
Abstract
Background:
Qualitative studies have explored changes in Tc-99m hydroxymethylene diphosphonate (HDP) uptake on single-photon emission computed tomography and computed tomography (SPECT/CT) as a result of offloading after medial opening-wedge high tibial osteotomy (MOWHTO) in patients with medial compartment knee osteoarthritis. However, whether changes in the Tc-99m HDP uptake on SPECT/CT reflect the degree of clinical improvement in postoperative outcomes, especially when using minimal clinically important differences (MCIDs), has not been investigated.
Purpose:
To investigate the association between changes in Tc-99m HDP uptake on SPECT/CT and MCID-based improvement on the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score in patients who underwent MOWHTO.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The study included 35 knees in 31 patients who underwent MOWHTO. SPECT/CT was performed preoperatively and 3 years postoperatively with clinical and radiological assessments. On SPECT/CT, the knee joint was divided into 10 regions, and the radiotracer uptake amount of each region was divided by the uptake amount of the reference zone. Patients were divided into 2 groups based on whether they achieved the MCID of 16.1 points on the WOMAC at 3 years postoperatively, and changes in uptake amount on SPECT/CT were compared between the groups.
Results:
At 3 years postoperatively, 22 patients achieved the MCID on the WOMAC (62.9%; above-MCID group) and 13 patients did not (37.1%; below-MCID group). In the above-MCID group, significant improvement was observed in the WOMAC after MOWHTO (from 55.8 to 19.6; P < .05); however, significant improvement was not observed in the below-MCID group (from 38.8 to 32.3; P = .100). Based on mean change of uptake on SPECT/CT in each region, the above-MCID group showed significantly greater reduction of uptake on SPECT/CT than the below-MCID group in the femoral anteromedial compartment (P = .004), tibial anteromedial compartment (P = .009), and tibial anterolateral compartment (P = .031).
Conclusion:
Reduction in radiotracer uptake on SPECT/CT of the knee joint reflected clinical improvement in patient-reported outcomes following MOWHTO.
For relatively young patients who have medial compartment osteoarthritis (OA) with varus knee deformity, medial opening-wedge high tibial osteotomy (MOWHTO) is an accepted treatment method because knee pain is reduced and satisfactory outcomes are achieved by offloading the medial compartment of the knee joint. 1,27,31 In addition, patients undergoing this treatment can expect a delay in the progression of degenerative OA and recovery in the damaged area of the medial compartment of the knee joint. 15,29
Tc-99m hydroxymethylene diphosphonate (HDP) single-photon emission computerized tomography and computerized tomography (SPECT/CT) is a method frequently used to determine the degree of progression and clinical symptoms of degenerative knee OA, and its use is gradually increasing. 8 –10,14,18,20,24,25 Because MOWHTO is a treatment to reduce loading of the medial compartment of the knee joint, SPECT/CT is an appropriate method to show the change in OA severity after offloading. Although the radiotracer uptake on SPECT/CT has been shown to decrease after MOWHTO 23 in qualitative studies, whether the degree of postoperative clinical improvement and the degree of radiotracer uptake are correlated has not been investigated.
In general, patient-reported outcome measures are useful for investigating clinical improvement after orthopaedic surgery, 6,22 and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score is a popular and well-proven method for assessing outcomes after knee surgery such as MOWHTO. 26,30 A concept recently used to evaluate outcomes after orthopaedic surgery is the assessment of the minimal clinically important difference (MCID) of a patient-reported outcome measure. 2,13 This is the smallest change in outcome in which the patient can recognize the benefit of a certain treatment. As clinical results after MOWHTO may vary by individual, 12 the MCID has attracted attention because the results above a clinically meaningful threshold are considered relevant for patients. 2,13 According to Kim et al, 16 the MCID of MOWHTO is 16.1 points for the total WOMAC score. Specifically, patients report that their knee OA symptoms and function improve with MOWHTO only if their postoperative total WOMAC score is at least 16.1 points better than the preoperative total.
In the current study, we analyzed whether the degree of patient improvement after MOWHTO can be objectively evaluated using SPECT/CT. We investigated the association between changes in Tc-99m HDP uptake on SPECT/CT and MCID-based improvement on the WOMAC score after MOWHTO.
