
Abstract
Purpose
This study aims to compare the mid-term radiographic, clinical results and survivorship between distal tibial tuberosity high tibial osteotomy (DTT-HTO) and conventional biplanar medial open-wedge high tibial osteotomy (cOW-HTO).
Methods
The weight-bearing line ratio (WBL%) and medial proximal tibial angle (MPTA) were evaluated using a standing anteroposterior view of lower extremity. The posterior tibial slope (PTS), Caton-Deschamps index (CDI), tilting angle (TT) and lateral shift ratio (LSR) were evaluated using the lateral views and Merchant views. The Knee Society (KS) knee and function score, Lysholm score, and Anterior Knee Pain Scale (Kujala score) were were used to evaluate the functional outcomes. All parameters were evaluated preoperatively and at the final follow-up. The postoperative complications and survivorship for both groups were also evaluated during the follow-up period.
Results
The WBL% and MPTA exhibited no significant differences between the two groups preoperatively and at the final follow-up. The postoperative CDI and TT in the cOW group decreased significantly compared with the DTT group (p = .037 and .041, respectively). The PF grade showed a significant increase after DTT-HTO and cOW-HTO (p = .036 and <0.001, respectively). Furthermore, the postoperative PF grade of cOW group was significantly higher than that of DTT group (p = .039). The KS knee and function score, Lysholm score, and Kujala score for both groups improved similarly at the final follow-up. The survivorship free of revision was 92.7 % in the DTT group and 94.2% in the OW group.
Conclusions
Despite observing a lower risk of PF joint progression in DTT-HTO compared to cOW-HTO, the clinical outcomes and survivorship after DTT-HTO and cOWHTO were comparable over a mid-term follow-up.
Background
High tibial osteotomy (HTO) has been an effective method in the treatment of medial knee osteoarthritis (OA) by shifting the weight-bearing load from the medial compartment to the viable lateral portion to restrict OA progression, potentially postponing or even avoiding the need for total knee arthroplasty (TKA).1,2 There are two possible approaches when performing medial open-wedge (OW) HTO: uniplanar and biplanar. Conventional biplanar OW-HTO (cOW-HTO) is a widely used technique for correcting varus deformity in the knee joint, and excellent mid-to long-term follow-up results have been reported.1,3 The Tomofix rigid locking plate has been extensively utilized in cOW-HTO due to its considerable advantages, including excellent rotational stability via anterior buttressing against sagittal tilting, preservation of the proximal tibia morphology, higher correction accuracy, and a lower risk of nerve damage. 4 However, the osteotomy site is located in the proximal of tibial tubercle, which may cause abnormal changes of the tibial tubercle and patella infera. 5 Previous studies have reported that osteotomy by downsloping the tibial tubercle or below the distal tibial tubercle should be performed.6,7 Despite such attempts, the osteotomy area is located in the cortical bone, which might result in a lower rate of bone healing and greater torsional stress on the plate. To avoid the disadvantages, a novel operation technique was developed, involving the distal tibial tuberosity HTO (DTT-HTO) by performing the osteotomy in the distal third of the tibial tubercle.2,8 Potential benefits of DTT-HTO include the constant patellar height through maintaining the position of tibial tubercle, and superior mechanical stability because of the two plate-leg design of the π plate.9,10
Previous studies have indicated that DTT-HTO showed the inconspicuous effect on the patellofemoral (PF) joint, and excellent short-term clinical outcomes have been reported.8,9 Currently, there is limited knowledge regarding the mid-term results of DTT-HTO in comparison to cOW-HTO. Therefore, further research is needed to better understand and compare the outcomes of these two techniques in the mid-term. To provide an update for the previous reports, the purpose of the present study was to compare the mid-term radiographic, clinical results, and survivorship between DTT-HTO and cOW-HTO. Our hypotheses were a) the PF OA after DTT-HTO was less progressive than that after cOW-HTO; b) both DTT-HTO and cOW-HTO achieved excellent clinical outcomes at the mid-term follow-up.
