
Abstract
Background:
There exists some controversy regarding whether patient age is a predictive factor for outcomes after high tibial osteotomy (HTO).
Purpose/Hypothesis:
The purpose of this study was to evaluate whether patient age affects clinical and radiological outcomes after medial open-wedge HTO (OWHTO) in a large population with a wider age range than previous studies. It was hypothesized that there would be no differences in outcomes when compared across age-groups.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective comparative study was conducted using 344 patients (303 knees) who underwent OWHTO from 2009 to 2018. These patients were divided into 3 groups based on age at the time of surgery: ≥55 years (group Y: 76 knees in 57 patients), 56 to 64 years (group M: 129 knees in 120 patients), and ≤65 years (group O: 139 knees in 126 patients). Clinical and radiological evaluations were performed immediately before surgery and at the final follow-up period, at a mean of 5.1 years (range, 3-11 years). Comparisons among the 3 groups were conducted with 1-way analysis of variance for continuous variables. When a significant result was obtained, a post hoc test with Bonferroni correction was conducted for multiple comparisons.
Results:
In clinical evaluations, there were no significant differences among the 3 groups either preoperatively or postoperatively concerning the Japanese Orthopaedic Association score, the Lysholm score, or the Knee injury and Osteoarthritis Outcome Score (KOOS), with the exception of the preoperative KOOS Symptoms subscale, which was significantly higher in group Y versus group O (48.9 ± 18.7 vs 58.7 ± 15.4, respectively; P = .011). The Tegner activity score was significantly different among the groups, both preoperatively and postoperatively (P < .001 for both). There was no significant difference in the occurrence of complications or the survival rate at final follow-up among the 3 groups.
Conclusion:
The study findings suggest that patient age does not affect clinical and radiological outcomes after OWHTO.
Open-wedge high tibial osteotomy (OWHTO) is a useful surgical option for medial osteoarthritis (OA) in knees.19,32 However, many risk factors that affect the mid- or long-term outcomes have been reported.6,7,10,20,23,26,32 The age of the patient at the time of surgery was suggested as a potential predictive factor for the outcome of OWHTO. 35 Many clinical studies have been widely conducted to clarify whether the age of the patient is a predictive factor for the outcome of OWHTO.2,7,9,12,14,15,29,36,37 However, there has been some controversy among previous studies. For example, many studies analyzed this age question using regression analyses. The majority of previous studies indicated that patient age was a significant factor that reduced the survival rate of OWHTO, which was defined by conversion to total knee arthroplasty (TKA).12,14 However, other studies reported that patient age was not a significant factor related to the survival rate, complications, or bone union at the osteotomy site.7,29,36,38 Thus, it remains unclear whether patient age at the time of surgery is a factor influencing survival rate after OWHTO.
A study by Kohn et al 15 compared younger patients (mean age, 42 years; range, 39-47 years) to an older group (mean age, 57 years; range, 55-63 years) and found no significant differences in the clinical outcomes between the 2 groups. This study, however, included only 13 patients in each group. The aim of this study was to use a similar design in a larger population to evaluate whether age affects clinical and radiological outcomes after OWHTO. We hypothesized that no significant differences would be found in clinical or radiological outcomes of OWHTO when compared according to age.
Methods
Study Design
Institutional review board approval was obtained for the study protocol, and informed consent was obtained from all participants. This retrospective comparative study involved 385 knees of 341 patients who underwent OWHTO from January 2009 to June 2018 at a single institution. The indications for OWHTO were (1) patients with persistent knee pain during daily, occupational, or sports activities due to medial OA or a varus knee with spontaneous osteonecrosis of the knee (SONK) in the medial femoral condyle after nonoperative treatment for at least 3 months, and (2) patients who had the desire to continue with active physical activities. The contraindications were (1) lateral femorotibial angle (FTA) >185°, (2) loss of knee extension >15°, (3) loss of knee flexion <130°, (4) history of knee infection, (5) severe patellofemoral (PF) joint OA as determined by Kellgren-Lawrence 13 grade >3, and (6) anterior cruciate ligament insufficiency or varus/valgus instability >10°. All operations were performed by 1 of 3 senior orthopaedic surgeons (T.Y., K.Y., and E.K.), who were sufficiently trained in OWHTO from 2005 at the same institution and had >30 years of experience with knee surgery. Clinical and radiological evaluations were performed immediately before surgery and at the final follow-up period. The mean follow-up period was 5.1 years (range, 3-11 years).
Of 385 knees in 341 patients, 41 knees (38 patients) were excluded from this study, because 35 knees (32 patients) were lost to follow-up and 6 knees (6 patients) did not undergo part of the scheduled radiological examinations. Consequently, the remaining 344 knees (303 patients) were included in this study (Figure 1). These patients were divided into the 3 groups based on age at the time of surgery: the first group, aged ≤55 years (group Y; 76 knees in 57 patients); the second group, aged 56 to 64 years (group M; 129 knees in 120 patients); and the third group, aged ≥65 years (group O; 139 knees in 126 patients) (Figure 1).

Flowchart of patient inclusion in this study. OWHTO, open-wedge high tibial osteotomy.