Methods
The protocol for this retrospective study was approved by the institutional review board of our hospital. Between April 2016 and November 2017, a total of 61 MOWHTOs were performed in 56 patients by a single surgeon (Y.I.) at a single institute. Indications for MOWHTO were age <65 years, isolated symptomatic medial compartment knee OA and varus knee alignment (hip-knee-ankle axis, varus 0°-15°), no inflammatory arthritis, flexion contracture <15°, knee range of motion >120°, no joint instability, and no history of knee joint infection. 17 Preoperative knee magnetic resonance imaging was routinely performed to confirm the status of the tibiofemoral and patellofemoral joints of the knee. All patients underwent hardware removal operation at 2 years after MOWHTO. Plate removal was performed to complete bone remodeling and prevent hardware breakage for the convenience of arthroplasty that might be performed in the future. Our clinical course included SPECT/CT examinations preoperatively and 3 years after MOWHTO. Exclusion criteria for the study were inflammatory arthritis, traumatic OA, osteonecrosis, lateral compartment OA, patellofemoral OA, severe obesity (body mass index >40), or loss of follow-up at 3 years after surgery.
Among the 61 knees, 26 were excluded for the following reasons: missing preoperative WOMAC score (n = 1), no preoperative SPECT/CT raw data (n = 3), refusal to undergo 3-year follow-up SPECT/CT (n = 20), and 3-year follow-up SPECT/CT examination without hardware removal (n = 2). The final study cohort included 35 knees (31 patients), which were divided into 2 groups based on an MCID threshold of 16.1 points in total WOMAC score according to Kim et al 16 : above-MCID group (n = 22 knees, 62.9%) and below-MCID group (n = 13 knees, 37.1%). Figure 1 outlines the patient inclusion process.

Flowchart of patient inclusion process in the study. MCID, minimal clinically important difference; MOWHTO, medial opening-wedge high tibial osteotomy; SPECT/CT, single-photon emission computed tomography and computed tomography; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Surgical Procedure and Rehabilitation
Preoperatively, every patient underwent full-length lower extremity radiographs while standing to measure the correction angle. The correction angle for MOWHTO was determined using 2 lines with the Dugdale method. 5,21 Line 1 is drawn from the center of the femoral head to 62.5% of the width of proximal end of the tibia, which is the Fujisawa point, and line 2 is drawn from the center of the ankle joint to the Fujisawa point. 5 The angle formed by these 2 lines is the Dugdale correction angle. Arthroscopic examination of the knee was routinely performed before HTO, and meniscectomy was conducted if needed. MOWHTO was performed using the biplanar osteotomy method. 11,28 The electrocautery cable technique was used intraoperatively to confirm that the calibrated weightbearing line passed the Fujisawa point. A locking plate (Tomofix; Synthes) and screws were used to fix the osteotomy site after achieving the preoperatively planned correction angle. We calculated that a 1-mm opening of the osteotomy site corresponded to 1° of correction, and we analyzed if the planned correction angle was suitable under an image intensifier using the intraoperative cable technique before plate fixation. 11
The same rehabilitation program was used for all patients after surgery. From day 1 after surgery, knee range of motion exercise was initiated using a continuous passive motion machine starting from 60° of flexion to 140° in increments of 10° per day. Weightbearing was prohibited until 4 weeks after surgery, and after 2 weeks of walking on crutches, full weightbearing was allowed from 6 weeks after surgery.
Outcome Measures
The following factors were compared between the above- and below-MCID groups: age, sex, body mass index, and operation side (right or left). Radiographic variables evaluated included Kellgren-Lawrence grade, pre- and postoperative hip-knee-ankle axis, the weightbearing line ratio (line connecting the hip and ankle center), and tibial sagittal slope.
WOMAC scores were obtained preoperatively and 3 years postoperatively for all patients. The WOMAC score is a proven 24-item disease-specific questionnaire widely used to evaluate clinical outcomes after knee surgery. The WOMAC consists of 3 subscales: pain (5 items), stiffness (2 items), and function (17 items). Each item has 5 possible responses and a score of 0 to 4 for each response, for a total of 20 points for the pain subscale, 8 for the stiffness subscale, and 68 for the functional subscale; thus, the total score ranges from 0 to 96.