Materials and methods
Patient selection
Between June 2016 and December 2018, a total of 125 consecutive patients (141 knees) who experienced HTO for the treatment of unicompartmental medial knee OA were analyzed. Patient data was extracted from an existing database which contained prospectively collected information. The study received approval from the Institutional Review Board of our hospital (20bkkyLW005). Written informed consent was obtained from all participants prior to surgery. Patients who met the following criteria were excluded from the surgery: (1) the incomplete clinical or radiological data (n = 7); (2) unwillingness to participate (n = 3); (3) lost to follow-up at the final assessment (n = 8). The HTO procedures were performed using either the DTT-HTO or cOW-HTO technique. All patients had a minimum follow-up period of 2 years. Finally, 18 patients (21 knees) was excluded, and 107 patients (120 knees) in the study were available for analysis. A total of 55 patients (64 knees) were divided into the DTT group, and a total of 52 patients (56 knees) were divided into the cOW group (Figure 1). Flow diagram for the patient enrollment. HTO, high tibial osteotomy; DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO.
The inclusion criteria for HTO were (1) medial unicompartmental OA; (2) medial proximal tibial angle (MPTA) < 85°, normal mechanical lateral distal femur angle (87 ± 3°), varus deformity ≥5°; (3) Kellgren-Lawrence (K-L) grade ≥Ⅱ 11 ; and (4) body mass index (BMI) ≤ 30 kg/m2. The exclusion criteria for surgery were as follows: (1) previous knee surgery, such as ligament reconstruction or femoral osteotomy; (2) septic or rheumatoid arthritis; (3) knee motion range <100° or flexion contracture >10°; (4) symptomatic knee pain of the lateral compartment; and (5) ligamentous instability around the knee.
The radiographic evaluation
The radiographs were analyzed using a picture-archiving and communication system (PACS, PiView STAR, Seoul, Korea). The procedure was as follows: (1) A computed tomography (CT) scan of the knee joint was performed post-surgery to evaluate the positioning of the osteotomy in both techniques (Figure 2); (2) The degenerative changes of knee OA were recorded according to the K-L grade
9
using the anteroposterior (AP) views preoperatively. (3) The weight-bearing line ratio (WBL%, calculated as the percentage of the distance between the intersection point A of the mechanical axis and the medial border of the tibial plateau to the width of the tibial plateau), and MPTA (∠ α, the angle between the anatomical axis of the tibia shaft and the tangent of the tibial plateau) were evaluated in the weight-bearing AP view of the entire lower extremity
6
(Figure 3(a) and (b)); (4) The posterior tibial slope (PTS, 90° -∠β, the angle between the tangent of the tibial plateau and a line perpendicular to the anatomical axis of the tibia), and Caton-Deschamps index (CDI, L2/L1, the ratio of the length from the distal surface of the patella to the anterior tibial tubercle to the length of the joint surface of the patella) were evaluated using lateral views of the knee joint
9
(Figure 3(c)). The patellofemoral (PF) grade, tilting angle (TT), and lateral shift ratio (LSR) were assessed using the Merchant view with the knee flexed to 45°
12
(Figure 3(d) and (e)). The degenerative changes of PF joint were recorded according to the K-L grade. TT (∠γ) represents the angle between the line passing through the widest part of the patella and the line connecting the anterior surfaces of the femoral condyles. LSR is defined as the ratio of the distances b1b2/L5L6. L5 indicates the perpendicular line passing through the summit of the lateral femoral condyle (b1) to L7 (the line between b1 and the summits of the medial femoral condyles [b2]). L6 indicates the perpendicular line passing through the lateral edge of the patella to L7. Changes in radiographic parameters indicate the differences between the postoperative and preoperative values. All radiographic data were assessed preoperatively and at the final follow-up. The radiographic assessment (a, b, c, d DTT-HTO; e, f, g, h cOW-HTO). a, b the CT scan of the osteotomy site position in DTT-HTO; c, d a π plate was used in DTT-HTO. e, f the CT scan of the osteotomy site position in cOW-HTO; g, h a Tomofix plate plate was used in cOW-HTO. DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO. The radiographic measurement. a, weight-bearing line ratio (WBL%, the percentage of the distance between the tibial platform intersection point A of the mechanical axis and the medial border of the tibial plateau to the tibial plateau width); b, medial proximal tibial angle (MPTA = ∠α, the medial angle between anatomic axis of the tibia shaft and tibial plateau tangent); c, The posterior tibial slope (PTS) = 90°-∠β, Caton-Deschamps index (CDI) = L2/L1; d, tilting angle (TT = ∠γ, the angle between the line intersecting the widest bony structure of the patella and the line connecting the anterior surface of the femoral condyles); e, lateral shift ratio (LSR, the ratio of the distances b1b2/L5L6).