Patient Characteristics
Table 1 summarizes the baseline characteristics of the patients. There were significant differences in age (P < .001), bilateral knee ratio (P < .001), height (P = .028), weight (P < .001), body mass index (BMI) (P = .001), and bone mineral density (BMD) (P = .002) among the 3 groups. There were no significant differences among the 3 groups in the follow-up period (Table 1).
Patient Characteristics According to Study Group (N = 344 Knees, 303 Patients) a

Data are reported as absolute value or mean ± SD (range) unless otherwise indicated. Boldface P values indicate a statistically significant difference among the 3 study groups (P < .05).
Significantly different from group M.
Significantly different from group O.
Bone mineral density is shown as the rate (%) compared to the young adult mean.
Preoperative Planning
Preoperative planning with an appropriate correction angle of the tibia was performed with the aid of a standing, full-length lower limb anteroposterior (AP) radiograph. The surgical planning methods have been previously described. 38 The hinge point P was located approximately 5 mm medial from the proximal tibiofibular joint (Figure 2). First, line A was drawn from the center of the femoral head through the point at 65% lateral from the medial edge of the lateral tibial plateau because sufficient valgus correction is needed to obtain excellent 10-year results.25,27,31,39 Second, line B was drawn from hinge point P to the center of the talar dome. Then, arc C was drawn so that it was across line A; the center and radius of arc C were the hinge point P and line B, respectively. Next, line D was drawn from hinge point P to the crossing point between line A and arc C. The angle formed between lines B and D is the correction angle. Of note, double-level osteotomy should be considered for varus knees with the preoperatively anticipated medial proximal tibial angle (MPTA) >95°. 24 Patients who underwent double-level osteotomy were excluded from this study.

Preoperative planning on standing full-length lower limb anteroposterior radiograph. The angle formed between lines B and D (α) is the correction angle.
Preoperative Arthroscopy and Additional Treatment
Each patient underwent diagnostic arthroscopy immediately before high tibial osteotomy (HTO) surgery. Diagnostic arthroscopy was performed with standard anterolateral and anteromedial parapatellar portals to confirm that there was an isolated medial compartment OA or SONK. Concomitant procedures were performed to address medial compartment chondral injury or meniscal disease.
Degenerative findings were observed in the medial menisci of all cases. Partial meniscectomy was performed for unstable meniscal tears in 210 knees (Table 2). Debridement was performed for fragmentation of the cartilage. No treatment was administered for softening or fissuring of the articular cartilage. Osteochondral autograft transfer was carried out in 25 knees using the Osteochondral Autograft Transfer System (Arthrex). There were no significant differences in the tear pattern of the medial meniscus or additional treatments among the 3 groups.
Preoperative Arthroscopic Findings and Additional Treatment According to Study Group (N = 344 Knees) a
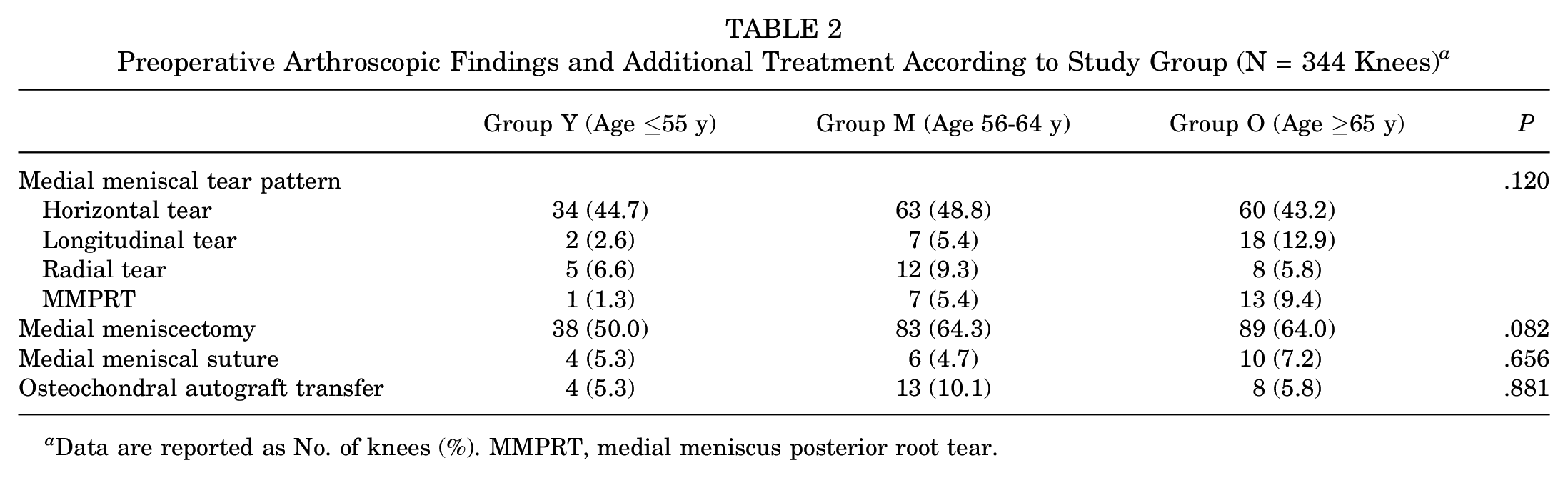
Data are reported as No. of knees (%). MMPRT, medial meniscus posterior root tear.
