
Abstract
Background:
Lateral epicondylitis (LE) is commonly treated with corticosteroid injections, which may lead to atrophy of the skin and subcutaneous fat. Surgical intervention becomes necessary in refractory cases, yet the optimal approach in patients with injection-induced soft tissue atrophy remains unclear.
Hypothesis/Purpose:
This study aimed to compare clinical outcomes and wound-related complications between arthroscopic and open extensor tendon release in patients with LE complicated by corticosteroid-induced soft tissue atrophy. It was hypothesized that the arthroscopic technique would result in superior outcomes and fewer wound-related complications.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively reviewed a prospectively collected database of patients who underwent arthroscopic or open extensor tendon release for LE between 2018 and 2024. Inclusion criteria were refractory LE for ≥6 months, visible corticosteroid-related skin and subcutaneous atrophy, and ≥12 months of follow-up. Patients with previous elbow surgery or additional pathologies were excluded. Functional outcomes (Mayo Elbow Performance Score [MEPS] and Quick Disabilities of the Arm, Shoulder and Hand [QuickDASH]) and complication rates were compared.
Results:
In total, 59 patients were included (arthroscopic: n = 32; open: n = 27). Preoperative demographics and scores were similar between groups (P≥ .272). At a mean 44-month follow-up, the arthroscopic group showed significantly better postoperative MEPS (91.4 ± 3.6 vs 88.8 ± 3.8, P = .009) and QuickDASH scores (14.4 ± 6.4 vs 20.4 ± 9.6, P = .006). Minimal clinically important difference, substantial clinical benefit, and patient acceptable symptom state thresholds were met by a significantly greater proportion of patients in the arthroscopic group across both scoring systems. Wound-related complications occurred in 4 open cases versus none in the arthroscopic group (P = .039). Poor clinical outcomes were more frequent in the open group, although not statistically significant (P = .084).
Conclusion:
Arthroscopic release provided superior functional outcomes and significantly fewer wound complications compared to open surgery in patients with LE who have corticosteroid-induced soft tissue atrophy.
Keywords
Commonly referred to as tennis elbow, lateral epicondylitis (LE) is the most prevalent enthesopathy of the upper extremity and typically results from repetitive microtrauma at the origin of the extensor carpi radialis brevis (ECRB). 18 Despite its straightforward clinical diagnosis and the wide range of available treatment options, this condition continues to impair patients’ quality of life. 9 Conservative management, including rest, nonsteroidal anti-inflammatory drugs, bracing, and physiotherapy, is effective for most individuals. 23 However, approximately 5% to 10% of patients with LE remain symptomatic after 6 months of nonoperative treatment and may require surgical intervention. 4 Although concomitant pathologies have been investigated in patients with LE who do not respond to conservative therapy, an alternative cause is often not identified. 3
Corticosteroid injection is still a commonly used first-line intervention for pain relief in patients with refractory LE.13,21 While these injections may provide short-term symptom improvement, their use has been associated with negative long-term clinical outcomes, with clinical deterioration seen within 6 months to 1 year following corticosteroid treatment.5,7 Moreover, repeated corticosteroid injections are associated with local adverse effects such as hypopigmentation, tendon degeneration, and atrophy of the skin and subcutaneous tissues.15,25 Soft tissue atrophy is not exceedingly rare, as some reports have indicated an incidence as high as 7.6%, yet it is often underappreciated in clinical decision-making. 21 Given the compromised condition of the skin and soft tissue, one might expect some challenges when surgery is required, particularly in terms of wound healing and postoperative complications.
Surgical treatment of LE primarily involves releasing and debriding the diseased ECRB tendon. The 2 main approaches, open and arthroscopic, offer distinct advantages and disadvantages.4,17 Open release provides direct visualization and procedural simplicity but requires a larger incision and more extensive dissection. 4 Arthroscopic release is technically more demanding but is minimally invasive, allows for intra-articular evaluation, and has been associated with faster recovery in some studies. 19 Although both techniques have demonstrated satisfactory functional outcomes in the general LE population, the optimal surgical strategy for patients with corticosteroid-associated soft tissue atrophy remains unclear.
Therefore, the aim of this study was to compare functional outcomes and complication rates between arthroscopic and open tendon release in patients with LE who have soft tissue atrophy secondary to repeated corticosteroid injections. It was hypothesized that patients undergoing arthroscopic release would exhibit superior clinical outcomes and fewer wound-related complications compared to those treated with the open technique.
