
Abstract
Background:
Neurovascular injury is a serious complication after opening-wedge high tibial osteotomy (OWHTO).
Purpose:
To evaluate (1) how neurovascular injuries during fixation can be prevented and (2) whether a lateral hinge–directed posteromedial fixation system provides comparable neurovascular safety during OWHTO to conventional and custom-made locking plate systems.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 275 knees that underwent OWHTO from March 2014 to May 2018. The knees were divided into 4 groups based on the type of fixation system used: (1) lateral hinge–directed system (LCfit HTO; LCfit group), (2) TDM decisive wedge locking plate (TDM group), (3) OhtoFix anatomic locking metal block plate (OhtoFix group), and (4) TomoFix titanium locking plate (TomoFix group). Using postoperative computed tomography, the following variables among the groups were compared: screw insertion angle relative to the tibia posterior cortex in the axial plane, length, proximity to neurovascular structures, and safety angle of screw fixation (angle between the most proximal posterior screw insertion line and a line tangent to the popliteal artery from the screw hole). Radiological and clinical outcomes were also compared between groups.
Results:
The screw angle was significantly smaller and the distance from neurovascular structures to the screw extension line was significantly farther in the LCfit group compared with the other 3 groups (P < .001 for both). The safety angle was also wider in the LCfit group than in the other groups (P < .001). There were no significant differences in radiologic or clinical outcomes between the groups during follow-up.
Conclusion:
The distance from the neurovascular structures to the screw extension line was significantly farther, and the safety angle was also significantly wider with the laterally directed posteromedial plate system compared with the other systems. There were no neurovascular injuries in any group or significant differences in clinical outcomes or radiological parameters between the LCfit and the other locking plate systems.
Opening-wedge high tibial osteotomy (OWHTO) is commonly performed for medial compartment osteoarthritis and regarded as an effective treatment in active patients. 1,7,16,17 However, it is also associated with a number of complications, such as infection, metal irritation, deep vein thrombosis, secondary loss of reduction, lateral hinge fracture, delayed union or nonunion, compartment syndrome, and neurovascular injuries. 3,15,21,22 In particular, compartment syndrome, necrosis of the tibial head, and injuries of the popliteal neurovascular bundle are major complications that can cause severe problems. 8 Neurovascular injuries after medial opening-wedge osteotomy have been noted in case reports, 2,5,19 indicating that catastrophic neurovascular injuries can occur during OWHTO.
The danger to the neurovascular structures during OWHTO has not yet been determined. Damage can occur during osteotomy or plate fixation. To prevent neurovascular injuries during osteotomy, several methods have been introduced. 10,14 For fixation, conventional systems are usually positioned on the anteromedial side, and screws are directed to the posterolateral side. Neurovascular bundles are predicted to be located on the posterior side near screws. 13,20 Most of the modern high tibial osteotomy systems (eg, TDM decisive wedge locking plate [Trademedics], OhtoFix anatomic locking metal block plate [Ohtomedical], and TomoFix T-shaped conventional titanium locking plate [Synthes]) use unicortical locking fixation constructs. However, neurovascular injuries can also occur during drilling the screw holes. In addition, there are some situations that require bicortical fixation.
In addition, 2 bridges remain after fixation: One is the plate fixation area on the medial side, and the other is the cortical hinge on the lateral side. For stability after OWHTO, the lateral hinge should be intact to create a fulcrum, and the screws should be set in the direction of this area. 6,9 This can be helpful for the protection of neurovascular structures because laterally directed (ie, toward the lateral hinge) fixation can help avoid direct infiltration of neurovascular bundles. Previous studies have evaluated lateral hinge–directed fixation systems for OWHTO. 9,18,23 In our previous study, the lateral hinge–directed fixation system showed fixation configurations that have theoretical mechanical advantages over conventional anatomic locking plates. 11
The aims of this study were to evaluate (1) how neurovascular injuries during fixation can be prevented and (2) whether a lateral hinge–directed fixation system provides comparable neurovascular safety to conventional and custom-made locking plate systems. Our hypothesis was that laterally directed fixation would provide more safety to neurovascular structures than would posterolaterally directed fixation.
Methods
Patients
After receiving institutional review board approval for the study protocol, we retrospectively reviewed 316 knees that underwent OWHTO from March 2014 to May 2018. The study inclusion criteria were as follows: (1) medial unicompartmental osteoarthritis, (2) genu varus deformity of the lower limb, and (3) completed immediate postoperative computed tomography (CT). The exclusion criteria were as follows: (1) revision OWHTO (3 knees); (2) double osteotomy, including distal femoral osteotomy (7 knees); and (3) simultaneous ligament reconstruction that required concomitant sagittal plane modification (5 knees). After 15 knees were excluded, a total of 301 knees were included. Among them, the knees without completed serial radiological and clinical assessments over a postoperative period of at least 2 years were excluded. Ultimately, 275 knees were included (Figure 1).