Surgical Procedure and Postoperative Rehabilitation
This OWHTO procedure has previously been reported in detail.16,26,30,38 Briefly, the proximal tibia was exposed through a 7-cm medial longitudinal incision. After complete release of the distal attachment of the superficial medial collateral ligament, 3 guide wires were inserted into the tibia so that each inserted guide wire precisely reached the proximal tibiofibular joint using the parallel guide. Next, a biplanar osteotomy of the tibia, which consisted of an oblique HTO and a frontal plane osteotomy behind the tibial tubercle, was performed with an oscillating saw and chisel. Under fluoroscopic observation, the oblique osteotomy site was gradually opened by use of a protractor installed by a specially designed spreader (Olympus Terumo Biomaterials) until the preoperatively planned opening angle was obtained. The medial opening angle was determined for each knee so that the mechanical axis in the corrected limb passed through a point on the lateral tibial plateau, which was approximately 65% lateral to the medial edge of the tibial joint surface. 8 Then, 2 wedge-shaped beta-tricalcium phosphate spacers (Osferion 60; Olympus Terumo Biomaterials) were implanted into the anterior and posterior parts of the opening space. 26 Finally, the tibia was fixed with a locking plate (TomoFix, DePuy Synthes or TriS Medial HTO Plate System, Olympus Terumo Biomaterials) by inserting 8 locking screws into the tibia (Figure 3).
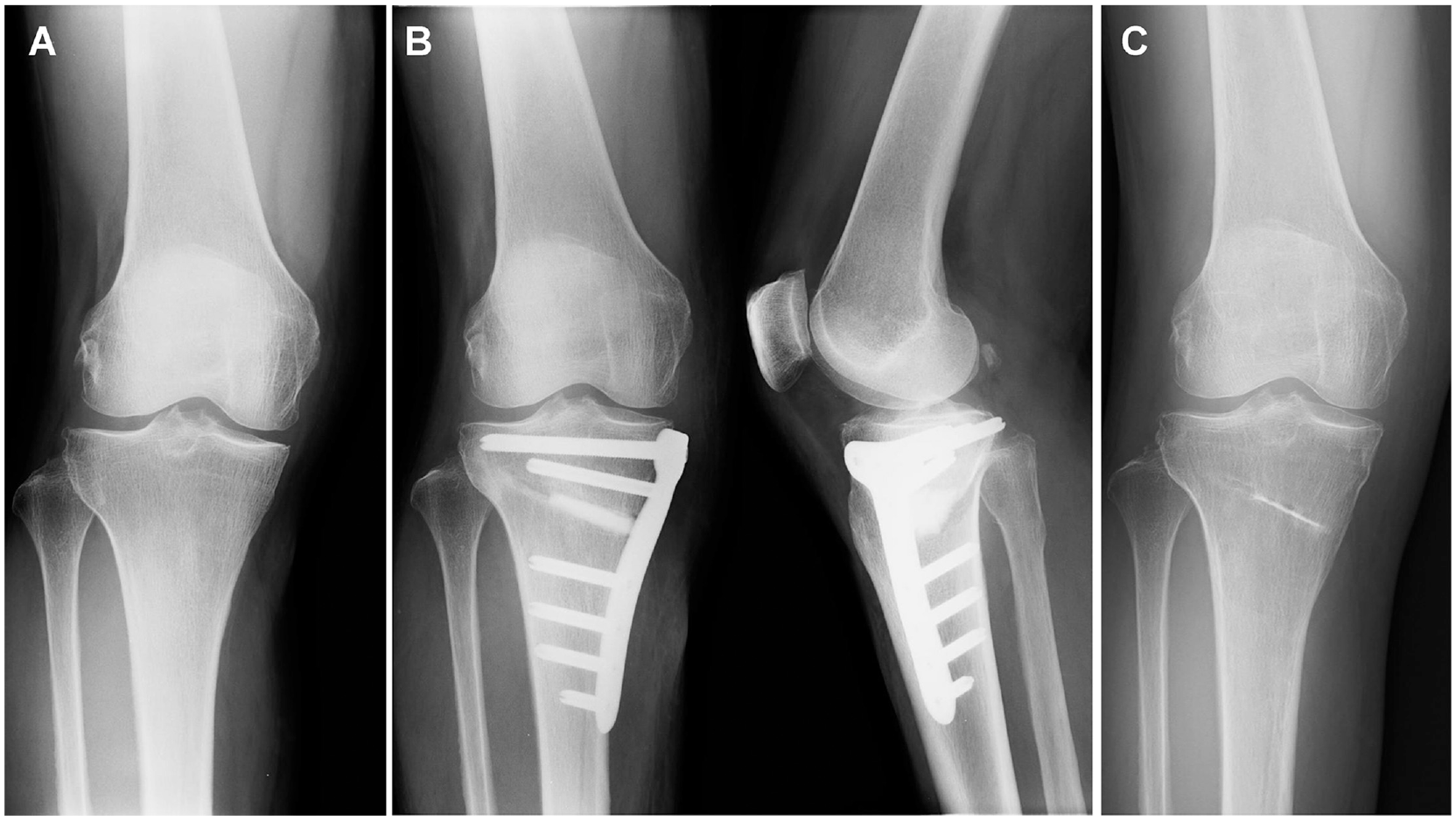
A representative case of the open-wedge high tibial osteotomy surgery. (A) Before surgery. (B) Immediately after surgery. (C) At the final follow-up (4 years after surgery).