Methods
Since 2018, the clinical and radiographic data of all adults who underwent surgical treatment for LE at our institution have been prospectively recorded in an institutional database after written consent was obtained. In this study, patients who underwent surgical treatment for LE between 2018 and 2024 were retrospectively evaluated. Specifically, those who developed skin and subcutaneous tissue atrophy secondary to repeated corticosteroid injections and underwent either open or arthroscopic extensor tendon release were considered for this retrospective comparative study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the institutional review board.
Patient Selection
The inclusion criteria for the study were as follows: (1) a clinical diagnosis of LE (a diagnosis made based on clinical examination, consisting of activity-related pain, palpable tenderness, and pain provoked just underneath the lateral epicondyle at the origin of the wrist extensors, with a positive Cozen's or chair test); (2) no response to at least 6 months of conservative treatment; (3) the presence of significant skin and subcutaneous tissue atrophy secondary to corticosteroid injections, confirmed through clinical examination and photographic documentation (Figure 1); and (4) a minimum postoperative follow-up period of 12 months. Patients with soft tissue atrophy, confirmed independently by two blinded orthopaedic specialists not involved in the study and documented in the surgical notes, were included in the study. Patients who had previously undergone elbow surgery on the same extremity and those with insufficient documentation, chondral or osteochondral lesions, obvious instability demonstrated by clinical examination and radiological findings, advanced osteoarthritis, or intra-articular loose bodies were excluded from the study.

Representative clinical preoperative figure of corticosteroid-induced skin and subcutaneous tissue atrophy.
Patients were divided into 2 groups based on whether they underwent an arthroscopic or an open procedure. No specific algorithm was followed in determining the surgical method; rather, the choice of technique depended on the operating surgeon. Open procedures were performed by a surgeon with expertise in open techniques, whereas arthroscopic procedures were performed by a surgeon specializing in arthroscopy. Both surgeons were fellowship-trained orthopaedic surgeons with at least 5 years of experience.
Outcome Measures
Preoperative assessment included demographic data (age, sex, affected side, body mass index [BMI]), duration of symptoms, the Mayo Elbow Performance Score (MEPS), and the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score. Postoperative clinical outcomes were evaluated using the same functional scoring systems at final follow-up. Complications were systematically recorded in both groups, with particular attention to wound-related issues, infections, reoperations, and recurrences.
Surgical Technique
Arthroscopic Procedure
The patient was placed in the lateral decubitus position, and the upper extremity was supported and operated on. All patients were operated under general anesthesia, and no regional block was used. A tourniquet was used routinely. The joint was inflated with saline solution introduced through the soft spot until sufficient capsular tension was achieved, which moved the neurovascular structures forward and allowed a more controlled entry of the arthroscope. The first portal, the proximal anteromedial imaging portal, was placed approximately 2 cm proximal to the epitrochlea and 1 cm anterior to the intermuscular septum. The proximal anterolateral portal was then created with a sharp scalpel under visual control from the medial portal, and a small capsulotomy was first performed with a scalpel. Then, the debridement of the intra-articular synovium was performed with a shaver through the lateral portal. All patients were routinely investigated for signs of instability, ensuring that there was no additional instability. A limited capsulectomy was carried out, carefully avoiding disruption of the anterior margin of the ECRB tendon and the posterior line extending between the radial head and the capitellum. The pathological ECRB origin was debrided near its insertion on the lateral epicondyle. Degenerated, dull-appearing tendon tissue was excised, while intact, glistening tendon fibers were meticulously preserved. The direct anterolateral portal was used for common extensor tenotomy. To prevent injury to the lateral collateral ligament, care was taken to stay in front of the bisector of the radial head with the elbow at 90° during radiofrequency and shaver release. The bone tissue was debrided with a shaver until bleeding was observed. The portals were closed with a simple suture, and the arm was bandaged.
Open Procedure
Open surgery was performed under general anesthesia in all patients, with the patient in the supine position. A tourniquet was routinely used. A slightly curved incision approximately 4 cm in length was made directly over the lateral epicondyle. The extensor origin was exposed, divided transversely close to its attachment at the lateral epicondyle, and allowed to retract distally. The degenerated or partially torn ECRB tendon origin was debrided of any calcification and dull fibrin deposits. Then, the joint capsule was released together with the extensor origin, and a small incision was made through the synovial membrane, allowing visualization of the joint. Bone spurs on the ridge and the thickened and avascular cortex on the lateral epicondyle were removed with a rongeur. The subcutaneous tissue and skin were sutured, and a compression bandage was applied.