Flowchart of patient enrollment. HTO, high tibial osteotomy; OWHTO, opening-wedge high tibial osteotomy.
The study patients were divided into 4 groups based on the type of fixation system used, as follows. Each plate had different fitting contours and locking screw directions.
LCfit group: Laterally directed hinge system with an inverted L-shaped plate anatomically contoured to the postcorrection tibia (LCfit HTO system; Corentec)
TDM group: TDM decisive wedge locking plate
OhtoFix group: OhtoFix anatomic locking metal block plate
TomoFix group: TomoFix titanium locking plate
These 4 fixation systems had been used sequentially in our practice. We used the TDM plate from March 2014 to March 2015, OhtoFix plate from April 2015 to May 2016, TomoFix plate from June 2016 to May 2018, and LCfit plate from February 2017 to May 2018.
Surgical Technique and Rehabilitation Protocol
All surgical procedures were performed by a single senior surgeon (Y.S.L.). The surgical procedures did not differ according to the fixation system used. An incision was made longitudinally 1 cm anterior to the posteromedial border of the tibia. The superior border of the pes anserinus was incised, and the superficial medial collateral ligament was mobilized from the tibia and released using a periosteal elevator. Under the C-arm image, a protective cutting system (Tradimedics and Corentec) was applied to the lateral cortical hinge located just below the tip of the fibular head. Osteotomy was performed from the medial to lateral side until it reached just 5 to 10 mm before the lateral cortex. 14 Next, the osteotomy site was distracted in accordance with the preoperative planning, and the plate was positioned at the central portion of each fragment, with best contouring with knees in 90° of flexion, if possible. After the plate was positioned, screw fixation was performed. The degree of distraction was adjusted to the most posterior side, and the gap ratio (anterior/posterior) was adjusted to around two-thirds ratio by compressing the anterior gap. 12
Isometric quadriceps exercises and continuous passive motion exercises were initiated on the first postoperative day. Partial weightbearing with crutches was permitted during the first 2 postoperative weeks, and full weightbearing as tolerated was permitted after postoperative week 2. Crutches were used 6 weeks postoperatively. Stair-climbing and sudden standing from the sitting position were prohibited during the first 3 months postoperatively, if possible. 18
Evaluations
All measurements were performed using INFINITT Version 5.0.9.2 (INFINITT). Preoperative magnetic resonance imaging (MRI) and postoperative CT scans without enhancements were performed with full extension of knees. CT scanning (SOMATOM Definition [Siemens]; MX8000, Brilliance 64, Brilliance iCT [Philips]) of the osteotomized knees was performed on the first or second postoperative day. Radiologic and clinical evaluations were performed at every visit to the outpatient clinic. The whole lower extremity, weightbearing anteroposterior (AP), and lateral radiographic views, and CT scans of all enrolled participants were analyzed.
Two observers (S.J.S. and H.W.J., both orthopaedic fellows) performed the quantitative evaluation, and interobserver and intraobserver reliability were assessed for all quantitative measurements. For intraobserver reliability, measurements were performed 2 times with a 6-week interval between.
Analysis of Neurovascular Safety
Using postoperative CT scans, the screw angle, length, proximity to neurovascular structures, and safety angle of screw fixation were evaluated and compared among the 4 groups.
The screw angle was measured from the proximal tibia using axial CT images at the most proximal screw level. A line crossing the proximal center screw of the plate was drawn, and a second line crossing the posterior cortex was drawn. The screw angle was measured between the 2 lines (Figure 2). Further, screw length was determined intraoperatively as the length of the proximal center screw because it indicated the longest length in most fixations (Figure 3). To assess neurovascular proximity, preoperative MRI scans were used to localize the neurovascular structures on CT images.

Measurement of screw angle on computed tomography scans by fixation system: (A) LCfit plate, (B) TDM plate, (C) OhtoFix plate, and (D) TomoFix plate. The angle was determined from the proximal center screw to the posterior cortical line.