Each patient underwent an additional procedure at a mean of 12.7 months (range, 6-30 months) after the initial surgery to remove the implanted plate and screws.
All patients underwent postoperative management using the same previously reported rehabilitation protocol. 26 Straight-leg raising and quadriceps setting exercises, as well as active and passive knee motion exercises, were encouraged on the day after surgery. Partial weightbearing was permitted with crutches 2 weeks after surgery, and full weightbearing was allowed 4 weeks after surgery.
Radiological Evaluation
In each patient, AP radiographs of the knee and whole lower limb were taken while standing on the affected limb. Lateral and skyline view radiographs were taken at 30° of knee flexion in the nonloading condition. On the AP radiograph of the knee, the radiological stage of OA was assessed according to the Kellgren-Lawrence grading system. 13 On the AP radiograph of the whole limb radiograph, we measured the FTA, MPTA, and point at which the mechanical axis passed across the joint line (Figure 4A). The patellar height and posterior tibial slope (PTS) angle were measured on the lateral radiograph of the knee (Figure 4B). To quantify the patellar height, the Caton-Deschamps (CD) index 5 was measured at 30° of knee flexion. The CD index was defined as a ratio of the distance between the inferior pole of the patella and the anteroproximal edge of the tibial plateau divided by the patellar length. The PTS angle was defined as the angle between the line perpendicular to the mid-diaphysis of the tibia and the posterior inclination of the medial tibial plateau. BMD was measured with a DXA Bone Densitometer (Discovery A; Hologic) immediately before surgery.

Radiological evaluations. (A) The lateral femorotibial angle was defined as the angle between the longitudinal axes of the femur and tibia. The point at which the weightbearing line passed across the joint line was drawn from the center of the femoral head to the middle point of the ankle joint surface, and the mechanical axis shown as a ratio (%) of the length between the point and the medial edge of the tibial plateau, which was divided by the width of the whole tibial plateau. The medial proximal tibial angle was defined as the angle between the proximal tibial joint line and the mechanical axis of the tibial shaft. (B) The posterior tibial slope angle was defined as the angle between the line perpendicular to the mid-diaphysis of the tibia and the posterior inclination of the medial tibial plateau. The Caton-Deschamps index was defined as a ratio of the distance (Y) between the inferior pole of the patella and the anteroproximal edge tibial plateau divided by the patellar length (X).
All radiological measurements were performed independently by 2 observers (K.Y. and T.K.). The inter- and intrarater reliability for the radiological measurements were 0.91 (range, 0.85-0.96) and 0.93 (range, 0.86-0.98), respectively, indicating a high degree of agreement.
Clinical Evaluation and Complications
Clinical evaluations of symptoms and knee functions were performed in each patient using the Japanese Orthopaedic Association (JOA) scale, which has been the standard knee function scale in Japan,1,38,39 as well as the Lysholm score, 21 the Knee injury and Osteoarthritis Outcome Score (KOOS), 28 and the Tegner activity score. 34
When a complication was clinically or radiologically detected during surgery or follow-up, it was recorded in the electronic medical record system according to previous studies.16,22,33,38 In addition, we recorded the number of knees that underwent conversion to TKA as well as the survival rate (ie, knees that did not undergo TKA conversion) at final follow-up.
Arthroscopic Assessment of Cartilage Injury
In addition to the arthroscopic examination before HTO surgery, patients underwent second-look arthroscopy at the time of removal of the implanted locking plate, which was performed at a mean of 12.7 months (range, 6-30 months) postoperatively.10,17 Morphological changes to the articular cartilage in the knee joint were assessed at both arthroscopic examinations using the International Cartilage Regeneration & Joint Preservation Society (ICRS) classification. 4
Statistical Analysis
Based on previous studies,10,35 a total sample size of 57 patients (57 knees) for each group was calculated a priori to have >90% power to test the study hypothesis. For each study parameter, 1-way analysis of variance (ANOVA) was performed for continuous variables among the 3 groups. When a significant result was obtained, a post hoc test with Bonferroni correction was conducted for multiple comparisons. The chi-square test for determining discrete variables was used. The pre- and postoperative outcomes as well as the change in outcomes (delta) were compared with the paired t test. All statistical calculations were conducted with JMP Pro Version 10.0 for Windows (SAS Institute Japan). The significance level was set at P < .05.
Results
Radiological Evaluation
The radiological evaluations showed that there was a significant difference in knee OA grade among the 3 groups preoperatively (P < .001), and post hoc testing indicated a significant difference between groups Y and M (P = .014) (Table 3). There was also a significant difference in radiological grade of knee OA among the 3 groups postoperatively (P < .001), specifically between groups Y and M (P = .009) and groups M and O (P = .041) (Table 3). Consequently, the pre- to postoperative changes in FTA, MPTA, PTS, mechanical axis, and CD index were significantly different within each group (P < .05 for all). There were no significant differences in the delta value among the 3 groups.
