the comprehensive etiology of this condition remains insufficiently delineated.7,14,17
Recently, the influence of femoral axial malalignment on the etiology of various hip and knee pathologies garnered increased interest. Studies have established a correlation between increased femoral torsion and a range of conditions, including femoroacetabular impingement, anterior cruciate ligament injuries, and patellofemoral pain. 19 Further studies have explored whether the specific location of the femoral torsion, supratrochanteric or diaphyseal, affects its association with these clinical presentations.1,10,12,13,17,18 Currently, there is no consensus on which location of the femoral torsion has a greater effect on the etiology of patellar instability.
In this study, we aimed to investigate the effect of supratrochanteric and diaphyseal femoral torsion on the etiology of RPD. Our hypothesis posits that femoral axial malalignment originating from the supratrochanteric region poses a higher risk for patellar instability than malalignment originating from the infratrochanteric region.
Methods
Patient Selection
This retrospective age-matched case-control study was performed at the sports surgery department of an orthopaedic surgery clinic within a tertiary care center, between January 2021 and December 2023. Ethical approval for the study was granted by the local ethics committee. All cases diagnosed with RPD during the specified period were reviewed.
The inclusion criteria included patients with RPD, described as ≥1 patellar dislocation event, without multienergy trauma, and patients aged <18 years with complete medical and radiologic records. The exclusion criteria encompassed a history of fracture in the affected extremity, leg-length discrepancy, incomplete medical or radiologic records, and previous diagnosis of slipped capital femoral epiphysis, Legg-Calvé-Perthes disease, or connective tissue disorders such as Marfan syndrome or Ehlers-Danlos syndrome, as well as generalized joint hypermobility, which was defined as a Beighton score >4. Patients in the control group were selected by screening individuals who underwent femoral magnetic resonance imaging (MRI) at the same center during the same period, with matching based on age. In patients aged <18 years, femoral neck angle variation between age groups has been well-documented; thus, age matching was performed by a range of ±1 year. 5 The control group, aged 12 to 18 years, had previously undergone bilateral femoral MRI scans for various reasons. Only patients without any history of patellar instability or related symptoms were included in the control group.
Starting in 2021, our center adopted a standardized protocol involving a whole-femur MRI to assess femoral torsion in patients presenting with patellar instability. This transition to MRI for evaluating torsional malalignment was motivated by its efficacy in providing detailed anatomic assessments while avoiding radiation exposure. 16
The study group: a total of 212 patients were initially screened for the study group, and 31 femurs of 22 patients who met the inclusion criteria were included in the final analysis. The control group included 28 patients (28 femurs) who had no history of patellar dislocation (Figure 1).

Flowchart of the patient enrollment process.
MRI Measurements
MRI measurements were conducted by 2 senior orthopaedic surgeons with >5 years in the specialty (A.H.Ç., Y.A.), 2 weeks apart, each blinded to the previous results. After confirmation of sufficient intraclass correlation (>0.8; good reliability), the mean values of each measurement were incorporated into the analyses.
MRI measurements were conducted across 3 distinct axial sections. For evaluations, T2-weighted turbo spin-echo sections were used. The first section was optimized for the sphericity of the femoral head, which involved drawing a line between the center of the circle placed on the femoral head to the center of the circle placed in the cervicobasilar junction at the femoral neck (first line). The second section was identified at the level where the lesser trochanter appeared most medially prominent, with a line drawn from the center of the femoral diaphysis to the apex of the lesser trochanter (second line). The third section was optimized to define the posterior condylar axis, which marks the most posterior aspect of the distal femoral articular surface (third line). The angular difference between the first and second lines was analyzed as the supratrochanteric torsion (STT) value, while the difference between the second and third lines was recorded as the infratrochanteric torsion (ITT) value (Figure 2). Femoral anteversion was analyzed as the angle between the first and third lines and was evaluated according to the methodology proposed by Fritz et al. 10

(A) T1-weighted axial image identifying the center of the femoral head. (B) T1-weighted axial image identifying the center of the femoral head and femoral neck axis. Line (1) leads from the center of the circle placed on the femoral head to the center of the circle at the cervicobasilar junction of the femoral neck. (C) T1-weighted axial image identifying the section where the lesser trochanter appears most medially prominent. Line (2) indicates the detection of the lesser trochanteric apex with the largest medial extension. The angle between lines (1) and (2) describes supratrochanteric torsion. (D) T1-weighted axial image identifying the posterior condylar axis, which marks the most posterior aspect of the distal femoral articular surface. Line (3) shows the femoral posterior condylar axis. The angle between lines (2) and (3) describes infratrochanteric torsion.