SPECT/CT evaluation was performed twice in each patient—preoperatively and 3 years postoperatively. All scans were performed using a hybrid SPECT/CT scanner (Symbia T6; Siemens). Planar blood pool imaging was performed at 1 minute after intravenous injection of approximately 740 MBq of Tc-99m HDP. Two hours after injection of radiotracer, planar images of both knees were acquired and immediately followed by SPECT/CT. CT images were acquired using the following parameters: 130 kVp and 2-mm slice thickness. The SPECT setting was peak energy at 140 keV with a 15% window. SPECT image reconstructions were performed using an iterative ordered subset expectation maximization algorithm (12 iterations, 16 subsets).
The radiotracer uptake was assessed in SPECT/CT images with a commercial fusion software system (Mirada Medical). SPECT/CT images were centrally and repeatedly reviewed by a nuclear medicine physician (H.Y.) blinded to the patient’s identity and clinicopathological results. Cuboid volumes of interest (VOIs) were created at specific sites that divided the knee joint into 10 regions.
The femur was divided into 4 regions: anteromedial, anterolateral, posteromedial, and posterolateral. The reference line for dividing the femur medially and laterally was a line connecting the deepest part of the trochlear groove and the center of the intercondylar notch. The reference line for dividing the femur anteriorly and posteriorly was the midpoint of the outermost anterior cortex and the outermost posterior cortex of the femur on the CT axial image. The tibia was also divided into 4 regions based on the bisecting point of the line connecting the protruding end of the anterior and posterior cortices and the midpoint of the medial and lateral cortical margins. The 4 femoral and 4 tibial regions were outlined as 1 cm–deep cuboid shapes containing the subchondral area of the knee joint (Figure 2, A and B).

Target regions for analysis of radiotracer uptake on single-photon emission computed tomography and computed tomography of a 47-year-old woman’s left knee: (A-D) coronal, sagittal, axial (distal femur), and axial (proximal tibia). The cross-sectional views at the positions of lines a-a′ and b-b′ in panel B are shown in panels C and D.
In addition, the entire patella was analyzed as a separate region (Figure 2, B and C); however, the tibial osteotomy site was considered a region ranging 2 cm distal from the tibial plateau to 4 cm in length, with a width that included the medial and lateral cortices of the tibia in a rectangular shape (violet region in Figure 2, A and B). For semiquantitative image analysis, a cylindrical VOI 1 cm in diameter and 2 cm in length was placed in the distal femoral shaft intramedullary area as a reference zone (ie, the distal end of the reference zone VOI was approximately 2 cm proximal from the distal femoral cortex; blue region in Figure 2B). The uptake ratio on SPECT/CT for each target region was defined as the maximum radiotracer uptake value from the target VOI region divided by the mean uptake value from the femoral shaft reference VOI.
The radiotracer uptake on SPECT/CT in each target zone was semiquantitatively calculated preoperatively and 3 years postoperatively in the 2 groups. The results between the groups were compared and analyzed by calculating the difference in the measurements before and 3 years after MOWHTO.
Statistical Analysis
The Student t test or the Wilcoxon signed-rank test was used to analyze continuous variables. The comparison of categorical variables of patient characteristics between the groups was assessed using the chi-square test or Fisher exact test. The paired t test was used to compare pre- and postoperative WOMAC scores and the uptake amount on SPECT/CT in each region. The Mann-Whitney U test was used to compare uptake differences on SPECT/CT in each target region of the above- and below-MCID groups in the total WOMAC score.
All statistical analyses were performed using SPSS (Version 24.0; IBM). P < .05 was considered statistically significant.
Results
Significant differences in patient demographics were not observed between the groups. Of the total 35 cases involved in study, 4 were male and 31 were female, and the proportion of female patients was 88.6%. Surgical factors, such as Kellgren-Lawrence grade, pre- and postoperative hip-knee-ankle axis and weightbearing line ratio, tibial sagittal slope, and surgical correction angle, were not significantly different between the groups (Table 1).