Pre- and Postoperative Radiological Outcomes and Change in Outcomes (N = 344 Knees) a
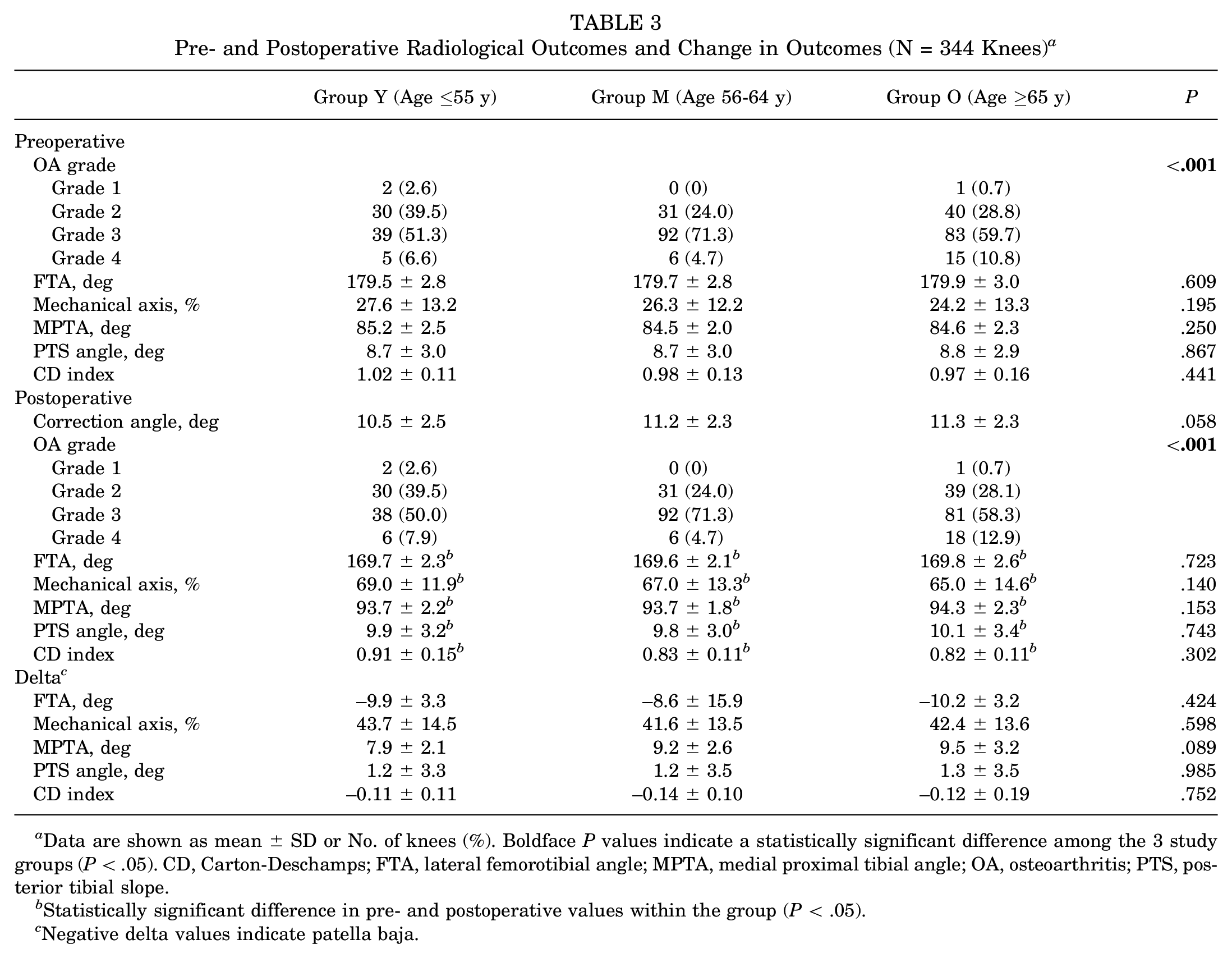
Data are shown as mean ± SD or No. of knees (%). Boldface P values indicate a statistically significant difference among the 3 study groups (P < .05). CD, Carton-Deschamps; FTA, lateral femorotibial angle; MPTA, medial proximal tibial angle; OA, osteoarthritis; PTS, posterior tibial slope.
Statistically significant difference in pre- and postoperative values within the group (P < .05).
Negative delta values indicate patella baja.
Clinical Evaluation
Table 4 shows the results of the preoperative and 5-year follow-up clinical evaluations. Significant pre- to postoperative improvement in the JOA score, Lysholm score, and KOOS were seen in each group (P < .05 for all). There were significant differences among the 3 groups in pre- and postoperative Tegner scores (P < .001 for both). No significant differences were seen among the 3 groups pre- or postoperatively concerning all the clinical evaluation items except for the pre- and postoperative Tegner activity scores (P < .001 for both) and the preoperative KOOS Symptoms subscale (P = .011; post hoc testing revealed significantly higher scores in group Y vs group O, P < .001). In addition, there were no significant differences in the pre- to postoperative change in outcomes among the 3 groups.