Statistical Analysis
The mean, standard deviation, median lowest, median highest, frequency, and ratio values were used for the descriptive statistics of the data. The distribution of the variables was determined using the Kolmogorov-Smirnov test. One-year age difference between groups was considered acceptable, and statistical comparisons were performed accordingly. The independent-samples t test and chi-square test were used to analyze quantitative independent data. The Fisher exact test was used when the conditions appropriate for the chi-square test were not met. The SPSS Version 22.0 statistical program (IBM Corp) was used to perform all analyses. With a power of 80%, α level of .05, and 95% CI, the number of patients needed was calculated as 16 per group.
Results
This study investigated data from 22 patients (31 femurs) with dislocation history and 28 control group patients with no dislocation history. The demographic characteristics were similar between the groups (Table 1). The mean number of dislocations was 2.5 in the patellar dislocation group (range, 1-5).
Demographic Characteristics a

Data are presented as mean ± SD or n (%).
The mean femoral anteversion was greater in the patellar dislocation group (20.1 ± 3.8 vs 11.5 ± 1.8; P = .0001) (Table 2). The mean STT was significantly greater in the patellar dislocation group (41.3 ± 7.6 vs 35.2 ± 3.1; P = .0002). The mean ITT values were similar between the groups (22.7 ± 2.8 vs 23.7 ± 2.3; P = .14) (Figure 3).
Comparison of Femoral Anteversion, STT, and ITT Between Groups a

Data are presented as mean ± SD (range).FA, femoral anteversion; ITT, infratrochanteric torsion; STT, supratrochanteric torsion. P values compare differences between groups; P < .05 indicates statistical significance.
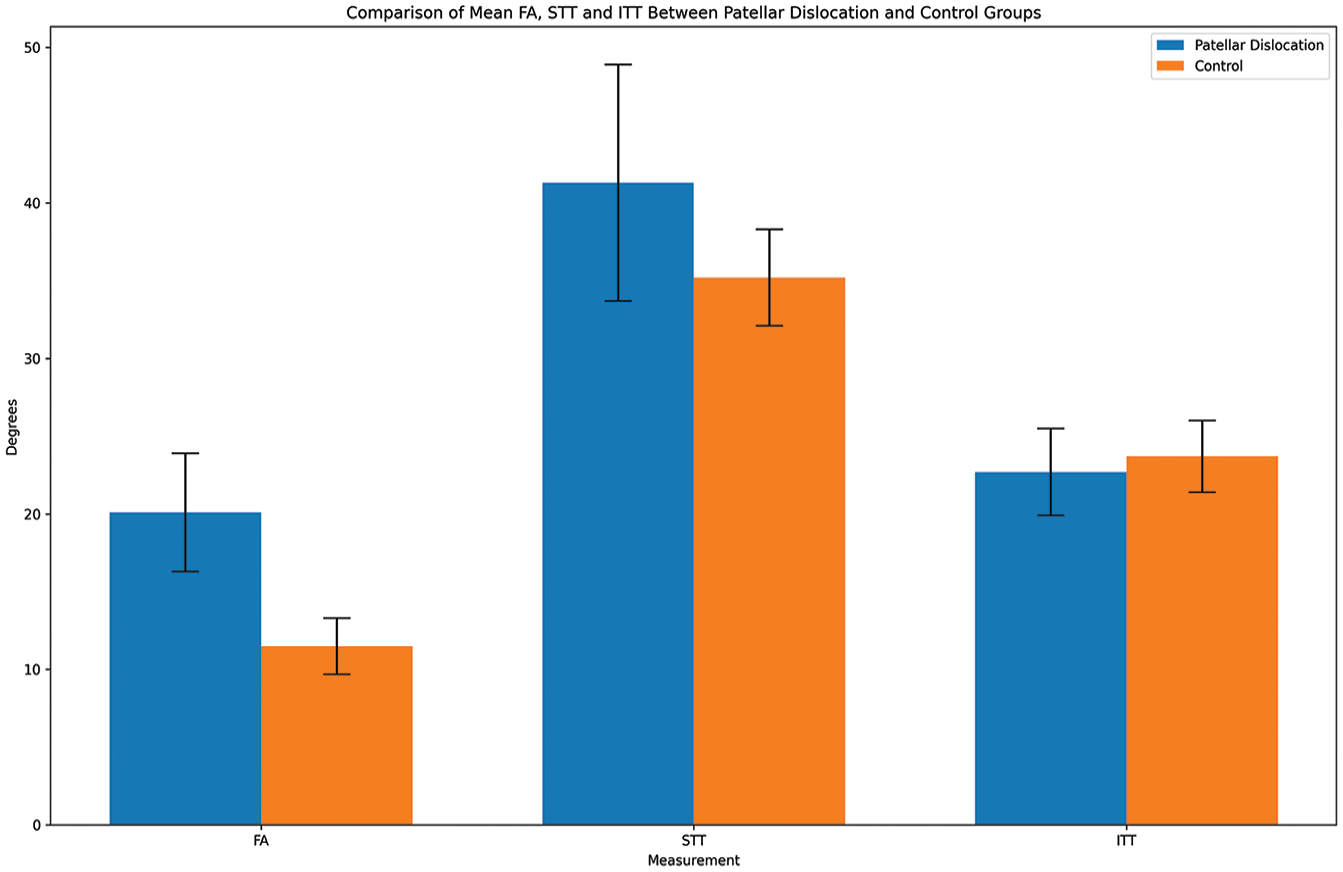
The patellar dislocation group had high femoral anteversion (FA) and supratrochanteric torsion (STT), but no infratrochanteric torsion (ITT). There was a high association between femoral anteversion and high supratrochanteric torsion within the patellar dislocation group.