Rehabilitation
Patients in both groups were advised to wear a sling for comfort for 2 weeks. The duration of sling use and the entire rehabilitation process were the same for both groups and included active range of motion from the first day after surgery and formal physical therapy beginning 10 to 14 days after surgery. A return to full activity was permitted to the extent that it was tolerated. In both groups, patients were advised to avoid heavy or repetitive hand work for 4 to 6 weeks.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (SPSS). Continuous variables were presented as mean ± standard deviation and categorical variables as frequencies and percentages. The normality of continuous variables was assessed using the Shapiro-Wilk test.
Previously established values for the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and patient acceptable symptom state (PASS) for QuickDASH and MEPS were used to interpret functional outcome scores. For MEPS, an MCID of 4.2 reported by Yao et al 24 in patients with LE was preferred over the 12.2 value described by Sun et al 20 for elbow stiffness. Reference values for MEPS also included an SCB of 17.3 and a PASS of 75, assessed in patients with elbow stiffness and elbow osteoarthritis.11,20 For the QuickDASH score, an MCID of 5.3 (elbow trauma) and SCB and PASS values of 16.9 and 15.9, respectively (from hand surgery data), were applied.8,16 Patients with a postoperative MEPS score <60 were categorized as having a poor clinical outcome, consistent with standard interpretation of the MEPS scale.
Between-group comparisons of continuous variables, including age, BMI, number of injections, follow-up duration, and both pre- and postoperative MEPS and QuickDASH scores, were performed using the independent samples t test. For categorical variables, including sex, dominant side, smoking status, wound-related complications, and poor clinical outcomes, the Fisher exact test was used because of small expected cell counts.
All tests were 2-tailed, and P≤ .05 was considered statistically significant.
Results
During the study period, 347 patients underwent surgical treatment for LE at our institution. Among them, 67 patients (19.3%) had soft tissue atrophy. Two patients were lost to follow-up, 2 patients had insufficient documentation, and 4 patients who underwent lateral collateral ligament imbrication (n = 2) or reconstruction (n = 2) for instability were excluded. In the 4 patients excluded because of instability, the diagnosis was made based on preoperative clinical examination in 2, whereas the other 2 patients were identified as unstable intraoperatively during arthroscopic assessment.
This resulted in a study cohort of 59 patients (56% women) with a mean follow-up of 44 months (range, 22-64 months). Of these, 32 patients underwent arthroscopic release, and 27 patients underwent open release. Baseline demographics and functional scores were comparable between groups (Table 1).
Preoperative Patient Demographics and Baseline Scores a

Values are presented as mean ± standard deviation unless otherwise indicated. BMI, body mass index; MEPS, Mayo Elbow Performance Score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand.
P < .05 was considered statistically significant.
In the entire study cohort, the mean preoperative MEPS of 61.2 ± 7.7 and QuickDASH of 67.1 ± 15.6 improved to 90.3 ± 3.7 and 16.8 ± 7.8 at the latest follow-up, respectively (P < .001). At final follow-up, both groups demonstrated improvement in functional scores compared to preoperative values (Table 2). The mean postoperative MEPS score of 91.4 ± 3.6 was higher in the arthroscopic group compared to the mean postoperative MEPS score of 88.8 ± 3.8 in the open group (P = .009) (Table 2). Similarly, the mean postoperative QuickDASH score of 14.4 ± 6.4 was better in the arthroscopic group than the mean postoperative value of 20.4 ± 9.6 in the open group (P = .006).
Clinical Outcomes and Functional Scores a

Values are presented as mean ± standard deviation unless otherwise indicated. MEPS, Mayo Elbow Performance Score; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand.
P < .05 was considered statistically significant. Bold values indicate statistically significant results (p < 0.05).
A poor clinical outcome was observed in 1 patient (3%) in the arthroscopic group and 6 patients (22%) in the open surgery group. Although this difference did not reach statistical significance (P = .084), there was a trend favoring the arthroscopic approach in terms of fewer unsatisfactory outcomes (Table 2).
For the MEPS score, all patients in the arthroscopic group (32/32, 100%) achieved the MCID, compared to 22 of 27 patients (81.5%) in the open surgery group (P = .016). Similarly, SCB for MEPS was achieved in 31 of 32 patients (96.9%) in the arthroscopic group and 19 of 27 patients (70.4%) in the open group (P = .008). In terms of PASS, the arthroscopic group again demonstrated significantly higher rates (29/32, 90.6%) compared to the open group (18/27, 66.7%) (P = .048).