Results of Clinical Evaluations Preoperatively and at Final Follow-up (N = 344 Knees) a
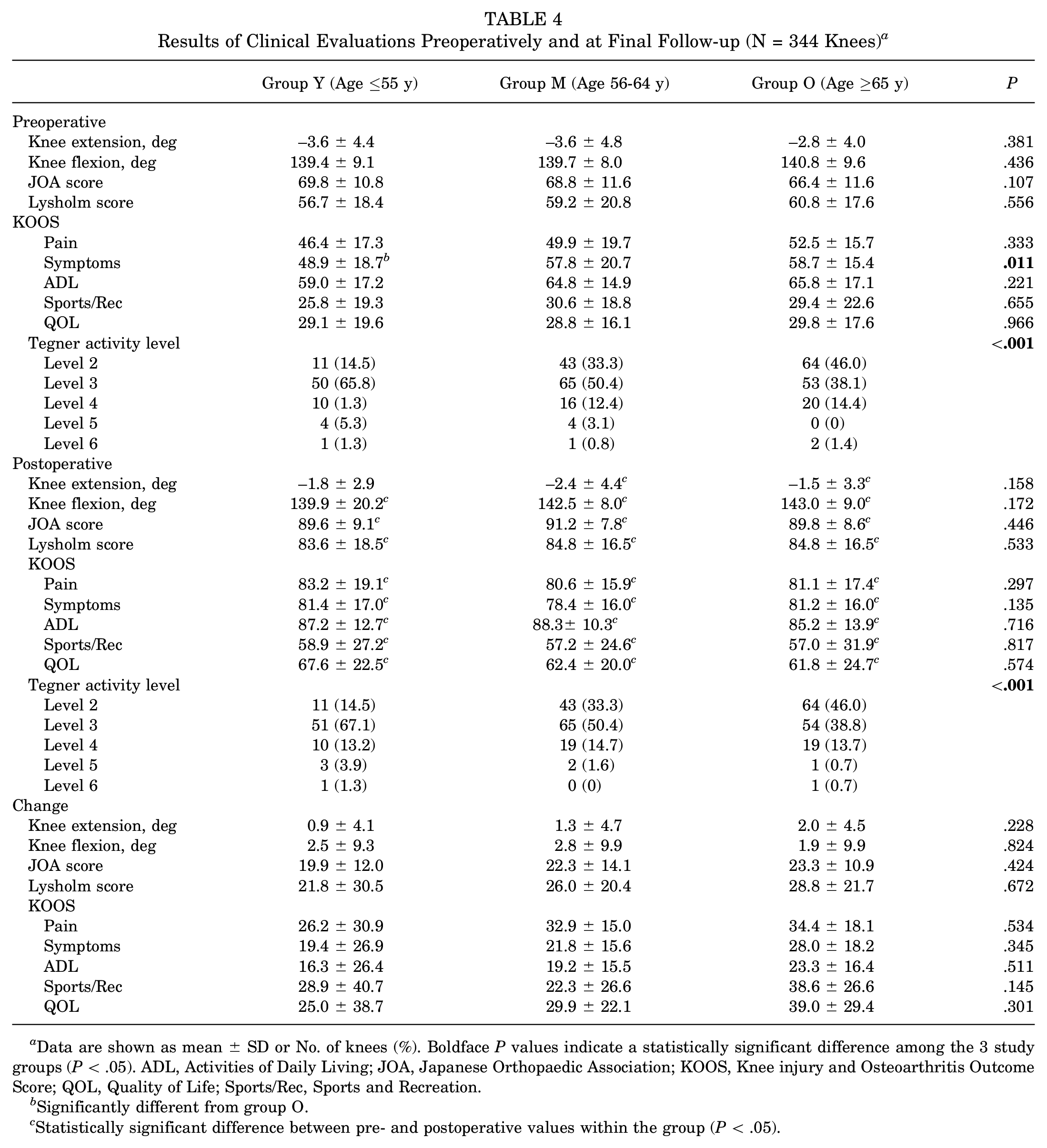
Data are shown as mean ± SD or No. of knees (%). Boldface P values indicate a statistically significant difference among the 3 study groups (P < .05). ADL, Activities of Daily Living; JOA, Japanese Orthopaedic Association; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; Sports/Rec, Sports and Recreation.
Significantly different from group O.
Statistically significant difference between pre- and postoperative values within the group (P < .05).
Complications
Table 5 shows both major and minor complications that occurred during or after the HTO surgery.22,38 In 71 of the 344 knees (20.6%), complications including lateral hinge fracture, superficial infection, unacceptable overcorrection (FTA <160°), correction loss >5°, intraosseous screw breakage, and nonunion were found. There were no significant differences in minor or major complications among the 3 groups. By the final follow-up examination, 4 knees had undergone TKA after HTO because of recurrence of knee pain. In 1 patient of group Y with continuous knee pain, TKA was performed 24 months after surgery. In 3 patients of group O with correction loss or continuous knee pain, TKA was performed 12, 24, and 72 months after surgery. No cases of popliteal vascular injury, peroneal nerve injury, tibial tubercle fracture, or compartment syndrome were noted in any of the 3 groups.
Complications During or After HTO Surgery and Conversion to TKA (N = 344 Knees) a

Data are shown as No. of knees (%). TKA, total knee arthroplasty.
Classification according to Martin et al. 22
Classification according to Takeuchi et al. 33
During the plate removal surgery, implant failure was found in 2, 1, and 3 knees in groups Y, M, and O, respectively (Table 5). We confirmed that 11 locking screws were broken. In these cases, we removed the inserted screw by hollowing out the bone tissue with a core reamer. There were no significant differences in the rate of this complication among the 3 groups.
The overall survival rate at the 5-year follow-up period was 98.7% in group Y, 100% in group M, and 97.8% in group O. There was no significant difference in the survival rate among the 3 groups.