The clinical evaluation and survivorship
During the clinical assessment, the Knee Society (KS) knee and function score, 13 Lysholm score, 14 and Anterior Knee Pain Scale (Kujala score) 15 were evaluated preoperatively, and at the time of the second revision or the final follow-up for patients free of revision. The postoperative complications and survivorship for both groups were also evaluated during the follow-up period.
Surgical procedures and rehabilitation
Prior to HTO, arthroscopic procedures were implemented to evaluate the state of the menisci, anterior cruciate ligaments (ACL), and articular cartilage. Arthroscopic debridement, which involves the irrigation of joint cavity and removal of any loose cartilage debris, was conducted when it was determined to be necessary. Additionally, meniscal resection or repair was conducted as an integral part of the surgical intervention when deemed necessary. In DTT-HTO, osteotomy was started from the distal third of the tibial tubercle on the medial side of the proximal tibia utilizing C-arm guidance 9 (Figure 2(a) and (b)). The detachment of the superficial layer of the medial collateral ligament (sMCL) and pes anserinus was implemented at the proximal medial side of the tibia. Two Kirschner wires were used to mark the osteotomy site from the distal third of the tibial tubercle to the caput fibulae. Osteotomy was performed using an osteotome and an oscillating saw below the two Kirschner wires, up to 10 mm from the lateral cortex, then the lateral cortex of the tibia was drilled to weaken the hinge. The osteotomy site was opened at the posterior gap, and the target point was maintained by 55% - 65% of the tibial plateau width based on the preoperative meniscus or cartilage status.16,17 A π plate 2 (Shuangyang, China) and locking screws were used to fix the osteotomy site (Figure 2(c) and (d)). In cOW-HTO, the osteotomy was started approximately 4 cm below the joint line. The transverse osteotomy was obliquely implemented from the upper edge of the pes anserinus tendon to the “safe zone” 18 using a bone saw and chisels, and the ascending osteotomy was performed at an angle of 110° behind the tubercle (Figure 2(e) and (f)). The ratio of anterior-posterior gap was adjusted about half to two-thirds to maintain the normal PTS. 19 The osteotomy site was progressively opened to a range of 55% - 65% of the tibial plateau width based on the preoperative meniscus or cartilage status.16,17 A Tomofix plate (DePuy Synthes, Switzerland) and locking screws were used to fix the osteotomy site (Figure 2(g) and (h)). The osteotomy gaps were filled with cancellous bone chips and bone morphogenetic protein (BMP). After wound closure was complete, pressure bandages were applied to relieve joint swelling.
Continuous passive motion exercise was recommended on the first day after HTO. Within 2 weeks of the surgery, some partial weight-bearing exercise was allowed with the help of a walking aid. Tolerable full weight-bearing walking was permitted between 4 and 6 weeks postoperatively.
Statistical analysis
An a priori power analysis was implemented based on the previous research.1,12 A sample size of 98 patients (49 patients per group) was calculated to detect such a difference with α = 0.05 and a power of 80% to verify the hypothesis. Therefore, we calculated the estimated sample size of 55 patients in the HTO group, and 52 patients in the control group.
Statistical analysis was performed using SPSS 21.0 and a mean standard deviation was calculated. The demographics and surgery data, radiographic and clinical parameters, and complications were compared according to the independent-sample t-test. The categorical variables were compared using Chi-square test or Fisher’s exact test. The knee OA and PF grade between the two groups were compared using the Mann-Whitney U test. Kaplan-Meier survival curves were used to estimate the probability of failure using the need for total knee arthroplasty (TKA) conversion as the end point. A p value <.05 was considered to be statistically significant. In order to evaluate the reliability of the radiological measurement, the intra- and inter-rater intraclass correlation coefficients (ICCs) were calculated by two independently experienced observers with a time interval of at least 2 weeks. An ICC greater than 0.75 indicated good repeatability, while an ICC lower than 0.40 suggested poor repeatability.
Results
Baseline characteristics and surgery information of the patients.