Measurement of screw length on computed tomography scans by fixation system: (A) LCfit plate, (B) TDM plate, (C) OhtoFix plate, and (D) TomoFix plate. The screw length was determined as the length of the proximal center screw.
The neurovascular position was determined in the preoperative axial MRI scan that showed the closest position to the CT scan in which proximal screws were inserted. The popliteal artery was demarcated, and its diameter was measured. The distances from the posterior tibial cortex line (line a in Figure 4) and fibular medial cortex line (line b) to the popliteal artery were measured in the MRI scan. Subsequently, the popliteal artery was transferred to the axial CT image at the measured distance from the 2 landmarks. To evaluate safety during drilling for screw fixation, the distance from the neurovascular structures to the screw extension line was measured as the distance from a line crossing the most posterior screw to the localized neurovascular structure (Figure 5).

Synchronizing method of neurovascular structures from (A) MRI scan to (B) CT scan. a is the distance from the posterior tibial cortex line to the popliteal artery; and b is the distance from the fibular medial cortex line to the popliteal artery.

Measurement of the distance from neurovascular structure to the screw extension line on computed tomography (CT) scan by fixation system: (A) LCfit plate, (B) TDM plate, (C) OhtoFix plate, and (D) TomoFix plate. Inset images represent the preoperative axial magnetic resonance imaging scan that showed the closest position to the CT scan. The circle represents the popliteal artery.
The medial safe-zone angle (α1), dangerous zone angle (α2), and screw-insertion angle (β) were evaluated to determine how we can drill and insert screws safely during fixation (Figure 6). The most protruding spot of the anterior tibial cortex was used as a landmark because this angle should be addressed intraoperatively, even though it would be a rough estimation. A line from the most posterior screw insertion site to the most protruding spot of the anterior tibial cortex was drawn (line a), and a line perpendicular to this line (line b) was drawn. The medial safe zone angle (α1) was measured between line b and a line from the posterior screw insertion site to the medial border of the neurovascular structure. The dangerous zone angle (α2) was measured between a line from the posterior screw insertion site to the medial border of the neurovascular structure and a line from the posterior screw insertion site to the lateral border of the neurovascular structure. The screw insertion angle (β) was measured between line b and the line crossing the most posterior screw. Therefore, we calculated the safety angle by subtracting the sum of the medial safe zone angle (α1) and the dangerous zone angle (α2) from the screw insertion angle (β).