Arthroscopic Assessment of the Cartilage Injury
Table 6 shows the results of the preoperative and second-look arthroscopic assessment of the degree of cartilage degeneration as assessed using ICRS grade. There were significant differences in both the pre- and postoperative cartilage degeneration of the medial femorotibial (FT) joint among the 3 groups (P < .001 for both); post hoc testing revealed that the degree of degeneration in the medial FT joint was significantly greater in groups M and O than in group Y, both preoperatively (P = .001 for each) and postoperatively (group M vs group Y, P = .001; and group O vs group Y, P = .003). Regarding the PF joint, there were no significant differences among the 3 groups, either preoperatively or postoperatively.
Degree of Cartilage Degeneration at Initial and Second-Look Arthroscopy a
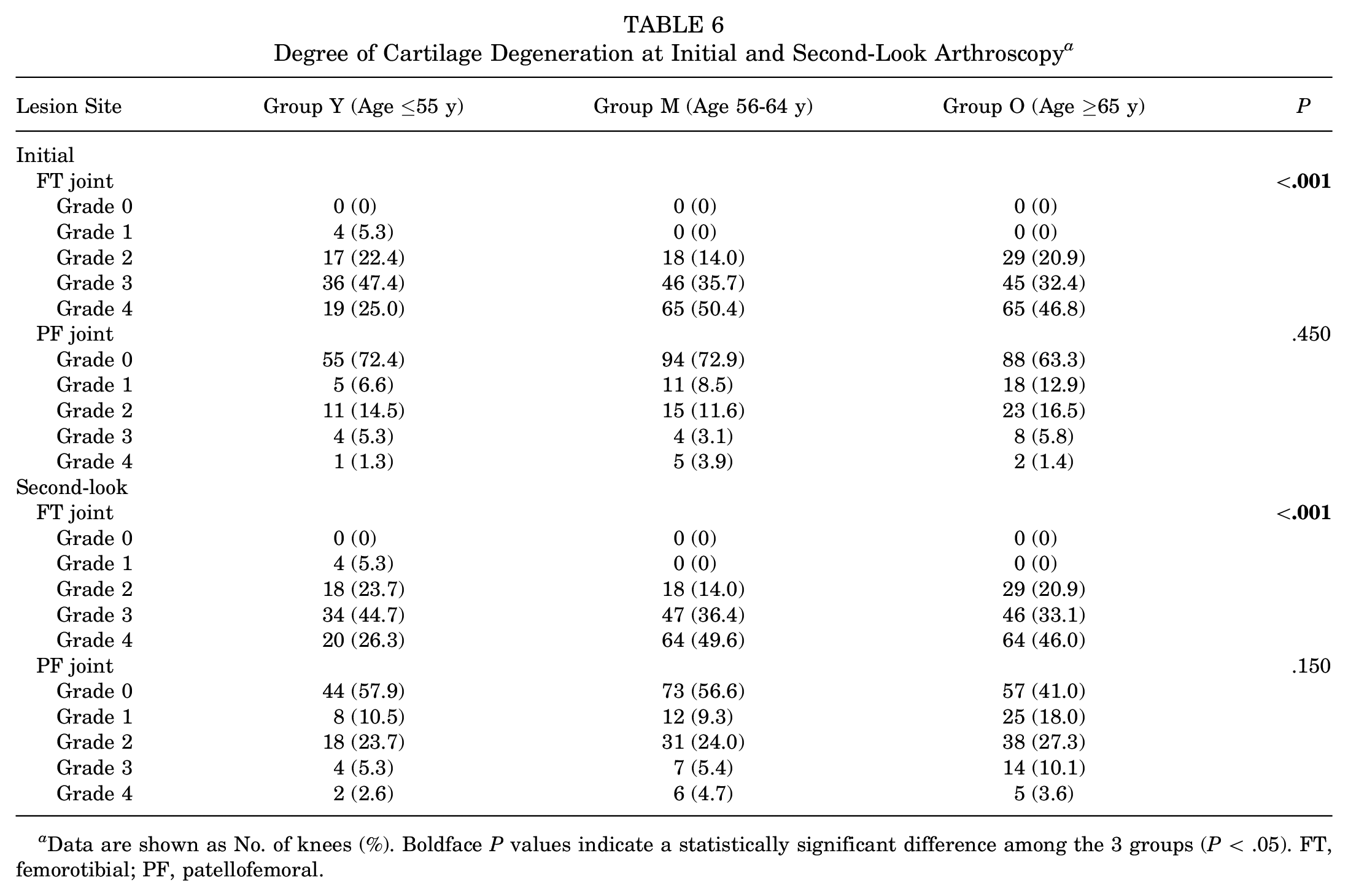
Data are shown as No. of knees (%). Boldface P values indicate a statistically significant difference among the 3 groups (P < .05). FT, femorotibial; PF, patellofemoral.
Additionally, in the medial FT joint, there were no significant differences in degree of cartilage degeneration from pre- to postoperatively within any of the 3 groups. On the other hand, in the PF joint, cartilage degeneration progressed slightly but significantly from pre- to postoperatively within group O (P = .006).