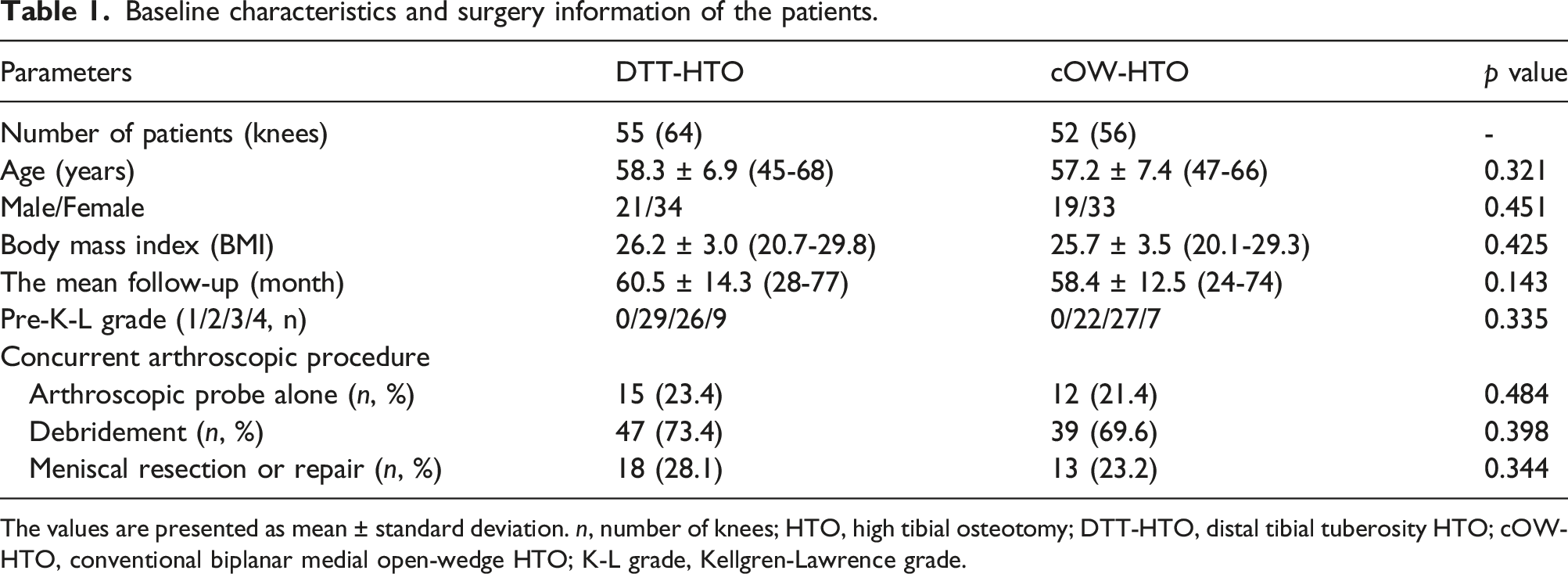
The values are presented as mean ± standard deviation. n, number of knees; HTO, high tibial osteotomy; DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO; K-L grade, Kellgren-Lawrence grade.
The radiographic outcomes between DTT-HTO and cOW-HTO preoperatively and at the final follow-up.

Data are presented as mean ± standard deviation. n, number of knees; the changes in radiographic parameters indicate the differences between postoperative and preoperative values. DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO; WBL%, weight-bearing line ratio; MPTA, medial proximal tibial angle; PTS, posterior tibial slope; CDI, Caton-Deschamps index; TT, tilting angle; LSR, lateral shift ratio; PF grade, patellofemoral grade. * The statistical significance was set at p < .05.
The clinical outcomes between DTT-HTO and cOW-HTO preoperatively and at the final follow-up.

The values are presented as mean ± standard deviation. DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO; KSKS, Knee Society knee score; KSFS, Knee Society function score; Kujala score, Anterior Knee Pain Scale.
The details of the complications between DTT-HTO and cOW-HTO.

n, number of knees; DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO.
The survivorship free of revision was 92.7 % in the DTT group and 94.2% in the cOW group (Figure 4). There were no significant differences observed in the mean time to revision between DTT group and cOW group (50.5 months ± 12.4 and 54.7 ± 15.1 months, p = .286). In the DTT group, four patients were converted to TKA. One revision was performed due to deep infection, which resulted in conversion to TKA after plate removal and administration of antibiotics. Two revisions were conducted due to under-correction (47.2% of the tibial plateau width). Additionally, one revision was performed due to over-correction (66.8% of the tibial plateau width). In the cOW group, three patients were converted to TKA. Two revisions were performed due to over-correction (68.2% of the tibial plateau width). One revision was conducted due to under-correction (44.5% of the tibial plateau width). Kaplan-Meier survivorship analyses. The red line represents the survival rate for DTT-HTO, and the blue line represents the survival rate for cOW-HTO. DTT-HTO, distal tibial tuberosity HTO; cOW-HTO, conventional biplanar medial open-wedge HTO.