For the QuickDASH score, all patients in the arthroscopic group (32/32, 100%) achieved the MCID, compared to 25 of 27 patients (92.6%) in the open group (P = .205). SCB was met in 31 of 32 arthroscopic patients (96.9%) and in 21 of 27 open surgery patients (77.8%) (P = .040). However, the difference in PASS rates for QuickDASH, although favoring the arthroscopic group (20/32, 62.5%) over the open group (11/27, 40.7%), did not reach statistical significance (P = .121) (Table 3).
Threshold-Based Comparison of Outcome Parameters Between Arthroscopic and Open Surgery Groups a

MCID, minimal clinically important difference; MEPS, Mayo Elbow Performance Score; PASS, patient acceptable symptom state; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand; SCB, substantial clinical benefit.
P < .05 was considered statistically significant. Bold values indicate statistically significant results (p < 0.05).
Complications
In the open surgery group, 4 patients (15%) experienced wound-related complications. Among these, 2 patients experienced wound dehiscence, 1 patient developed a superficial surgical site infection managed with oral antibiotics, and 1 patient had a deep infection requiring surgical debridement. Two patients who developed wound complications in the open surgery group underwent reoperation within the first 6 months due to recurrent symptoms. In addition, 1 patient was followed up with wound care and left to heal secondarily. A poor outcome was found in 3 patients with wound-related complications. No wound complications or reoperations were observed in the arthroscopic group, resulting in a significantly higher complication rate in the open surgery group (P = .039; Table 4).
Complications and Reoperations by Group
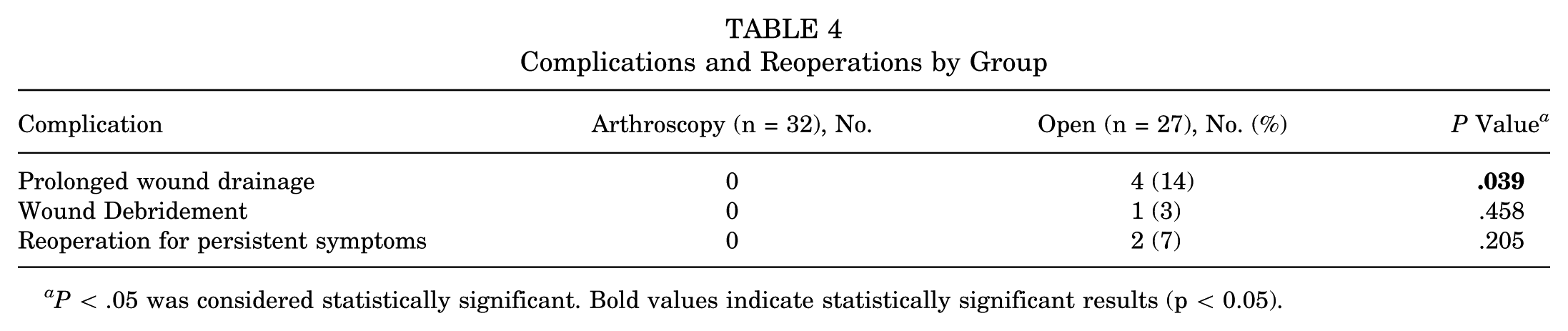
P < .05 was considered statistically significant. Bold values indicate statistically significant results (p < 0.05).
Discussion
This study compared the functional outcomes and complication rates of arthroscopic versus open extensor tendon release in patients with LE with corticosteroid-induced skin and subcutaneous tissue atrophy. The main finding of this study is that, while both techniques resulted in significant functional improvement, the arthroscopic approach was associated with higher postoperative MEPS scores, better QuickDASH scores, and fewer wound-related complications. These findings highlight the surgical challenges that can be encountered in this specific subgroup of patients when treated with an open procedure and suggest that arthroscopic release may be the preferred technique for this patient group, given its favorable functional outcomes while minimizing wound-related complications.
Although some authors found a faster recovery after arthroscopic release, most studies have reported comparable clinical outcomes and complication rates for both open and arthroscopic techniques in the general LE population.4,13,19,26 Our findings are consistent with those studies in terms of functional recovery, as both surgical techniques demonstrated satisfactory functional results, with most patients achieving an MCID and SCB, supporting both surgical techniques for the treatment of chronic LE. Significant differences in functional outcome were observed between the 2 groups. The MCID of 5.3 for QuickDASH was exceeded between groups in favor of arthroscopic treatment, whereas the MCID of 4.2 for MEPS was not. Additionally, a greater proportion of patients in the arthroscopic group reached MCID, SCB, and PASS (Table 3). Overall, most analyses addressing functional outcome favored arthroscopic treatment, although the observed differences did not always achieve clinically important cutoffs. Therefore, the found differences in functional outcomes between techniques may be marginal.