Patient Characteristics a
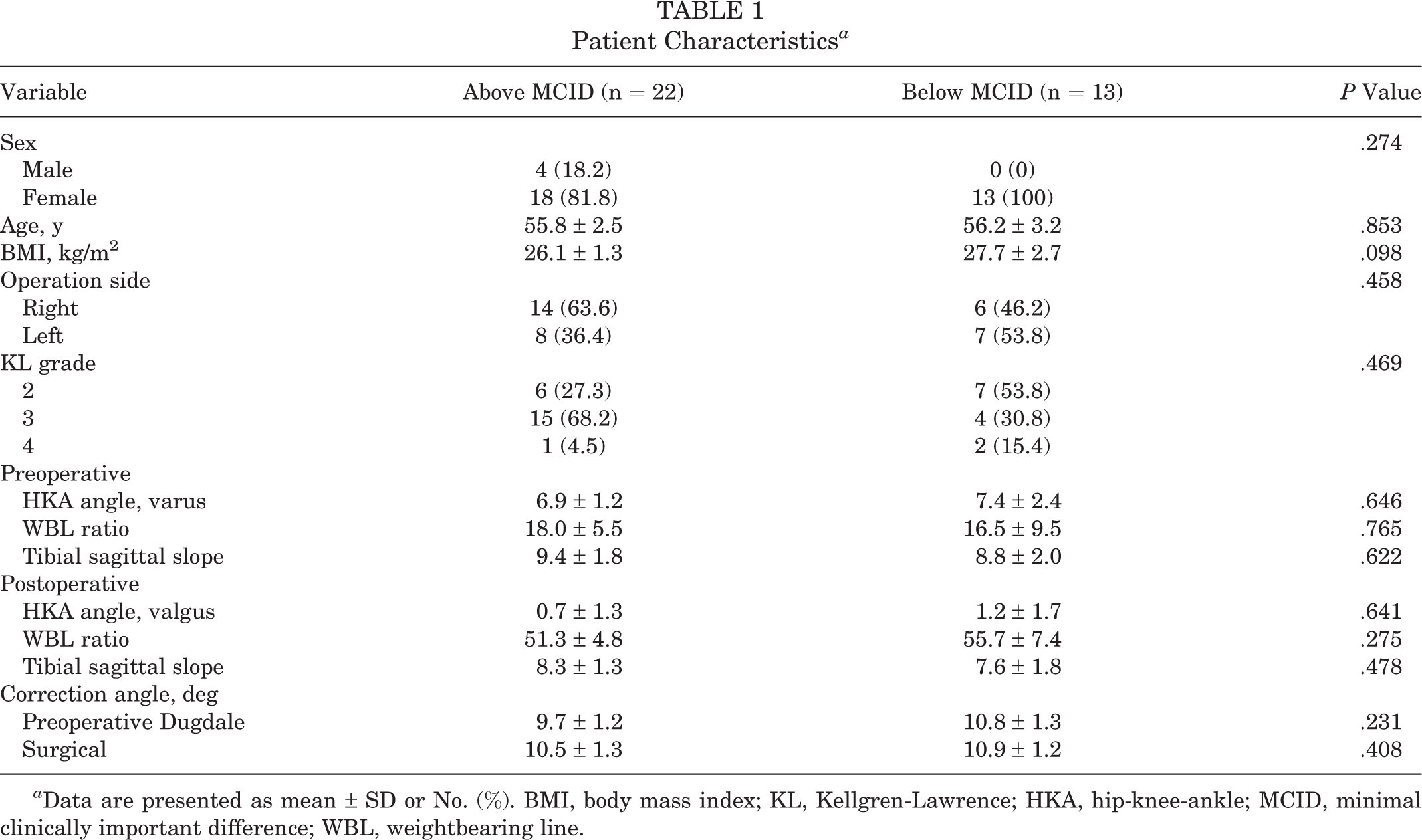
a Data are presented as mean ± SD or No. (%). BMI, body mass index; KL, Kellgren-Lawrence; HKA, hip-knee-ankle; MCID, minimal clinically important difference; WBL, weightbearing line.