In the patellar dislocation group, there was significantly higher femoral anteversion and STT. In contrast, the patellar dislocation group exhibited no significant ITT compared with controls (Table 2 and Figure 3).
Discussion
The most significant finding was that increased femoral torsion originated from the supratrochanteric (41.3 ± 7.6 vs 35.2 ± 3.1; P < .05) region of the femur, rather than from the infratrochanteric (22.7 ± 2.8 vs 23.7 ± 2.3; P = .14) region or the distal femur when compared with normal femoral anteversion.
The study by Seitlinger et al, 18 which initiated discussions regarding the anatomic site of torsional malalignment, had a notable effect; however, the broad age range of participants, spanning from 11 to 65 years old, is a limitation to consider. The study showed that femoral anteversion increases by approximately 1.5° per year, particularly in adolescents. 5 Additionally, Archibald et al 2 stated that the torsional increase of the femur is slightly more related to the femoral neck than to the femoral shaft. In our study, we felt that femoral anteversion decreases with age by matching the control and study groups within the typical age range for femoral torsional abnormalities. We believe this approach enhanced the statistical reliability of the femoral anteversion angle measurements, which are known to vary with age.
Determining the anatomic site of the rotational deformity in the femur is critical to the treatment plan and clinical outcomes.4,9 Jia et al 15 reported better results in patients having femoral torsion above the lesser trochanter in the treatment of RPD, although corrective osteotomies were performed distal to the femur regardless of the anatomic site of torsional malalignment. Our results suggested that the torsional malalignment in patients with RPD originated from supratrochanteric region rather than the infratrochanteric region. This raises the question of whether performing the osteotomy at this level eliminates the need for different soft tissue interventions or if the osteotomy level should be more proximal rather than distal. These results may inform future research comparing distal and proximal femoral derotation osteotomies in patients with RPD.
Although the importance of femoral torsion in RPD has been previously established, the exact location within the femur remained unclear, with the exception of the findings presented by Seitlinger et al. 18 However, Fritz et al 10 demonstrated that ITT or STT in femoroacetabular impingement may influence the treatment. The current study agrees with this for RPD.
Xu et al 20 studied segmental femoral torsion in patients with the RPD and concluded that midfemoral torsional malalignment was more correlated with RPD. While one of the limitations in the study by Xu et al was to pool patients from a broader range of age groups, their study reported important data on this debatable subject. Although the results of the current study appear to contradict those of Xu et al, we believe 2 key issues merit further investigation. First, torsional malalignment characteristics may vary across cohorts of different ethnic origins. Second, potential differences between the growing skeleton and the fully matured skeleton could influence these findings. Future studies focusing on more specific subgroups and homogeneous patient populations that can provide clearer answers to these questions would be valuable in this regard.
Limitations
This study has several limitations. First, it was retrospective and included a relatively small patient cohort, which could have potentially biased the results. Second, the absence of data on other anatomic variables such as trochlear and tibial morphology, as well as the lack of matching for height and skeletal maturity, may have introduced selection bias. Although additional patellofemoral measurements such as tibial tuberosity–trochlear groove distance, Quadriceps angle (Q-angle), and sulcus angle were reviewed during patient screening, they were not included in the analysis, as the study focused specifically on the segmental origin of femoral torsion.
Conclusion
Our results indicate that increased femoral anteversion in RPD originates from the supratrochanteric region of the femur. Future large-scale studies, specifically focusing on the relationship between femoral anatomic variables and patellar instability, could yield significant insights into this matter.
Footnotes
Correction (July 2025):
This article has been updated to correct the affiliation for Baris Kocaoglu.
Final revision submitted April 8, 2025; accepted May 1, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the local ethics committee (approval No. ESH/BAEK 2024/31).