Measurement of the medial safe zone angle (α1), dangerous zone angle (α2) and screw insertion angle (β) by fixation system: (A) LCfit plate, (B) TDM plate, (C) OhtoFix plate, and (D) TomoFix plate. Inset images represent the preoperative axial MRI scan that showed the closest position to the computed tomography scan. Line a represents the line from the most posterior screw insertion site to the most protruding spot of the anterior tibial cortex, line b is a line perpendicular to line a, and the circle represents the popliteal artery.
Outcomes
Clinical and radiological findings were also evaluated and compared among the 4 groups. Clinical outcomes were evaluated by the preoperative and final follow-up American Knee Society Score (AKSS) and Western Ontario and McMaster Universities (WOMAC) scores. Postoperative complications were also assessed. Whole-leg weightbearing and plain standing lateral knee radiographs were used to analyze radiological outcomes. Changes in the hip-knee-ankle (HKA) angle, weightbearing line (WBL) ratio, and medial proximal tibial angle (MPTA) were compared to evaluate the correction loss in the coronal plane from whole-leg standing radiographs taken at 2 weeks postoperatively and at the final follow-up. Changes in the posterior tibial slope (PTS) were compared using plain standing lateral knee radiographs taken at 2 weeks postoperatively and at the final follow-up.
Statistical Analysis
The inter- and intraobserver reliability were assessed using the intraclass correlation coefficient (ICC). The normality tests for continuous variables were performed using the Shapiro-Wilk test. Using 1-way analysis of variance (ANOVA), the parameters of neurovascular safety and clinical and radiologic outcomes were compared among the 4 groups. If there was a difference between the 4 groups, the Scheffé test was used for post hoc analysis. To evaluate the changes in the HKA angle, WBL ratio, and PTS (quantitative parameters) from radiographs taken at 2 weeks postoperatively and at the final follow-up, the paired t test was performed. Statistical significance was set at P < .05. Data were analyzed using SPSS Version 28.0 (IBM).
A post hoc power analysis of the study was performed using G*power Version 3.1.9.7 with an effect size of 0.40, according to our result of CT analysis variables, and an alpha value of 0.05.
Results
Of the 275 knees, 87 (31.6%) were allocated to the LCfit group, 75 (27.3%) to the TDM group, 85 (30.9%) to the OhtoFix group, and 28 (10.2%) to the TomoFix group. There were no significant differences among the 4 groups in terms of preoperative demographic and radiologic data (Table 1).
Preoperative Demographic and Radiologic Data (N = 275 Knees) a
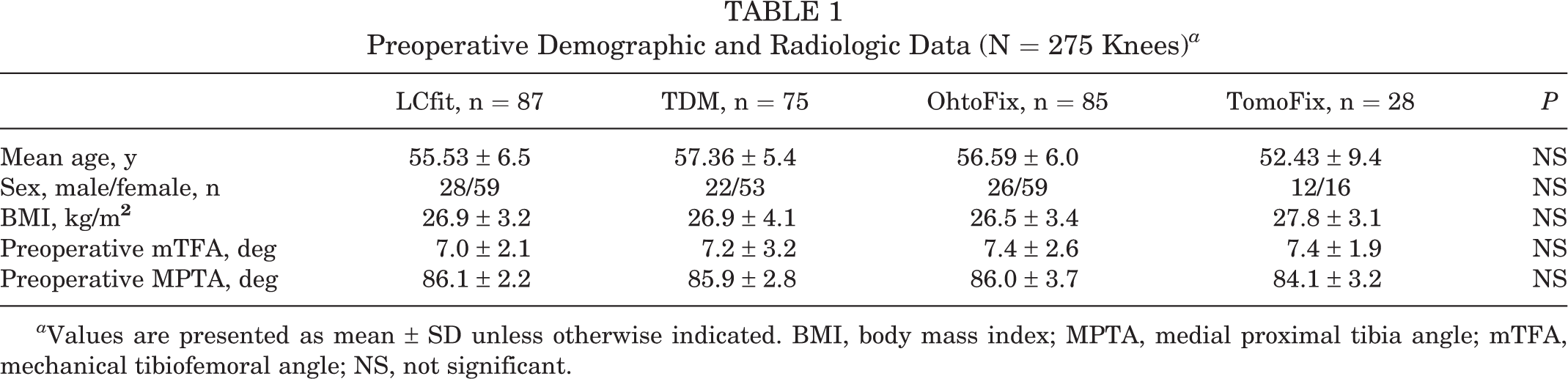
a Values are presented as mean ± SD unless otherwise indicated. BMI, body mass index; MPTA, medial proximal tibia angle; mTFA, mechanical tibiofemoral angle; NS, not significant.
The inter- and intraobserver reliability for the CT and MRI measurements were satisfactory, with mean ICC values of 0.87 (range, 0.85-0.89) and 0.89 (range 0.87-0.91), respectively. According to the post hoc power analysis, the statistical power of this study was 0.99.
Analysis of Neurovascular Safety
The results of 1-way ANOVA for the postoperative CT measurements related to neurovascular safety in the 4 groups are summarized in Table 2. The screw angle was significantly smaller in the LCfit group (30.1° ± 6.3°) versus the TDM (45.6° ± 9.4°), OhtoFix (48.5° ± 9.2°), and TomoFix (47.2° ± 7.5°) groups (P < .001). There were no significant differences in screw angle among the TDM, OhtoFix, and TomoFix groups. The screw length was longer in the LCfit (62.8 ± 5.6 mm) and TomoFix (61.3 ± 5.0 mm) groups than in the TDM (57.5 ± 5.0 mm) and OhtoFix (53.8 ± 5.3 mm) groups (P < .001). The distance from neurovascular structures to the screw extension line in the LCfit group (11.7 ± 4.7 mm) was significantly farther than that in the other groups (TDM: 6.0 ± 6.2 mm; OhtoFix: 3.6 ± 7.5 mm; TomoFix: 5.8 ± 4.2 mm; P < .001 for all). The safety angle was also wider in the LCfit group (11.3° ± 5.6°) than in the other 3 groups (TDM: 4.8° ± 7.2°; OhtoFix: 2.4° ± 5.4°; TomoFix: 5.1° ± 4.3°; P < .001 for all).
Postoperative Computed Tomography Analysis of the Neurovascular Safety a

a Values are presented as mean ± SD unless otherwise indicated. NS, not significant; NV, neurovascular structures.
b Numbers represent the corresponding groups.
c See Figure 6 for explanation of angles.
Outcomes
There were no significant differences in HKA, WBL ratio, MPTA, and PTS values between the 4 groups at 2 weeks postoperatively and the final follow-up. In addition, the changes in HKA, WBL, MPTA, and PTS values between these follow-ups were similar in all 4 groups (Table 3).
Comparison of Radiologic Outcomes Between Groups a