Discussion
The purpose of the present study was to compare the radiographic, clinical outcomes, and survivorship between DTT-HTO and cOW-HTO over a mean follow-up period of 5 years. The two most important findings were the lower risk of PF degeneration after DTT-HTO and the similar mid-term clinical outcomes and survivorship between the two groups. The results prove the original hypothesis. To the present knowledge, the study is the first in which the mid-term radiographic, clinical results, and survivorship between DTT-HTO and cOW-HTO were compared. The findings contribute to a more comprehensive understanding for clinical decision-making when selecting patients for HTO treatment.
Regarding the PF congruency after HTO, our results demonstrated a statistically significant decrease in TT after cOW-HTO, while no significant alteration in PF congruity was observed after DTT-HTO. Previous studies have reported that the TT decreased slightly after cOW-HTO. Gaasbeek et al 20 reported increased medial patellar tilt because of the increased lateral tension of the patella. The findings of Lee et al. 21 in their meta-analysis indicated a significant decrease in the TT but no significant difference in the LSR after cOW-HTO, which is consistent with the results observed in the present study. Conversely, among studies examining DTT-HTO, only Han et al. reported on the short-term clinical outcomes, suggesting that this procedure has minimal effects on PF joint congruity. 9 Our findings in the present study were consistent with previous results, providing further support for the notion of minimal impact on the PF joint after DTT-HTO during the mid-term follow-up period.
In the present mid-term results, cOW-HTO induced the patella infera, whereas DTT-HTO maintained the constant patella height at the final follow-up. Previous studies have indicated that the most common radiographic change found after cOW-HTO with ascending tibial tubercle osteotomy was patella infera. 22 Patella infera can result in a shorter patellar height, which can lead to abnormal patellar tracking, increased stress on the PF joint, and potentially contribute to the development of anterior knee pain and PF joint degeneration. 23 Ishimatsu et al. 24 found that the patellar height decreased significantly, and the degenerative changes of PF joint were observed after cOW-HTO. Egmond et al 25 also reported that cartilage degeneration was frequently found on the PF joint after cOW-HTO, the pressure distribution patterns of the femoral lateral trochlea and the medial portion of the patellar lateral facet after cOW-HTO were also found to be significantly increased using the CT method. Han et al. reported that DTT-HTO did not have a significant effect on patellar height, as they maintained a constant tibial tubercle position 9 ; however, notably, their study had a relatively short follow-up period of 23 months, emphasizing the indispensability of the mid-term studies.
The change in PTS may have a profound influence on the biomechanics and kinetics of the knee joint. The abnormal change in PTS after HTO can adversely affect both cruciate ligaments strain and joint contact forces.26,27 In previous studies, the PTS was prone to increase after cOW-HTO and decrease after closed-wedge (CW) HTO.2,28 In the present study, the PTS after cOW-HTO showed no significant change compared with the preoperative value. Such results could be attributed to the adjustment of the anterior-posterior gap ratio by about half to two-thirds when opening the osteotomy site. The PTS after DTT-HTO decreased slightly at the final follow-up, but this difference did not reach statistical significance. The observed reduction in PTS may be attributed to the technical variations between the two procedures, which highlights the potential influence of the specific technique used in DTT-HTO on the PTS. One difference observed in the DTT-HTO procedure compared to cOW-HTO is the absence of an ascending plane. Thus, the inadequate osteotomy in the anterior tibial tubercle would limit the anterior gap opening (Figure 3(b)). Then, the opening position tended to locate in the posterolateral of the osteotomy gap due to the limiting opening in the anterior tibia. The combined factors might contribute to PTS decreasing after DTT-HTO, thereby theoretically decreasing the ACL strain. 26 However, a previous biomechanical study suggested the changed PTS (approximately 4.4°) after HTO does not affect situ forces of cruciate ligaments, whether under isolated anteroposterior or axial pressure load or under combined pressure. 29 Based on the present results, which indicate that the change in PTS after DTT-HTO was less than 1°, it is likely that there would be little effect on cruciate ligament tension.