Discussion
The important findings of the present study were that at the 5-year follow-up after OWHTO, there were no significant differences among the 3 age-based study groups in the complication rate, survival rate, or most clinical outcomes, with the exception of KOOS Symptoms and the Tegner activity score. To correctly understand these findings, it is important to pay attention to some differences in the preoperative demographic data. Before surgery, the height, weight, BMI, and BMD were slightly but significantly greater in the youngest group (group Y; patients aged ≤55 years) than in the oldest group (group O; patients aged ≥65 years). These differences are usually seen when comparisons are made for different age-groups. However, there were no significant differences between these 2 groups concerning knee alignment or additional treatments associated with HTO surgery. In addition, the preoperative radiological evaluation showed that there were no significant differences among the 3 groups. Thus, this study demonstrated that the age of patients did not affect the clinical and radiological outcomes after OWHTO, even though preoperative OA grade and degree of cartilage degeneration were significantly different among the 3 study groups.
Only 4 studies9,15,18,35 have reported on the influence of age on clinical outcomes after OWHTO. Trieb et al 35 reported that the clinical results were significantly worse in patients ≥65 years than in patients ≤65 years. On the other hand, Goshima et al 9 and Kuwashima et al 18 found no significant differences in postoperative clinical outcomes between patients aged >65 versus <65 years. In these studies, 65 years was set as the boundary age. However, the most appropriate boundary age with which to evaluate outcomes is unclear.
The design of the present study was similar to that of Kohn et al, 15 but our study included a greater number of knees and a wider patient age range. The findings of the current study showed that patient age did not influence the clinical and radiological outcomes after OWHTO, thus supporting the conclusion of Kohn et al.
Another important point in the present study is that the BMD was measured in each patient, because Goshima et al 9 pointed out that BMD had rarely been measured in previous studies concerning the effect of patient age on HTO outcomes. The mean BMDs in groups Y and O were 96.2% and 86.1%, respectively, showing a significant difference between the youngest and oldest study patients. Nevertheless, there were no significant differences in the clinical results between these 2 groups. In the present study, we did not provide any osteoporosis treatments for the patients with OWHTO who had BMD >80%. However, we provided medicine for osteoporosis to the patients with BMD <70% after the HTO surgery was performed. Under this medical condition, the significant difference in BMD due to the aging factor did not affect the clinical results of HTO.
Concerning the preoperative arthroscopic assessment in the present study, the degree of cartilage degeneration in the medial FT joint was significantly greater in groups M and O than in group Y, similar to the preoperative radiological OA. Commonly, the cartilage degeneration precedes bone changes in OA. Therefore, it is considered that the preoperative degree of OA in groups M and O was somewhat more advanced than that in group Y. The second-look arthroscopy performed at approximately 1 year after HTO showed that the OWHTO surgery did not significantly affect the degree of degeneration in the medial FT joint in each group, and that the degree of cartilage degeneration remained significantly greater in groups M and O than in group Y. However, this postoperative arthroscopic assessment did not influence the mean 5-year clinical evaluations, because there were no differences in the JOA score, Lysholm score, and KOOS among the 3 groups. This finding suggests that OWHTO provided similarly favorable midterm results for each group.
In the previous literature, studies using regression analyses have reported patient age as a significant factor for reducing the conversion rate to TKA.2,3,11,14 Bonasia et al 2 and Bouguennec et al 3 reported that patients >54 to 56 years were significantly associated with poorer outcomes. Other investigators11,12,14 reported that older patient age (>46-50 years) significantly lowered the survival rate of HTO. On the other hand, several studies using regression analyses have reported that patient age was not a significant factor related to survival rate, clinical scores, complications, or bone union rate at the osteotomy site.7,29,36,37 For example, Floerkemeier et al 7 reported that no correlation between patient age and the Oxford Knee Score was observed, and the other studies29,36,37 described that no significant differences existed in complication rates after OWHTO relative to patient age at the time of surgery. Thus, it remains controversial whether patient age is a significant factor related to the clinical outcomes in regression analyses. However, the mean age of the patients included in 3 of these studies7,36,37 ranged from 44 to 55 years. In contrast, the mean age of the patients in the present study was 61.6 years. Thus, the patients in the other studies may have been too young to assess the effects of age on clinical outcomes after OWHTO. We believe that, compared with the studies discussed above, the range of patient age in the present study was wide enough to more accurately analyze these effects.
Limitations
There were some limitations in the present study. First, this was a retrospective, nonrandomized, cohort study. Second, the follow-up period ranged from 3 to 11 years, with a mean of 5.1 years. Therefore, this study cannot refer to the long-term follow-up results. Third, there were significant differences (P < .001) in the bilateral knee ratio among the 3 groups. Operating on both sides can affect the results. Fourth, a fundamental approach to the benefits of HTO rather than TKA is needed for patients >70 years of age. However, we did not evaluate the clinical outcome for patients >70 years of age in this study. Fifth, we did not measure muscle strength between each group before and after surgery in this study. Despite these limitations, we believe that this study provides important clinical information when considering the indication of OWHTO for older patients.
Conclusion
There were no significant differences in the mean 5-year follow-up clinical outcomes after OWHTO among the 3 groups. The study findings suggest that the age of patients does not affect the clinical and radiological outcomes after OWHTO.
Footnotes
Acknowledgements
The authors appreciate Professor Emeritus Howard Tarnoff for his English proofreading.
Final revision submitted May 5, 2023; accepted May 19, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hokkaido University Hospital (reference No. 018-0213).