Delayed or impaired wound healing is a known concern in patients with corticosteroid-induced skin and subcutaneous tissue atrophy. Corticosteroids reduce the number of local adipocytes, fibroblast activity, and collagen synthesis, which can compromise the integrity and regenerative capacity of soft tissue.6,22 Additionally, dermal and epidermal atrophy is associated with increased fragility of the skin because of elasticity loss, affecting the skin barrier integrity. 14 In our cohort, wound-related complications, including prolonged drainage and need for reoperation, were observed exclusively in the open surgery group. While the study design limits definitive causal conclusions, we hypothesize that atrophic tissue, when further disrupted by open dissection, may be more vulnerable to complications during healing. Given that arthroscopic release requires smaller incisions and minimizes subcutaneous undermining, it may represent a safer alternative for patients with preexisting steroid-related compromised soft tissue, as minimizing surgical trauma is likely to be favorable regarding wound healing.
A systematic review by Kholinne et al 10 highlighted that repeated corticosteroid injections are a potential contributor to underlying soft tissue compromise and elbow instability, particularly posterolateral rotatory instability. Their findings emphasize the importance of a thorough preoperative evaluation for ligamentous insufficiency, especially in patients with a history of multiple injections. To keep the cohort as homogeneous as possible, patients with clinically and radiologically evident instability were excluded from our study. All patients were routinely evaluated with the posterior drawer test and pivot-shift test. However, Arrigoni et al 2 described intra-articular findings related to symptomatic minor instability of the lateral elbow, which are best diagnosed arthroscopically, as clinical examination may not reliably detect them. From this perspective, arthroscopic treatment for LE may allow the identification and management of these findings using fully arthroscopic techniques, offering an additional advantage over open procedures in this specific patient group. 1
Recently, an arthroscopic suture anchor repair technique has shown promising results with favorable outcomes compared to an isolated arthroscopic debridement technique. 24 The additional repair led to clinically important superior results in QuickDASH and MEPS, while visual analog scores at rest and during activity remained similar. Given that the favorable functional scores might be attributed to recovery of extension strength, an additional evaluation of grip and extension strength seems warranted. Because of the retrospective design, quantitative evaluation of grip and extension strength was not possible in our study, representing a limitation of the study. The proposed subcutaneous extracapsular suture repair technique proved to be safe for the general LE population. In our patient cohort, this technique might be more challenging, as the atrophic skin and surrounding soft tissue might be violated, and the suture material might be more prominent underneath the thin and vulnerable skin, potentially leading to additional problems. Therefore, the feasibility and safety of this technique still have to be proved for the specific subgroup of patients studied in our study.
The retrospective study design has inherent limitations. Treatment allocation was not randomized but based on surgeon preference, introducing potential selection bias. However, the comparable baseline characteristics between groups mitigate some of these shortcomings. Since there is no grading system for assessing soft tissue atrophy, the degree of soft tissue atrophy may differ between patients. The subjective evaluation of atrophy may affect the results. Although we have data on the number of steroid injections administered to patients, we do not have data on which corticosteroid derivative was administered at what dose. This limits our ability to draw conclusions about dose-dependent effects. This study included only 59 patients, making it a small study cohort despite exceeding the previously described minimum of 23 patients in each group. 12 Nonetheless, to our knowledge, this is the first study to directly compare surgical techniques in patients with corticosteroid-induced skin and subcutaneous tissue atrophy. Moreover, most of the MCID, SCB, and PASS cutoffs used were derived from other pathologies, representing an additional limitation of the study.
Conclusion
In patients with LE complicated by skin and subcutaneous tissue atrophy from repeated corticosteroid injections, both open and arthroscopic extensor tendon release yielded significant improvements in functional outcome. The arthroscopic technique was associated with small yet distinct differences in functional outcome, favoring this approach. More importantly, wound-related complications were less frequent in the arthroscopic group. These findings suggest that arthroscopic release may offer both functional advantages and a reduced risk of wound complications in this specific patient subgroup.
Footnotes
Final revision submitted July 1, 2025; accepted November 7, 2025.
Presented at the 2024 SECEC Congress Munich.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
The University of Health Sciences, Baltalimani Bone Diseases Training and Research Hospital Institutional Review Board approved the study protocol (App no:35/256).
ORCID iDs
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions and patient confidentiality. However, deidentified data may be available from the corresponding author upon reasonable request and with approval of the institutional ethics committee.