Previous studies demonstrated that excessive valgus alignment after HTO were the factors affecting PF cartilage degeneration. Lee et al. 30 indicated that postoperative mechanical alignment, potentially resulting from overcorrection, is significantly associated with the degeneration of PF cartilage. Yoon et al. 31 found that a postoperative mechanical alignment of 62% was identified as the only risk factor. Song et al. 15 reported that PF cartilage degeneration was prone to further progression after OWHTO and CWHTO in patients with a correction angle >10°. In our results, the postoperative mechanical alignment and corrction angle between DTT-HTO and cOW-HTO were found to be comparable at the final follow-up (58.9% and 57.6%, 9.8° and 9.1°, respectively). Therefore, the effect of valgus alignment on PF degeneration was found to be comparable between two groups. In the present study, there were 15 of 64 knees exhibiting large valgus alignment after DTT-HTO, and 12 of 56 knees were observed after cOW-HTO, potentially contributing to the degeneration of PF cartilage at the final follow-up.
In the present study, despite the more severe PF degeneration observed after cOW-HTO compared to DTT-HTO, both groups showed similar excellent mid-term clinical results. Such findings are supported with previous studies. Yoon et al. 31 evaluated the American Knee Society (AKS) score, Knee Injury and Osteoarthritis Outcome Score (KOOS), and Kujala score with a minimum 5-year follow-up, and found that PF degeneration did not affect the clinical outcomes or survivorship after cOW-HTO. In another study, Kim et al. 13 reported that the outcomes in the PF joint, including the cartilage status and clinical scores, remained unchanged after cOW-HTO, despite the presence of patellar infera. Similarly, Lee et al. 32 performed a retrospective study to evaluate the clinical and radiologic outcomes of PF joint after cOW-HTO, and indicated that the functional results were significantly improved after surgery, despite descent of the patella observed after a mean follow-up of 44 months.
Survival rates observed in the present study for both DTT-HTO and cOW-HTO were comparable, which were similar to values reported in the literatures. Previous studies have reported that superior survival rate following cOW-HTO varied from 80-95% after mid-to long-term follow-up.33,34 Egmond et al. 25 reported that 91.7% of survival after 5 years and 81.3 % after 7.9 years were obtained after cOW-HTO. In a study by Akizuki et al., 35 the survival rate after 10 years was reported to be 97.6%. Further, the survival rate after 15 years was noted to be 90.4%, with TKA being the endpoint. In the present results, the survival rate in DTT-HTO at a mean follow-up of 5 years was 92.7 %, in accordance with the survival rate (94.2%) in cOW-HTO. Consequently, although the extent of PF progression after cOW-HTO was inferior to that after DTT-HTO, the comparable excellent mid-term survival rates between the two groups were inconsistent with the extent of PF joint progression at the postoperative follow-up.
The majority of revisions in this study (six out of seven cases) were conducted due to over- or under-correction of mechanical alignment. Such findings are consistent with previous research indicating that the size of correction is an independent factor associated with improved survival of HTO. 36 Thus, an association was found between under- or over-correction and failure rate after surgery. However, the total number of patients (six) with such a correction was considerably small, and further larger sample size studies should be conducted for more reliable results.
There were several limitations to the present study. Firstly, the present study exhibited inherent biases similar to those observed in retrospective studies, including the potential selection bias in group assignment, despite the surgeon’s attempts to randomize allocation as much as possible. Although there were no significant differences in patient characteristics or preoperative status between DTT-HTO and cOW-HTO, a more elaborate design in a prospective randomized study would provide more reliable data. Secondly, there was no evaluation of the cartilage status of PF joint using arthroscopy at the final follow-up. Thus, the more detailed status of cartilage degeneration in the PF joint could not be further assessed. In addition, conducting a mean follow-up period of only 5 years may have been inadequate to detect the differences in clinical outcomes between the two techniques. Further high quality, prospective long-term follow-up is required to draw more concrete conclusions.
Conclusion
Despite observing a lower risk of PF joint progression in DTT-HTO compared to cOW-HTO, the clinical outcomes and survivorship after DTT-HTO and cOWHTO were comparable over a mid-term follow-up.
Footnotes
Acknowledgments
The authors gratefully acknowledge all volunteers who participated in this study, and the financial support from the Special Fund for Science and Technology Development of Beijing Rehabilitation Hospital (No.2022-053).
Author contributions
Study design: FLS. Administrative support: FLS. Surgery performance: FLS, HBG. Data collection: KL, HQW. Data analysis:KL. Writing manuscript: KL. Approving final version of manuscript: FLS. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Special Fund for Science and Technology Development of Beijing Rehabilitation Hospital (No.2022-053).
Ethical statement
Data Availability Statement
Data and materials for this study are not publicly available, but can be availabled from the corresponding author.