a Values are presented as mean ± SD. HKA, hip-knee-ankle; MPTA, medial proximal tibia angle; NS, not significant; PTS, posterior tibial slope; WBL, weightbearing line.
The clinical scores, including the AKSS and WOMAC scores, significantly improved postoperatively compared with the preoperative values. However, there were no significant differences in the final follow-up clinical scores (AKSS and WOMAC scores) among the 4 groups. No neurovascular injury or infection cases were observed in any group, and there was no significant difference in the incidence of hinge fracture among the 4 groups (Table 4).
Comparison of Clinical Outcomes and Complications Between Groups a

a Values are presented as mean ± SD or No. of patients (%). AKSS, American Knee Society Score; F, function; K, knee; NS, not significant; WOMAC, Western Ontario and McMaster Universities.
Discussion
The principal finding of this study was that the lateral hinge–directed posteromedial fixation system (LCfit) provided better neurovascular safety during plate fixation as evidenced by postoperative CT analysis. However, no neurovascular injury was observed in any of the 4 plate groups. Therefore, our hypotheses were partially validated only in terms of neurovascular safety.
Previous studies have reported various methods to prevent neurovascular injuries during OWHTO. 4,10 In this study, a protective cutting system was used during osteotomy to protect neurovascular structures during sawing of the bone. 14 However, neurovascular injuries can also occur during plate fixation. To the best of our knowledge, this is the first study to analyze the safety of neurovascular structures in relation to the fixation system position and the screw direction by synchronizing preoperative MRI scans with postoperative CT scans using measurements such as screw angle, distance from the neurovascular structure to screw extension line, and safety angle.
There are several concerns regarding fixation after OWHTO. First, the plate should be appropriately contoured and positioned at the central area of both proximal and distal fragments. 11 Second, screws should be headed toward hinge direction for the support of the thin lateral bridge. 9 In addition, the screws should be safe for the posterior neurovascular structures. Thus, screw insertion angle is an important consideration. The screw angle was significantly smaller in the LCfit group than in the other plate groups because of the posteromedial position. The smaller screw angle is related to the longer screw length in the LCfit group because the screw is directed from medial to lateral rather than anteromedial to posterolateral proximal tibia. These findings suggest that posteromedial plating with laterally directed screw fixation is safer for neurovascular structures than anteromedial plating with posterolaterally directed screw fixation. It has already been demonstrated that posteromedial plating shows superior fixation stability in contrast to anteromedial plating. 11 While the screw length was also longer in the TomoFix group than in the TDM or OhtoFix group, this is probably because the TomoFix plate did not fit well on the osteotomized tibia. The distance from the neurovascular structure to the screw extension line was also farther in the LCfit group because the screw angle was small and all proximal screws were far lateral to the neurovascular structures. The screws in the other groups were just lateral and even medial to the neurovascular structures in some cases. The safety angle was wider in the LCfit group than in the other 3 groups. Surgeons can learn how to drill and insert screws safely during fixation using the landmark, the most protruding spot of the anterior tibial cortex.
Limitations
One limitation of this study was that neurovascular safety was analyzed by comparing the screw direction and the distance from the neurovasculature in each plate group. Factors such as patient anatomic variance, knee flexion angle, and vascular status could affect the risk of neurovascular injury. Therefore, to compare the definitive neurovascular safety of each locking plate system, further biomechanical comparisons of the 4 plate groups are necessary. In addition, as there were no cases of neurovascular injury in any of the study groups, the increased safety of the LCfit plate could not be demonstrated, as most modern high tibial osteotomy systems offer the possibility of unicortical locking fixation constructs. However, neurovascular injuries can also occur during drilling of the screw holes, and there are some situations that require bicortical fixation (which can cause neurovascular injury), even we if do not want to use it.
In addition, the 4 different plates were not used randomly, and selection bias could have affected the results. However, no selection criteria outside of the operation period were applied to determine the plate type, and there were no differences in the demographic characteristics between the 4 groups. Finally, the synchronizing method of neurovascular structures from the MRI scan to the CT scan is not validated. Even though we found the most similar image to the MRI scan on the CT scan, there should be measurement error caused by the different direction of cross section or the different magnification between MRI and CT scans. Therefore, further cadaveric studies to standardize this method are necessary.
Conclusion
The distance from the neurovascular structures to the screw extension line was significantly farther and the safety angle was also significantly wider with the laterally directed posteromedial plate system compared with the other systems. There were no neurovascular injuries in any group or significant differences in clinical outcomes or radiological parameters between the LCfit and the other locking plate systems.
Footnotes
Final revision submitted January 26, 2022; accepted March 9, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2021R1A2C1092657). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seoul National University Bundang Hospital (reference No. B-2109-708-106).