WOMAC Scores
Significantly improved outcomes were observed on the total WOMAC score and every subscore in the overall cohort of 35 patients (P < .001 for all) (Table 2). When compared with the below-MCID group, the above-MCID group had significantly higher preoperative WOMAC scores (P < .05 for all) and significantly lower 3-year scores, with the exception of the WOMAC stiffness subscore. Within the above-MCID group, significant pre- to postoperative improvement was observed on all WOMAC scores (P < .05 for all), but only the WOMAC pain and function scores showed postoperative improvement in the below-MCID group.
WOMAC Scores Overall and Between the Study Groups a

a Data are reported as mean ± SD. Bold P values indicate statistically significant difference between and within groups (P < .05). MCID, minimal clinically important difference; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
bP value: pre- vs postoperative.
cP value: above vs below MCID.
For the 20 patients who were not included in the study because of refusal to take the follow-up SPECT/CT, all postoperative WOMAC scores improved significantly as compared with preoperative scores (total WOMAC, 51.5 to 30.6; WOMAC pain, 11.7 to 3.8; WOMAC stiffness, 5.1 to 2.0; WOMAC function, 34.7 to 15.1; P < .001 for all).
Uptake Differences on SPECT/CT
In 19 of the 22 patients in the above-MCID group, the radiotracer uptake of the medial compartment before MOWHTO on SPECT/CT was decreased at the 3-year postoperative examination, as confirmed on 3-dimensional reconstruction (Figure 3).

(A) Pre- and (B) postoperative 3-year single-photon emission computed tomography and computed tomography images of a 48-year-old woman who underwent MOWHTO. The amount of uptake decreased in the subchondral region of the medial compartment of the right knee joint after MOWHTO in 3-dimensional reconstruction and maximal-intensity projection images. MOWHTO, medial opening-wedge high tibial osteotomy.
Comparison of uptake differences on SPECT/CT in each target region showed that the above-MCID group had significantly greater pre- to postoperative changes in radiotracer uptake in the femoral anteromedial compartment (mean ± SD, 4.8 ± 3.4 vs 0.3 ± 2.1; P = .004), tibial anteromedial compartment (7.9 ± 4.4 vs 1.5 ± 2.8; P = .009), and tibial anterolateral compartment (1.1 ± 1.6 vs 0.3 ± 1.2; P = .031) as compared with the below-MCID group (Table 3).
Major complications needing additional surgery were not observed, except plate removal during the 3-year follow-up period in both groups.
Uptake Differences on SPECT/CT in Each Target Region Between the Study Groups a

a The relative uptake value was calculated as the absolute value of uptake for the target area divided by the femoral shaft reference zone. Data are presented as mean ± SD. Bold P values indicate statistically significant difference between groups (P < .05). MCID, minimal clinically important difference; SPECT/CT, single-photon emission computed tomography and computed tomography.
Discussion
The most important finding in the present study was that patients who achieved the MCID in WOMAC scores at 3 years after MOWHTO showed greater changes in the radiotracer uptake on SPECT/CT—specifically, greater reduction in the femoral anteromedial compartment, tibial anteromedial compartment, and tibial anterolateral compartment. Based on this result, SPECT/CT was considered to reflect clinical improvement after MOWHTO. Conversely, significant changes on SPECT/CT were not observed in patients who did not experience clinical improvement after MOWHTO (ie, those who did not achieve the MCID).
SPECT/CT is advantageous because the results can be understood visually; thus, determining the patient’s satisfaction after surgery and explaining the results is not complicated. In this study, SPECT/CT reflected improvements in WOMAC score, which might have value in identifying patients who do not do well after MOWHTO.
Mucha et al 23 investigated changes in uptake on SPECT/CT in patients who underwent MOWHTO and reported significantly decreased radiotracer uptake 12 and 24 months postoperatively in the medial compartment of the knee as well as significant improvement of WOMAC scores. However, in the present study, several patients in the below-MCID group showed increased radiotracer uptake or almost no interval change in the examination 3 years after MOWHTO, thereby indicating that not every patient showed a good outcome after surgery. The reasons for the contradictory results are probably due to the larger sample size in the present study (22 knees in Mucha et al 23 vs 35 knees in the current study) resulting in various findings or to the different follow-up periods after surgery (2 years in Mucha et al 23 vs 3 years in the current study) causing differences in radiotracer uptake attributed to OA progression.
The patients in the above-MCID group after MOWHTO had significantly higher preoperative WOMAC scores than patients in the below-MCID group and showed much better results after surgery except for stiffness. This finding was similar to other studies, 3,4 which might be due to the increased capacity for clinically meaningful improvement in patients with low preoperative WOMAC scores. 16 As such, the surgical effect may be better in patients who complain of more severe discomfort before surgery.
On preoperative SPECT/CT, radiotracer uptake was significantly higher in the anteromedial tibia in the above-MCID group than in the below-MCID group, which appears to reflect the high preoperative WOMAC score in the above-MCID group. At 3 years postoperatively, the amount of change in radiotracer uptake was significantly greater in the above-MCID group than in the below-MCID group, similar to the change in WOMAC score in the above-MCID group. However, although the difference in preoperative uptake on SPECT/CT between the groups was not observed in the anteromedial femur and anterolateral tibia, a significant change was observed in the above-MCID group 3 years postoperatively, indicating that clinical improvement results are associated with changes on SPECT/CT.
Limitations
The present study had several limitations. First, given the limitation of the SPECT/CT analysis program used, the index volume of the target regions was drawn in cuboid shapes. Although this VOI included the joint surface and subchondral area that were necessary for analysis, a limitation in accurately dividing the regions existed because the area was divided into a cuboid shape. A more accurate analysis could have been possible if the target region was drawn more precisely in 3 dimensions. Second, this was a retrospective cohort study in which 2 groups were compared; however, the data were obtained only from a single institute and a single surgeon, which could have caused a selection bias. More meaningful results might have been obtained if data from more institutes were analyzed.
The small sample size was another limitation. Among the patients who underwent MOWHTO during the study period, the final number enrolled in this study was insufficient because many could not be included for various reasons, such as refusal to undergo SPECT/CT. Therefore, the data should be analyzed using a nonparametric test. If fewer patients had refused to undergo SPECT/CT follow-up examinations, more patients would have been included in the study; thus, more precise results might have been obtained. A fourth limitation was that most of the patients were female (88.6%). However, all patients were of Asian ethnicity, and the prevalence, incidence, and severity of OA for Asians are known to be higher in women than men. 19
Why clinically improved cases had a significantly decreased uptake on SPECT/CT in the anterolateral compartment of the tibia 3 years postoperatively could not be explained. In the case of MOWHTO, only the improvement of the medial compartment can be expected because the operation is performed on medial compartment OA, although a significant improvement in the tibial anterolateral compartment for the above-MCID group was observed in SPECT/CT analysis. In addition, this treatment might lead to overloading the lateral compartment because the weightbearing line is shifted from the medial to the lateral compartment after MOWHTO, which induces a weightbearing increase on the lateral side of the knee joint and worsens the radiotracer uptake of the area. Yet, the results showed the opposite findings at the tibial anterolateral compartment. Hernigou et al 7 reported the risk of proximal tibial osteotomy overcorrection, which causes progression of lateral compartment OA. Therefore, the correction angle performed for the clinically improved cases in the present study was appropriate; however, radiotracer uptake improvement in the anterolateral compartment of the tibia cannot be explained. An increase of tibial slope is common after MOWHTO and is believed to have an effect, but in our study, tibial slope was not increased after HTO in either group. Further studies are needed to determine why uptake improved in the tibial anterolateral compartment on SPECT/CT.
Conclusion
This study analyzed changes in uptake on SPECT/CT of the knee joint after dividing patients into 2 groups based on the MCID for the total WOMAC score. Results showed that reduction in radiotracer uptake reflected clinical improvement in patient-reported outcomes after MOWHTO.
Footnotes
Final revision submitted May 24, 2022; accepted June 6, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul St Mary’s Hospital, The Catholic University of Korea (No. KC20RISI0903).